You might also like
- Research: Burden of Care Amongst Caregivers Who Are First Degree Relatives of Patients With SchizophreniaDocument10 pagesResearch: Burden of Care Amongst Caregivers Who Are First Degree Relatives of Patients With SchizophreniaLusiaNo ratings yet
- Original Article: Family Burden in Caregivers of Schizophrenia Patients: Prevalence and Socio Demographic CorrelatesDocument7 pagesOriginal Article: Family Burden in Caregivers of Schizophrenia Patients: Prevalence and Socio Demographic CorrelatesMUKESH KUMARNo ratings yet
- Adeosun, I. I. (2013) Correlates of Caregiver Burden Among Family Members of Patients With Schizophrenia in Lagos, NigeriaDocument7 pagesAdeosun, I. I. (2013) Correlates of Caregiver Burden Among Family Members of Patients With Schizophrenia in Lagos, NigeriaDevi ListianiNo ratings yet
- Family Support and Quality of Life of Schizophrenia PatientsDocument8 pagesFamily Support and Quality of Life of Schizophrenia PatientsIJPHSNo ratings yet
- Psychiatric Morbidity and Subjective Burden Among Carers of Outpatients of A Psychogeriatric Clinic in Southwestern NigeriaDocument13 pagesPsychiatric Morbidity and Subjective Burden Among Carers of Outpatients of A Psychogeriatric Clinic in Southwestern NigeriaRobby RNo ratings yet
- Sleep Quality Among Primary Care Attendees in Kaduna, Northern Nigeria A Case-Control Study-Nuhu Et Al IJPMDocument11 pagesSleep Quality Among Primary Care Attendees in Kaduna, Northern Nigeria A Case-Control Study-Nuhu Et Al IJPMAdeyemi OlusolaNo ratings yet
- Lasebikan Ayinde 2013 Family Burden in Caregivers of Schizophrenia Patients Prevalence and Socio Demographic CorrelatesDocument7 pagesLasebikan Ayinde 2013 Family Burden in Caregivers of Schizophrenia Patients Prevalence and Socio Demographic CorrelatesAttiya ZainabNo ratings yet
- Somatization Disorder Among Adolescents in Southeast Nigeria: A Neglected IssueDocument7 pagesSomatization Disorder Among Adolescents in Southeast Nigeria: A Neglected Issueyeremias setyawanNo ratings yet
- Articulo 1Document5 pagesArticulo 1lucia acasieteNo ratings yet
- Pjms 29 1122Document6 pagesPjms 29 1122Edo GusdiansyahNo ratings yet
- Prevalence of Schizophrenia Among Patients Admitted Into Neuro-Psychiatric Hospital, Rumuigbo, Port Harcourt, Rivers State, NigeriaDocument9 pagesPrevalence of Schizophrenia Among Patients Admitted Into Neuro-Psychiatric Hospital, Rumuigbo, Port Harcourt, Rivers State, NigeriaSteven JonesNo ratings yet
- General Hospital Psychiatry: Psychiatry and Primary CareDocument5 pagesGeneral Hospital Psychiatry: Psychiatry and Primary CareAndra NicoleNo ratings yet
- Assessment of Factors Responsible For Relapses in Schizophrenic Patients at Kampala International University Teaching Hospital, Uganda.Document14 pagesAssessment of Factors Responsible For Relapses in Schizophrenic Patients at Kampala International University Teaching Hospital, Uganda.KIU PUBLICATION AND EXTENSIONNo ratings yet
- Kart Tune N 2010Document10 pagesKart Tune N 2010AndreiaNo ratings yet
- Pone 0250309Document16 pagesPone 0250309edo_gusdiansyahNo ratings yet
- My ProjectDocument34 pagesMy ProjectrahmatullahqueenmercyNo ratings yet
- Adolescent With CFSDocument6 pagesAdolescent With CFSiri_balNo ratings yet
- Psychosocial Impact of Sickle Cell Disorder - Perspectives From A Nigerian SettingDocument7 pagesPsychosocial Impact of Sickle Cell Disorder - Perspectives From A Nigerian SettingTomiwa AdeshinaNo ratings yet
- Caregivers Consequences of Care Among Patients With Eating DisordersDocument10 pagesCaregivers Consequences of Care Among Patients With Eating DisordersVictoria PazNo ratings yet
- Dokumen Tanpa JudulDocument9 pagesDokumen Tanpa Judulsalsabela fithriNo ratings yet
- BiblioDocument2 pagesBiblioFlorenze ArtNo ratings yet
- 5063-5069 4.18 Pinar Sercekus PDFDocument7 pages5063-5069 4.18 Pinar Sercekus PDFNurul ShahirahNo ratings yet
- Mypublicationin Int JResearchand Med SC Oct 2015Document9 pagesMypublicationin Int JResearchand Med SC Oct 2015Dr-Dalya ShakirNo ratings yet
- Demencies 2Document12 pagesDemencies 21821ainaNo ratings yet
- Delirium and Precipitants Among Elderly Medical Patients in A Nigerian HospitalDocument18 pagesDelirium and Precipitants Among Elderly Medical Patients in A Nigerian HospitalDiah Pradnya ParamitaNo ratings yet
- Family Burden in Patient With Schizophrenia and Depressive Disorder: A Comparative StudyDocument3 pagesFamily Burden in Patient With Schizophrenia and Depressive Disorder: A Comparative StudyBayu Firdaus SiradzNo ratings yet
- Review: Burden On Family Caregivers Caring For Patients With Schizophrenia and Its Related FactorsDocument13 pagesReview: Burden On Family Caregivers Caring For Patients With Schizophrenia and Its Related FactorsmesiNo ratings yet
- Factors Related To Family's Ability To Care For Schizophrenic PatientsDocument8 pagesFactors Related To Family's Ability To Care For Schizophrenic PatientsIJPHSNo ratings yet
- Subjective and Objective Caregiver Burden in Parkinson's DiseaseDocument7 pagesSubjective and Objective Caregiver Burden in Parkinson's Diseasearpit11111No ratings yet
- Attitudes Towards Mental Illness in Malawi: A Cross-Sectional SurveyDocument6 pagesAttitudes Towards Mental Illness in Malawi: A Cross-Sectional SurveyAdina OlteanuNo ratings yet
- Quality of Life of General and Psychiatric Ward Caregivers: A Comparative StudyDocument8 pagesQuality of Life of General and Psychiatric Ward Caregivers: A Comparative StudyIOSRjournalNo ratings yet
- Psychiatric Morbidities and Burden in Caregivers of Patients of Obsessive Compulsive DisorderDocument7 pagesPsychiatric Morbidities and Burden in Caregivers of Patients of Obsessive Compulsive DisorderIJAR JOURNALNo ratings yet
- Job Related Stress in Psychiatric NursesDocument8 pagesJob Related Stress in Psychiatric Nursesezinne obinna-umaNo ratings yet
- Classification and Clinical Features of Headache Disorders in Pakistan: A Retrospective Review of Clinical DataDocument8 pagesClassification and Clinical Features of Headache Disorders in Pakistan: A Retrospective Review of Clinical DatarikramNo ratings yet
- The Prevalence of Mental Disorders in Adults in Different Level General Medical Facilities in KenyaDocument8 pagesThe Prevalence of Mental Disorders in Adults in Different Level General Medical Facilities in KenyaxxxxomarxxxxNo ratings yet
- Research Article - Burnout Among Nurses in A Nigerian General HospitalDocument7 pagesResearch Article - Burnout Among Nurses in A Nigerian General HospitalAndrei AlexandruNo ratings yet
- Cohort CDocument14 pagesCohort CShodiq AbdillahNo ratings yet
- Quality of Life in Caregivers of Patients With Schizophrenia A Literature ReviewDocument6 pagesQuality of Life in Caregivers of Patients With Schizophrenia A Literature Reviewgw0q12dxNo ratings yet
- Belingheri Et AlDocument4 pagesBelingheri Et AlChiara ZanichelliNo ratings yet
- Research Concept Note For Addmission Into The Doctor of MedicineDocument2 pagesResearch Concept Note For Addmission Into The Doctor of Medicineumar farukNo ratings yet
- CC 12736Document8 pagesCC 12736Neneng HumairohNo ratings yet
- Quality of Life of Caregivers of Patients Diagnosed With SevereDocument10 pagesQuality of Life of Caregivers of Patients Diagnosed With SeverejlbermudezcNo ratings yet
- Journal 11Document5 pagesJournal 11Francis GecobeNo ratings yet
- Supporting and Empowering People With Epilepsy Contribution of The Epilepsy Specialist NursesDocument8 pagesSupporting and Empowering People With Epilepsy Contribution of The Epilepsy Specialist Nursescelia.longuetNo ratings yet
- BAGIAN ILMU PENYAKIT SARAF Journal ReadingDocument28 pagesBAGIAN ILMU PENYAKIT SARAF Journal ReadingKarelau KarniaNo ratings yet
- Characteristics of Nursing Care For Terminally Ill Patients in Hospice/Palliative Care UnitDocument9 pagesCharacteristics of Nursing Care For Terminally Ill Patients in Hospice/Palliative Care UnitFahmiNo ratings yet
- Epilepsy JournalDocument7 pagesEpilepsy JournalOcha24 TupamahuNo ratings yet
- Postpartum Psychiatric Disorders Atwo Year Retrospective Review at A Tertiary Health Institution in Damaturu North East Nigeria 1141Document6 pagesPostpartum Psychiatric Disorders Atwo Year Retrospective Review at A Tertiary Health Institution in Damaturu North East Nigeria 1141fanyNo ratings yet
- Depression Among Patients Attending Physiotherapy Clinics in Erbil CityDocument6 pagesDepression Among Patients Attending Physiotherapy Clinics in Erbil Citysarhang talebaniNo ratings yet
- Jurnal PD 4Document11 pagesJurnal PD 4Jay MNo ratings yet
- Relatives ' Quality of Life and Psychological Disturbance: A New Concern of SLE ManagementDocument7 pagesRelatives ' Quality of Life and Psychological Disturbance: A New Concern of SLE ManagementPrimadiati Nickyta SariNo ratings yet
- A2 - Loi, 2021Document8 pagesA2 - Loi, 2021bayu seno ajiNo ratings yet
- Health Related Quality of Life of Caregivers of Dementia PatientsDocument10 pagesHealth Related Quality of Life of Caregivers of Dementia PatientsΞένια ΤσιάκαλουNo ratings yet
- Public Health - Vol 2 - Issue 4 - Article 5Document44 pagesPublic Health - Vol 2 - Issue 4 - Article 5kaisamerno2003No ratings yet
- Determination of Qol On PLWHADocument5 pagesDetermination of Qol On PLWHASinta Maysila100% (1)
- Is Looking Older Than One's Actual Age A Sign of Poor HealthDocument6 pagesIs Looking Older Than One's Actual Age A Sign of Poor HealthIvan PeregorodievNo ratings yet
- Self-Management in Older Patients With Chronic Illness: ResearchpaperDocument11 pagesSelf-Management in Older Patients With Chronic Illness: ResearchpaperAlberto MeroNo ratings yet
- Psychological Distress TBDocument9 pagesPsychological Distress TBFirmanNo ratings yet
- Epilepsy & Behavior: Shanna M. Guilfoyle, Sally Monahan, Cindy Wesolowski, Avani C. ModiDocument6 pagesEpilepsy & Behavior: Shanna M. Guilfoyle, Sally Monahan, Cindy Wesolowski, Avani C. ModiJhonny BatongNo ratings yet
- Finding the Path in Alzheimer’s Disease: Early Diagnosis to Ongoing Collaborative CareFrom EverandFinding the Path in Alzheimer’s Disease: Early Diagnosis to Ongoing Collaborative CareNo ratings yet
- Asthma English2Document1 pageAsthma English2jadarcNo ratings yet
- Pubdoc 11 1697 150Document4 pagesPubdoc 11 1697 150jadarcNo ratings yet
- Pubdoc 11 670 150Document6 pagesPubdoc 11 670 150jadarcNo ratings yet
- Pubdoc 4 14280 150Document6 pagesPubdoc 4 14280 150jadarcNo ratings yet
- Pa Q LQ ValidationDocument7 pagesPa Q LQ ValidationjadarcNo ratings yet
- Air-Cooled Rotary Screw Chillers: Product ManualDocument84 pagesAir-Cooled Rotary Screw Chillers: Product ManualPragnesh BhalodiaNo ratings yet
- Sample Science Lesson PlanDocument5 pagesSample Science Lesson PlanLunafreya NyxNo ratings yet
- Problem and SolutionDocument22 pagesProblem and SolutiondaRainNo ratings yet
- Checklist: I. Q & A II. Ôn tập QuizzesDocument19 pagesChecklist: I. Q & A II. Ôn tập QuizzesLê Hoàng Minh ThưNo ratings yet
- Error Handling in CDocument3 pagesError Handling in CJaysinh KumpavatNo ratings yet
- A Study On Usage of Digital Banking in Rural AreasDocument7 pagesA Study On Usage of Digital Banking in Rural AreasKartik H ANo ratings yet
- Introduction To Industry 4.0 and Industrial IoT Week 3 Quiz SolutionsDocument5 pagesIntroduction To Industry 4.0 and Industrial IoT Week 3 Quiz SolutionssathyaNo ratings yet
- Review XXX ACS Guide 2014Document2 pagesReview XXX ACS Guide 2014Vinod ManjuNo ratings yet
- Group Assignment Golden RatioDocument4 pagesGroup Assignment Golden RatioRIFAH FIDZDIANI AIN BINTI RIFKIY FS21110415No ratings yet
- Engine Inspection Using Windrock Technology DiagnosticsDocument4 pagesEngine Inspection Using Windrock Technology DiagnosticsImranFazal100% (1)
- XL640 User ManualDocument213 pagesXL640 User ManualSIELAB C.A.No ratings yet
- 2.materials Technology Answered PDFDocument4 pages2.materials Technology Answered PDFOxbown9167% (6)
- Giancoli - Physics SolutionsDocument1 pageGiancoli - Physics Solutionspo4xx0% (1)
- Topographic Map of HagansportDocument1 pageTopographic Map of HagansportHistoricalMapsNo ratings yet
- Lesson Plan Week 1 The Eve of The Viking AgeDocument3 pagesLesson Plan Week 1 The Eve of The Viking AgeIsaac BoothroydNo ratings yet
- SR5 TOOL Adept Powers List + Description, CompiledDocument5 pagesSR5 TOOL Adept Powers List + Description, Compiledvwp09705No ratings yet
- Strategic Supply Chain ManagementDocument16 pagesStrategic Supply Chain ManagementKknow Ddrug100% (3)
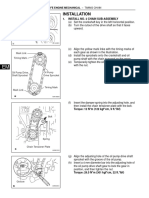
- Sincronizacion de Motor Toyota 2az-FeDocument12 pagesSincronizacion de Motor Toyota 2az-FeWilliams NavasNo ratings yet
- PHILIPS RC133V W62L62 1 xLED36S840 OC PDFDocument3 pagesPHILIPS RC133V W62L62 1 xLED36S840 OC PDFNavneet SinghNo ratings yet
- Pengaruh Skarifikasi Dan Hormon Giberelin (Ga) Terhadap Daya Kecambah Dan Pertumbuhan Bibit Palem Putri (Veitchia Merillii)Document8 pagesPengaruh Skarifikasi Dan Hormon Giberelin (Ga) Terhadap Daya Kecambah Dan Pertumbuhan Bibit Palem Putri (Veitchia Merillii)Adi IndraNo ratings yet
- WAP To Find The Sum of The Series S 1 + (3/2!) + (5/3!) + (7/4!) + ....... To NDocument8 pagesWAP To Find The Sum of The Series S 1 + (3/2!) + (5/3!) + (7/4!) + ....... To NSOUMYA MAHAPATRANo ratings yet
- Fitting Catalog 2013: Maret 2013 - 112Document39 pagesFitting Catalog 2013: Maret 2013 - 112SujokoTeeNo ratings yet
- MR Collins Maths Year 11 HomeworkDocument6 pagesMR Collins Maths Year 11 Homeworkafeueffmk100% (1)
- Additional Topics in Variance Analysis: True / False QuestionsDocument232 pagesAdditional Topics in Variance Analysis: True / False QuestionsElaine GimarinoNo ratings yet
- Predominance Area DiagramDocument5 pagesPredominance Area Diagramnaresh naikNo ratings yet
- Finite Element Heat Transfer EquationsDocument8 pagesFinite Element Heat Transfer EquationsRicox4444No ratings yet
- DLL-Q3-W6 - Mam LouDocument9 pagesDLL-Q3-W6 - Mam LouChello Ann Pelaez AsuncionNo ratings yet
- Focus ForecastingDocument4 pagesFocus ForecastingVedant MishraNo ratings yet
- StatisticsDocument2 pagesStatisticsAnish JohnNo ratings yet
- Session 2004: 21, Rue D'artois, F-75008 Paris © CigréDocument8 pagesSession 2004: 21, Rue D'artois, F-75008 Paris © CigréOscar GarciaNo ratings yet