You might also like
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Exercise and Diabetes: A Clinician's Guide to Prescribing Physical ActivityFrom EverandExercise and Diabetes: A Clinician's Guide to Prescribing Physical ActivityNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Medical Encyclopedia XXL: Prof. J.P. Schadé, M.D., Ph.D. D.Sc.hcFrom EverandMedical Encyclopedia XXL: Prof. J.P. Schadé, M.D., Ph.D. D.Sc.hcNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- CoxsackievirusDocument14 pagesCoxsackievirusAndrés Gordillo100% (1)
- VACAMDocument43 pagesVACAMEstudiando SaluddNo ratings yet
- Les 387 Notions Qui TombentDocument26 pagesLes 387 Notions Qui TombentAymen SalemNo ratings yet
- Hypoglycemia, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandHypoglycemia, A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- (E-BOOK ITA) - Respirazione-Esercizi ZenDocument11 pages(E-BOOK ITA) - Respirazione-Esercizi ZenAndrea C. BiffiNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Diabetes Diet Plan: Diabetic Diet Guidelines for Curing Diabetes and Lose Weight Naturally. (Diabetes Diet Cookbook and Recipes to Prevent Diabetes, Boost Metabolism , Diabetes Treatment, Diabetes TipFrom EverandDiabetes Diet Plan: Diabetic Diet Guidelines for Curing Diabetes and Lose Weight Naturally. (Diabetes Diet Cookbook and Recipes to Prevent Diabetes, Boost Metabolism , Diabetes Treatment, Diabetes TipNo ratings yet
- Practical Insulin: A Handbook for Prescribing ProvidersFrom EverandPractical Insulin: A Handbook for Prescribing ProvidersRating: 5 out of 5 stars5/5 (2)
- Meditations & Confessions For Health and Healing - by John OsteenDocument3 pagesMeditations & Confessions For Health and Healing - by John OsteenwondimuNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Stres Oksydacyjny PDFDocument3 pagesStres Oksydacyjny PDFMarekDereżyńskiNo ratings yet
- Smoothies for Diabetics: Reverse Diabetes and Lower Blood Sugar with 36 Quick & Easy Delicious Diabetic Smoothie RecipesFrom EverandSmoothies for Diabetics: Reverse Diabetes and Lower Blood Sugar with 36 Quick & Easy Delicious Diabetic Smoothie RecipesRating: 5 out of 5 stars5/5 (2)
- Naplex Complete Study Outline A Topic-Wise Approach DiabetesFrom EverandNaplex Complete Study Outline A Topic-Wise Approach DiabetesRating: 4 out of 5 stars4/5 (2)
- Fatty Liver Diet: A 3-Week Step-by-Step Guide for Women Over 50From EverandFatty Liver Diet: A 3-Week Step-by-Step Guide for Women Over 50No ratings yet
- 12 Habits that Control Blood Sugar and Reverse PrediabetesFrom Everand12 Habits that Control Blood Sugar and Reverse PrediabetesRating: 5 out of 5 stars5/5 (1)
- Insulin Resistance Eating Plan: A Beginner's 2-Week Step-by-Step Guide for Women to Manage PCOS and Prediabetes, With Sample Curated RecipesFrom EverandInsulin Resistance Eating Plan: A Beginner's 2-Week Step-by-Step Guide for Women to Manage PCOS and Prediabetes, With Sample Curated RecipesNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Diabete: Weight Loss and Exercise: The most important information you need to improve your healthFrom EverandDiabete: Weight Loss and Exercise: The most important information you need to improve your healthNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Diabetes Ready Reference for Nurse Practitioners: Clear, Concise Guidelines for Effective Patient CareFrom EverandDiabetes Ready Reference for Nurse Practitioners: Clear, Concise Guidelines for Effective Patient CareNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5807)
- Exame Neurológco Do Recém-Nascido A TermoDocument25 pagesExame Neurológco Do Recém-Nascido A TermojucavaletiNo ratings yet
- Gastric Sleeve Cookbook: Fluid and Puree: Effortless Bariatric Cooking, #1From EverandGastric Sleeve Cookbook: Fluid and Puree: Effortless Bariatric Cooking, #1Rating: 4 out of 5 stars4/5 (2)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Diabetic Recipes for One and TwoFrom EverandDiabetic Recipes for One and TwoRating: 3 out of 5 stars3/5 (1)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Summary & Study Guide - The End of Diabetes: The Eat to Live Plan to Prevent and Reverse Diabetes - Including Diet Cheat SheetFrom EverandSummary & Study Guide - The End of Diabetes: The Eat to Live Plan to Prevent and Reverse Diabetes - Including Diet Cheat SheetNo ratings yet
- Escala de Actitudes Disfuncionales DAS (A)Document4 pagesEscala de Actitudes Disfuncionales DAS (A)rosamcamanezNo ratings yet
- Handbook of Drug Interaction and the Mechanism of InteractionFrom EverandHandbook of Drug Interaction and the Mechanism of InteractionRating: 1 out of 5 stars1/5 (1)
- Frontiers in Clinical Drug Research - Diabetes and Obesity: Volume 2From EverandFrontiers in Clinical Drug Research - Diabetes and Obesity: Volume 2No ratings yet
- Prediabetes: A Fundamental Text: Pathophysiology, Complications, Management & ReversalFrom EverandPrediabetes: A Fundamental Text: Pathophysiology, Complications, Management & ReversalNo ratings yet
- Ketogenic Diet "Yes & No" Guide For BeginnersFrom EverandKetogenic Diet "Yes & No" Guide For BeginnersRating: 3 out of 5 stars3/5 (1)
- Fatty Liver Solution: A Beginner’s Quick Start Guide on Naturally Managing Fatty Liver Disease Through NutritionFrom EverandFatty Liver Solution: A Beginner’s Quick Start Guide on Naturally Managing Fatty Liver Disease Through NutritionNo ratings yet
- Breaking the Chains of Diabetes. A Comprehensive Guide to Understanding and Managing Diabetes NaturallyFrom EverandBreaking the Chains of Diabetes. A Comprehensive Guide to Understanding and Managing Diabetes NaturallyNo ratings yet
- High Triglycerides Diet: A Beginner's 3-Week Step-by-Step Guide With Curated Recipes and a 7-Day Meal PlanFrom EverandHigh Triglycerides Diet: A Beginner's 3-Week Step-by-Step Guide With Curated Recipes and a 7-Day Meal PlanNo ratings yet
- Fatty Liver Disease Diet: A Beginner's Step-by-Step Guide with Recipes and a Meal PlanFrom EverandFatty Liver Disease Diet: A Beginner's Step-by-Step Guide with Recipes and a Meal PlanNo ratings yet
- Protein Power: Effortless Strategies to Boost Protein Intake With GLP-1 AgonistsFrom EverandProtein Power: Effortless Strategies to Boost Protein Intake With GLP-1 AgonistsNo ratings yet
- Conquering Diabetes: Fenugreek Success in Regulating Blood Sugar LevelsFrom EverandConquering Diabetes: Fenugreek Success in Regulating Blood Sugar LevelsNo ratings yet
- Type 1 Diabetes Diet Demystified: Simple and Tasty Recipes for Managing Your Blood Sugar with ConfidenceFrom EverandType 1 Diabetes Diet Demystified: Simple and Tasty Recipes for Managing Your Blood Sugar with ConfidenceNo ratings yet
- Fatty Liver Detox Cleanse: A Beginner's 3-Week Step-by-Step Guide to Managing Fatty Liver Symptoms Including Fatigue with Recipes and a Meal PlanFrom EverandFatty Liver Detox Cleanse: A Beginner's 3-Week Step-by-Step Guide to Managing Fatty Liver Symptoms Including Fatigue with Recipes and a Meal PlanNo ratings yet
- The Type 2 Diabetes Cookbook: Quick and Easy Recipes for a Healthy LifestyleFrom EverandThe Type 2 Diabetes Cookbook: Quick and Easy Recipes for a Healthy LifestyleNo ratings yet
- Metabolic Syndrome: Underlying Mechanisms and Drug TherapiesFrom EverandMetabolic Syndrome: Underlying Mechanisms and Drug TherapiesMinghan WangNo ratings yet
- Ultimate Diet Plan for Diabetic Patients: Revolutionizing Diabetic NutritionFrom EverandUltimate Diet Plan for Diabetic Patients: Revolutionizing Diabetic NutritionNo ratings yet
- Pupilometro. Practica. Angel MendezDocument4 pagesPupilometro. Practica. Angel MendezAngelxxx MendezzzNo ratings yet
- NURS 2710 Tarea 2.2Document10 pagesNURS 2710 Tarea 2.2johnmaster2010No ratings yet
- Actividad Sesión 13de Abril 2021 Sistema RespiratorioDocument3 pagesActividad Sesión 13de Abril 2021 Sistema RespiratorioFabiola RosalesNo ratings yet
- Cuadro EnterobacteriaDocument2 pagesCuadro EnterobacteriaSamuel May100% (3)
- Exposición de Transmisión VerticalDocument11 pagesExposición de Transmisión VerticalAngie Meza NúñezNo ratings yet
- Transferencia NeuróticaDocument7 pagesTransferencia NeuróticaFedericoRodriguezNo ratings yet
- Clínica de Plantas Versión: 1 Última Actualización: 19/10/14 Elaborado Por: Juan Camilo Garzón León Revisado Por: Sandra Gómez Aprobado PorDocument16 pagesClínica de Plantas Versión: 1 Última Actualización: 19/10/14 Elaborado Por: Juan Camilo Garzón León Revisado Por: Sandra Gómez Aprobado PorJohan Sebastian Ramirez VanegasNo ratings yet
- FichaDocument2 pagesFichaVictor CarrilloNo ratings yet
- Processo Seletivo 2023 Medicina ProvaDocument27 pagesProcesso Seletivo 2023 Medicina ProvaFernandaOliveiraNo ratings yet
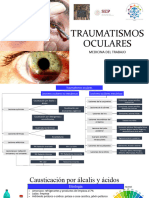
- Traumatismos OcularesDocument30 pagesTraumatismos OcularesTanisha uwuNo ratings yet
- ModeloDocument45 pagesModeloAida Campomanes TarazonaNo ratings yet
- Formato de Control de TemperaturaDocument3 pagesFormato de Control de Temperaturajhan betanNo ratings yet
- Encéphalomyopathies MitochondrialesDocument13 pagesEncéphalomyopathies MitochondrialesaissaNo ratings yet
- A Comprehensive Review and Evaluation of in Vitro Antifungal Potential of Rauvolfia SerpentinaDocument14 pagesA Comprehensive Review and Evaluation of in Vitro Antifungal Potential of Rauvolfia SerpentinaIJRASETPublicationsNo ratings yet
- Belleza de La Piel PDFDocument5 pagesBelleza de La Piel PDFAntónio João Lacerda VieiraNo ratings yet
- Atividade Contextualizada-Estágio Supervisionado 1Document3 pagesAtividade Contextualizada-Estágio Supervisionado 1Helen Cristina De Sena RochaNo ratings yet
- Turnitin SkripsiDocument65 pagesTurnitin Skripsisevty agustinNo ratings yet
- Bloqueio AnestesicoDocument7 pagesBloqueio AnestesicoBreno SampaioNo ratings yet
- Cancer Case StudyDocument3 pagesCancer Case Studyapi-311163159No ratings yet
- E ColiDocument17 pagesE Coliisna nurul dukhaNo ratings yet
- City Government of Kabankalan: State Protect TheDocument2 pagesCity Government of Kabankalan: State Protect ThefortunecNo ratings yet
- Valoración Neurológica CompletaDocument44 pagesValoración Neurológica CompletaEduardoNo ratings yet