You might also like
- Sodium Fluoride PET/CT in Clinical UseFrom EverandSodium Fluoride PET/CT in Clinical UseKalevi KairemoNo ratings yet
- Pet CT and Pet Mri in Head and Neck MalignancyDocument10 pagesPet CT and Pet Mri in Head and Neck MalignancyAndrés Faúndez TeránNo ratings yet
- Lung Cancer Investigation and Staging GuideDocument8 pagesLung Cancer Investigation and Staging GuideCarlos MichasNo ratings yet
- Role of FDG PET/CT in Detecting Unknown Primary CancersDocument14 pagesRole of FDG PET/CT in Detecting Unknown Primary CancersDeivid Ruidiazz GmezzNo ratings yet
- Clinical Impact of FDG PET-CT On Management Decisions For Patients With Primary Biliary TumoursDocument10 pagesClinical Impact of FDG PET-CT On Management Decisions For Patients With Primary Biliary TumourslkitkatgirlNo ratings yet
- Daisne 2004Document8 pagesDaisne 2004alinaNo ratings yet
- 2010 Article 22Document16 pages2010 Article 22Andreas KrishnaputraNo ratings yet
- MainDocument8 pagesMainNurulrezki AtikaNo ratings yet
- PET-CT in Unknown Primary CancerDocument22 pagesPET-CT in Unknown Primary CancerCesar Caldas ValdezNo ratings yet
- Imaging characteristics predict NPC metastasisDocument7 pagesImaging characteristics predict NPC metastasisJose JulianNo ratings yet
- Del Beke 2004Document7 pagesDel Beke 2004nitsuga oneNo ratings yet
- FDG PET CT in Testicular CancerDocument4 pagesFDG PET CT in Testicular CancerlkitkatgirlNo ratings yet
- Contemporary Approach To The Diagnosis of Malignant Pleural EffusionDocument8 pagesContemporary Approach To The Diagnosis of Malignant Pleural EffusionranityaindraNo ratings yet
- jnm046045 1920.Document3 pagesjnm046045 1920.Rahul KashyapNo ratings yet
- Accuracy of 18FFDG PETCT in Detection and Restaging of Recurrent Ovarian CancerDocument7 pagesAccuracy of 18FFDG PETCT in Detection and Restaging of Recurrent Ovarian CancerHana SalemNo ratings yet
- Pet Scan en Ca de TiroidesDocument9 pagesPet Scan en Ca de TiroidesdrmolinammNo ratings yet
- PET-CT - SeminarDocument33 pagesPET-CT - SeminarSanjai NarayanasamyNo ratings yet
- Incidental Primary Breast Cancer Detected On PET-CTDocument8 pagesIncidental Primary Breast Cancer Detected On PET-CTMaxime PorcoNo ratings yet
- MARYLYN. Proposal Presentation. DraftDocument20 pagesMARYLYN. Proposal Presentation. DraftpriyyaNo ratings yet
- Editorial Surveillance in Testicular Cancer: Who, When, What and How?Document3 pagesEditorial Surveillance in Testicular Cancer: Who, When, What and How?Jocho NeavesNo ratings yet
- DX TX Cancer PulmonDocument13 pagesDX TX Cancer PulmonFernando AtenciaNo ratings yet
- Pet ScanDocument7 pagesPet ScanKranthikumar BobbillapatiNo ratings yet
- 279 FullDocument2 pages279 FullkirachidNo ratings yet
- 10 1053@j Semnuclmed 2020 07 005Document10 pages10 1053@j Semnuclmed 2020 07 005anon_813722240No ratings yet
- Theraphy RadDocument4 pagesTheraphy RadMega PuspitaNo ratings yet
- Jurnal Radiologi 2Document21 pagesJurnal Radiologi 2Adelya Dwi AsyifaNo ratings yet
- PET in OncologyDocument70 pagesPET in Oncologyg_daniel119974No ratings yet
- The Place of FDG PET CT in Renal Cell Carcinoma - Value and LimitationsDocument7 pagesThe Place of FDG PET CT in Renal Cell Carcinoma - Value and LimitationslkitkatgirlNo ratings yet
- Comparative Treatment Planning Study of Photons and ProtonsDocument15 pagesComparative Treatment Planning Study of Photons and ProtonsJesse Helmut Hansen-BartelNo ratings yet
- Towards Personalized Treatment For Prostate CancerDocument202 pagesTowards Personalized Treatment For Prostate CancerEduar Antonio Landazuri IdroboNo ratings yet
- Radiotherapy and OncologyDocument6 pagesRadiotherapy and OncologyIntan Kartika NursyahbaniNo ratings yet
- Surveillance of Hepatocellular Carcinoma with ImagingDocument16 pagesSurveillance of Hepatocellular Carcinoma with ImagingMahmoud AbouelsoudNo ratings yet
- Counter-Point: Are We Really Ordering Too Many CT Scans? - PMCDocument6 pagesCounter-Point: Are We Really Ordering Too Many CT Scans? - PMCMenna KhNo ratings yet
- Hallifax Radiological Investigation of Pleural DiseaseDocument38 pagesHallifax Radiological Investigation of Pleural Diseaselaila.forestaNo ratings yet
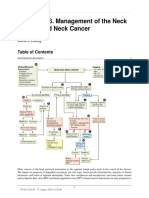
- Chapter 146. Management of The Neck in Head and Neck Cancer: David E EiblingDocument3 pagesChapter 146. Management of The Neck in Head and Neck Cancer: David E EiblingYasin KulaksızNo ratings yet
- Pet BrochureDocument20 pagesPet BrochureSheikh Hasnain AliNo ratings yet
- Clinical Practice Guidelines: Penile Cancer: ESMO Clinical Practice Guidelines For Diagnosis, Treatment and Follow-UpDocument10 pagesClinical Practice Guidelines: Penile Cancer: ESMO Clinical Practice Guidelines For Diagnosis, Treatment and Follow-Uphypebeast dopeNo ratings yet
- Surgical Management of Recurrent Nasopharyngeal Carcinoma: Sheng-Po Hao, MD, Facs, Fics Ngan-Ming Tsang, MD, DSCDocument9 pagesSurgical Management of Recurrent Nasopharyngeal Carcinoma: Sheng-Po Hao, MD, Facs, Fics Ngan-Ming Tsang, MD, DSCMirzaulin LeonaviriNo ratings yet
- ieee_tranDocument12 pagesieee_trankoushikraj900No ratings yet
- Young 2017Document7 pagesYoung 2017Rosi SurianiNo ratings yet
- Characterization of Adrenal Metastatic Cancer Using FDG PET CTDocument8 pagesCharacterization of Adrenal Metastatic Cancer Using FDG PET CTEngky ChristianNo ratings yet
- A Role of FDG-PET-CT For Response Evaluation in Metastatic Breast CancerDocument11 pagesA Role of FDG-PET-CT For Response Evaluation in Metastatic Breast CancerZuriNo ratings yet
- 521.fullDocument11 pages521.fullhafidisara05No ratings yet
- bfcr163 Pet-Ct PDFDocument34 pagesbfcr163 Pet-Ct PDFMirza BaigNo ratings yet
- Imaging Findings of Sinonasal TumorsDocument17 pagesImaging Findings of Sinonasal TumorstaufikolingNo ratings yet
- Article Oesophage CorrectionDocument11 pagesArticle Oesophage CorrectionKhalilSemlaliNo ratings yet
- DX Evaluation Lung Cancer - UpToDateDocument2 pagesDX Evaluation Lung Cancer - UpToDateashlyanna3173No ratings yet
- Management of The Solitary Pulmonary NoduleDocument6 pagesManagement of The Solitary Pulmonary Nodulevictor ibarra romeroNo ratings yet
- 1 s2.0 S1368837518304299 MainDocument8 pages1 s2.0 S1368837518304299 MainIgor VainerNo ratings yet
- Radioterapia en CacUDocument6 pagesRadioterapia en CacUVicente RamosNo ratings yet
- Giant Cell Tumour of Bone: A Demographic Study From A Tumour Unit in South AfricaDocument6 pagesGiant Cell Tumour of Bone: A Demographic Study From A Tumour Unit in South AfricaRadenSiwi Bagus HadhiningratNo ratings yet
- F-FDG PET CT As A Prognostic Factor in Hepatocellular CarcinomaDocument7 pagesF-FDG PET CT As A Prognostic Factor in Hepatocellular CarcinomaUvi Cancino RamosNo ratings yet
- Fluid Complications: Malignant Pleural EffusionDocument11 pagesFluid Complications: Malignant Pleural Effusiont4tranNo ratings yet
- Staging Cholangiocarcinoma by Imaging Studies: V. VilgrainDocument4 pagesStaging Cholangiocarcinoma by Imaging Studies: V. VilgrainNikos SerifisNo ratings yet
- 2019 Article 5894 PDFDocument8 pages2019 Article 5894 PDFGalgalo GarbichaNo ratings yet
- Austin Journal of Nuclear Medicine and RadiotherapyDocument5 pagesAustin Journal of Nuclear Medicine and RadiotherapyAustin Publishing GroupNo ratings yet
- AtomDocument13 pagesAtomapi-3821924No ratings yet
- CT Scan CA ColonDocument31 pagesCT Scan CA ColonNadia IndriNo ratings yet
- Thyroidcancer: Ultrasound Imaging and Fine-Needle Aspiration BiopsyDocument21 pagesThyroidcancer: Ultrasound Imaging and Fine-Needle Aspiration BiopsyPedro Gómez RNo ratings yet
- Pet ManejoDocument9 pagesPet ManejodrmolinammNo ratings yet
- E AvulsionDocument8 pagesE Avulsionbudi doremiNo ratings yet
- Nerve Injuries of The NeckDocument12 pagesNerve Injuries of The NeckAndrés Faúndez TeránNo ratings yet
- ANASTESIDocument30 pagesANASTESIaftinaaNo ratings yet
- The Early Secondary GingivoperiosteoplastyDocument11 pagesThe Early Secondary GingivoperiosteoplastyAndrés Faúndez TeránNo ratings yet
- Description and Evaluation of An Intraoral Cervical Plexus Anesthetic TechniqueDocument6 pagesDescription and Evaluation of An Intraoral Cervical Plexus Anesthetic TechniqueAndrés Faúndez TeránNo ratings yet
- Smas Face Lift AnatomyDocument5 pagesSmas Face Lift AnatomyJacob AlajyNo ratings yet
- Relaciones Anatomicas Intraoseas en Rama y Cuerpo Mandibular en La Tecnica de Osteotomia Sagital Mandibular ModificadaDocument7 pagesRelaciones Anatomicas Intraoseas en Rama y Cuerpo Mandibular en La Tecnica de Osteotomia Sagital Mandibular ModificadaAndrés Faúndez TeránNo ratings yet
- Masseter Muscle Reattachment After Mandibular Angle SurgeryDocument4 pagesMasseter Muscle Reattachment After Mandibular Angle Surgery洪侊增No ratings yet
- Anatomy of The SMAS RevisitedDocument8 pagesAnatomy of The SMAS RevisitedJoana AiresNo ratings yet
- Dr. Atif Sher ASCVD CardioConDocument21 pagesDr. Atif Sher ASCVD CardioConwali ahmedNo ratings yet
- X ENGLISH FINAlDocument12 pagesX ENGLISH FINAlRamNo ratings yet
- Tetanus Shots For Adults: Patient HandoutDocument1 pageTetanus Shots For Adults: Patient Handoutselvie87No ratings yet
- Infectious Diseases: CowpoxDocument3 pagesInfectious Diseases: CowpoxMohammedNo ratings yet
- ConditionalsDocument7 pagesConditionalsquynhnnp234101eNo ratings yet
- Diabetic Ketoacidosis and Hyperosmolar Hyperglycemic State GuideDocument26 pagesDiabetic Ketoacidosis and Hyperosmolar Hyperglycemic State GuideEleanorNo ratings yet
- ROTC Registration FormDocument2 pagesROTC Registration FormMJ Cortez PaguioNo ratings yet
- Annals of Medicine - HPV VaccineDocument12 pagesAnnals of Medicine - HPV VaccineJudicial Watch, Inc.100% (3)
- CHAPTER 2 Infectious EpidemiologyDocument89 pagesCHAPTER 2 Infectious EpidemiologyteklayNo ratings yet
- Compartment SyndromeDocument21 pagesCompartment SyndromeMiztaloges86100% (1)
- SUmmary of Clinical EfficacyDocument182 pagesSUmmary of Clinical EfficacyStacey Kreller100% (1)
- Vaccination Trends and Herd ImmunityDocument2 pagesVaccination Trends and Herd ImmunityYoshi NNo ratings yet
- Taub - Osteomyelitis of The Jaw A Retrospective AnalysisDocument7 pagesTaub - Osteomyelitis of The Jaw A Retrospective AnalysisChristopher McMullinNo ratings yet
- PSYC 1111-01 Written Assignment Unit 7Document4 pagesPSYC 1111-01 Written Assignment Unit 7Muftaudeen Yusuf BabatundeNo ratings yet
- Medication Administration and Asepsis ReviewDocument11 pagesMedication Administration and Asepsis ReviewÀi ZìjǐNo ratings yet
- Pytania AngielskiDocument4 pagesPytania AngielskiDementij ŻukówNo ratings yet
- DR Lal Pathlabs: LPL - Lpl-Rohini (National Reference Lab) Sector - 18, Block - E Rohini Delhi 110085Document2 pagesDR Lal Pathlabs: LPL - Lpl-Rohini (National Reference Lab) Sector - 18, Block - E Rohini Delhi 110085Vivek PatelNo ratings yet
- Medically Unexpl. Symptoms, Somatisation, Bodily Distress - F. Creed, Et. Al., (Cambridge, 2011) WWDocument267 pagesMedically Unexpl. Symptoms, Somatisation, Bodily Distress - F. Creed, Et. Al., (Cambridge, 2011) WWTommi JitaruNo ratings yet
- 2020 Image Challenge in Veterinary Pathology Answers Avian DiseasesDocument2 pages2020 Image Challenge in Veterinary Pathology Answers Avian DiseasesArub Muna NabilaNo ratings yet
- Pigeon Disease TreatmentsDocument1 pagePigeon Disease TreatmentsJohnMasive100% (1)
- Public Health History and InterventionsDocument5 pagesPublic Health History and InterventionsIzza KazandraNo ratings yet
- Rak Pluêa: Lung CarcinomaDocument12 pagesRak Pluêa: Lung Carcinomamiaamiaa4244No ratings yet
- Cn7 Palsy (Bells Palsy)Document5 pagesCn7 Palsy (Bells Palsy)Wande AyodeleNo ratings yet
- Oplisto Protocols For Emerging Infectious DiseaseDocument56 pagesOplisto Protocols For Emerging Infectious DiseaseYang RheaNo ratings yet
- ARI: Acute Respiratory Infection GuideDocument29 pagesARI: Acute Respiratory Infection GuideJam Knows RightNo ratings yet
- Uniprot IDs of spike proteins from coronaviruses and other virusesDocument8 pagesUniprot IDs of spike proteins from coronaviruses and other virusesPiyush RajNo ratings yet
- Deadly Ebola Virus IntroductionDocument14 pagesDeadly Ebola Virus IntroductionAli SyedNo ratings yet
- Carpal Tunnel Syndrome Questionnaire (CTSQ)Document1 pageCarpal Tunnel Syndrome Questionnaire (CTSQ)Samuel Iñiguez JiménezNo ratings yet
- Narotam 1994 KKDocument10 pagesNarotam 1994 KKFernandaPlatnerNo ratings yet
- Heart Failure DDx and WorkupDocument3 pagesHeart Failure DDx and WorkupAizel ManiagoNo ratings yet
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (14)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 3.5 out of 5 stars3.5/5 (2)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 5 out of 5 stars5/5 (4)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 5 out of 5 stars5/5 (5)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsFrom EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo ratings yet
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (327)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 3.5 out of 5 stars3.5/5 (33)
- Daniel Kahneman's "Thinking Fast and Slow": A Macat AnalysisFrom EverandDaniel Kahneman's "Thinking Fast and Slow": A Macat AnalysisRating: 3.5 out of 5 stars3.5/5 (130)
- Summary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisFrom EverandSummary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisRating: 5 out of 5 stars5/5 (3)