You might also like
- The Nature of Substance - Rudolf Hauschka PDFDocument250 pagesThe Nature of Substance - Rudolf Hauschka PDFBruno Morin100% (5)
- Riordan Protocol For IVCDocument9 pagesRiordan Protocol For IVCNaturasfera Suplementos AlimenticiosNo ratings yet
- Design of A Tuned Intake Manifold - H. W. Engelman (ASME Paper 73-WA/DGP-2)Document9 pagesDesign of A Tuned Intake Manifold - H. W. Engelman (ASME Paper 73-WA/DGP-2)david_luzNo ratings yet
- Collaboration Processes: Looking Inside the Black BoxDocument13 pagesCollaboration Processes: Looking Inside the Black Boxเข้าใจว่า น่าจะชื่อตุ้นNo ratings yet
- Construction Site PremisesDocument78 pagesConstruction Site PremisesDrew B Mrtnz67% (6)
- Vitamin C: Should We Supplement?: ReviewDocument8 pagesVitamin C: Should We Supplement?: ReviewOlivia CristieNo ratings yet
- Hydrocortisone, Vitamin C, and Thiamine For The Treatment of Severe Sepsis and Septic ShockDocument10 pagesHydrocortisone, Vitamin C, and Thiamine For The Treatment of Severe Sepsis and Septic Shockmmmaw mmNo ratings yet
- Marik 2016Document10 pagesMarik 2016PedroNo ratings yet
- Vitamina C, Tiamina, Corticoides and Shock SepticoDocument10 pagesVitamina C, Tiamina, Corticoides and Shock SepticoNorvingNo ratings yet
- Vitamin C, Hydrocortisone and Thiamine in Patients With Septic Shock (VITAMINS) Trial: Study Protocol and Statistical Analysis PlanDocument7 pagesVitamin C, Hydrocortisone and Thiamine in Patients With Septic Shock (VITAMINS) Trial: Study Protocol and Statistical Analysis Planjesus peñaNo ratings yet
- Vitamin C and Viral InfectionDocument3 pagesVitamin C and Viral InfectionFARCASANU MARIA-ANDREEANo ratings yet
- Vitamin C My Literature ReviewDocument7 pagesVitamin C My Literature ReviewAnestis FilopoulosNo ratings yet
- IntravenousVitaminCTherapyDocument3 pagesIntravenousVitaminCTherapyfrancoNo ratings yet
- Vitaminas en SepsisDocument9 pagesVitaminas en SepsisAndrés Felipe PérezNo ratings yet
- Treating SepsisDocument4 pagesTreating SepsisEdwin ClNo ratings yet
- Micronutrient Deficiency in Critical Illness: An Invisible Foe?Document4 pagesMicronutrient Deficiency in Critical Illness: An Invisible Foe?Lee Foo WengNo ratings yet
- B-Group Vitamin Supplementation Mitigates Oxidative Damage After Acute Ischaemic StrokeDocument8 pagesB-Group Vitamin Supplementation Mitigates Oxidative Damage After Acute Ischaemic StrokeLyslie Maron RibeiroNo ratings yet
- Vitamin C May Reduce Mortality in COVID-19 PatientsDocument25 pagesVitamin C May Reduce Mortality in COVID-19 PatientsLizNo ratings yet
- News & Views: Restrictive Fluid Therapy and High-Dose Vitamin C in SepsisDocument2 pagesNews & Views: Restrictive Fluid Therapy and High-Dose Vitamin C in SepsisLAURA ALEJANDRA GONZALEZ MONTOYANo ratings yet
- Hipocalcemia en La Enf CriticaDocument9 pagesHipocalcemia en La Enf CriticaDarwin CamposNo ratings yet
- Vitamin C and Its Therapeutic Potential in the ManDocument7 pagesVitamin C and Its Therapeutic Potential in the ManJose VasquezNo ratings yet
- Management of Severe Sepsis: Learning ObjectivesDocument5 pagesManagement of Severe Sepsis: Learning ObjectivesVictoriano Valiente100% (1)
- Udy 2010Document3 pagesUdy 2010aNo ratings yet
- Mega Doses of Vit CDocument1 pageMega Doses of Vit CSALVADORNo ratings yet
- 1 s2.0 S1549963419302011 MainDocument15 pages1 s2.0 S1549963419302011 MainYeroNo ratings yet
- Vitamins & Minerals: Metadichol Induced High Levels of Vitamin C: Case StudiesDocument5 pagesVitamins & Minerals: Metadichol Induced High Levels of Vitamin C: Case StudiesSilambarasu KaruppiahNo ratings yet
- Journal Medicine: The New EnglandDocument11 pagesJournal Medicine: The New EnglandSali ÁdámNo ratings yet
- Adjuvant Steroid Therapy in Community-Acquired Pneumonia: What 'S New in Infectious DiseasesDocument3 pagesAdjuvant Steroid Therapy in Community-Acquired Pneumonia: What 'S New in Infectious DiseasesDianNo ratings yet
- Suliman 2018Document12 pagesSuliman 2018juheb ansariNo ratings yet
- Azithromycin For The Prevention of COPD ExacerbationsDocument6 pagesAzithromycin For The Prevention of COPD ExacerbationsI Made AryanaNo ratings yet
- Vitamina D 2010Document7 pagesVitamina D 2010amb251No ratings yet
- Vitamin D and Ocular InflammationDocument5 pagesVitamin D and Ocular InflammationRIYA PARVEENNo ratings yet
- Vit C Infusion in SepsisDocument12 pagesVit C Infusion in Sepsisعدنان عبد الملكNo ratings yet
- DIC Pregnancy 2009 PDFDocument2 pagesDIC Pregnancy 2009 PDFGebbyNo ratings yet
- Vitamin E in The Prevention of Cardiovascular Disease: The Importance of Proper Patient SelectionDocument8 pagesVitamin E in The Prevention of Cardiovascular Disease: The Importance of Proper Patient SelectionaniNo ratings yet
- Utility of Procalcitonin in Clinical PracticeDocument8 pagesUtility of Procalcitonin in Clinical PracticeEdward ElBuenoNo ratings yet
- Hypertension JournalDocument5 pagesHypertension JournalYola SurbaktiNo ratings yet
- SepsisDocument7 pagesSepsisrifkizidnyNo ratings yet
- Jan 23Document80 pagesJan 23kalpana chamlingNo ratings yet
- Corona VirusDocument8 pagesCorona VirusIndraNo ratings yet
- Hormonal Therapies in Septic Shock: Review ArticleDocument8 pagesHormonal Therapies in Septic Shock: Review ArticleJhon3xNo ratings yet
- Recommendation-Specific Supportive TextDocument22 pagesRecommendation-Specific Supportive Textodaliz.berrocalNo ratings yet
- Vit CDocument10 pagesVit C3/2 no.34 สรัญญากร สีหาราชNo ratings yet
- Infectious DiseasesDocument9 pagesInfectious DiseasesMaharani Sari NastitiNo ratings yet
- Ingles 2020Document8 pagesIngles 2020Tika HapsariNo ratings yet
- Intensive Care Unit Management of The Trauma PatientDocument8 pagesIntensive Care Unit Management of The Trauma Patientantonio dengNo ratings yet
- Combined QDocument46 pagesCombined QRoh JitenNo ratings yet
- Vitamin C For SepsisDocument3 pagesVitamin C For SepsissignaturebeatNo ratings yet
- 270 FullDocument4 pages270 Fullpalembang2015No ratings yet
- 20 - Doddakula2010Document6 pages20 - Doddakula2010TandeanTommyNovenantoNo ratings yet
- Safety and Efficacy of CorticosteroidsDocument9 pagesSafety and Efficacy of CorticosteroidsMatt CoghlanNo ratings yet
- A Review of Micronutrients in Sepsis The Role of Thiamine L Carnitine Vitamin C Selenium and Vitamin DDocument10 pagesA Review of Micronutrients in Sepsis The Role of Thiamine L Carnitine Vitamin C Selenium and Vitamin Dmiftah furqonNo ratings yet
- Mekanisme Scurvy (Prinsip Kolagen) Karena Defisiensi Vitamin CDocument8 pagesMekanisme Scurvy (Prinsip Kolagen) Karena Defisiensi Vitamin CFeby MutiaNo ratings yet
- Article 01Document2 pagesArticle 01Robin AthotaNo ratings yet
- Research ArticleDocument5 pagesResearch ArticleiwanNo ratings yet
- Perspectives in Clinical Hepatology Current and Novel Immunosuppressive Therapy For Autoimmune HepatitisDocument7 pagesPerspectives in Clinical Hepatology Current and Novel Immunosuppressive Therapy For Autoimmune HepatitisPathrecia Natalia SiagianNo ratings yet
- Manejo de La Sepsis 2Document5 pagesManejo de La Sepsis 2Rachmi Pratiwi Febrita PartiNo ratings yet
- Vitamin C Pharmacokinetics: Implications For Oral and Intravenous UseDocument6 pagesVitamin C Pharmacokinetics: Implications For Oral and Intravenous UseΒόρειο ΣέλαςNo ratings yet
- Lodoco PilotDocument8 pagesLodoco PilotAndreas Erick HaurissaNo ratings yet
- Sharifi2019 PDFDocument7 pagesSharifi2019 PDFmoussaouiNo ratings yet
- Hypovolemic Shock ResuscitationDocument21 pagesHypovolemic Shock ResuscitationM Lutfi FananiNo ratings yet
- Vitamin D Penelitian CHFDocument6 pagesVitamin D Penelitian CHFEga NurNo ratings yet
- Management of Fungal Infections in MCS and Cardiothoracic Organ Transplant Recipients: ISHLT Monograph Series (Volume 12)From EverandManagement of Fungal Infections in MCS and Cardiothoracic Organ Transplant Recipients: ISHLT Monograph Series (Volume 12)No ratings yet
- Let Us Discover: Hairdressing-Grade 11Document5 pagesLet Us Discover: Hairdressing-Grade 11cherry d.bandolaNo ratings yet
- Course Progression Map For 2021 Commencing Students: E3001 Bachelor of Engineering (Honours) Common First YearDocument21 pagesCourse Progression Map For 2021 Commencing Students: E3001 Bachelor of Engineering (Honours) Common First YearNguyễn An KhoaNo ratings yet
- Genética, Modificaciones y MutacionesDocument12 pagesGenética, Modificaciones y MutacionespokemaniacoplancheNo ratings yet
- ĐỀ SỐ 2Document98 pagesĐỀ SỐ 2van hoa nguyenNo ratings yet
- Explore the beaches and parks of Labuan IslandDocument2 pagesExplore the beaches and parks of Labuan IslandDudeNo ratings yet
- Category D Fluid ServiceDocument2 pagesCategory D Fluid Serviceaslam.ambNo ratings yet
- PSUTIL Documentation for Monitoring System ResourcesDocument77 pagesPSUTIL Documentation for Monitoring System ResourcesImam RiadiNo ratings yet
- G5 C11 TestDocument6 pagesG5 C11 TestvictoriaNo ratings yet
- 3M CatalogueDocument32 pages3M Cataloguefandi.azs37No ratings yet
- Plasma ChemistryDocument6 pagesPlasma ChemistryArief RomadhonNo ratings yet
- Effect of Pregnancy Induced Hypertension on Mothers and Babies Hematological ProfilesDocument3 pagesEffect of Pregnancy Induced Hypertension on Mothers and Babies Hematological ProfilesAbdifatah AhmedNo ratings yet
- Reles, Fuentes, Etc. Catalogo - ABBDocument452 pagesReles, Fuentes, Etc. Catalogo - ABBmpica100% (1)
- Stereochemistry MSCDocument29 pagesStereochemistry MSCBapu Thorat50% (2)
- Fit For WashingDocument85 pagesFit For WashingIyaka YoeNo ratings yet
- Postmodern EthicsDocument1 pagePostmodern Ethicsgeorge elerickNo ratings yet
- Radiological Investigations: UltrasonographyDocument42 pagesRadiological Investigations: UltrasonographyDeeptanu GhoshNo ratings yet
- Partial Discharge - Open ElectricalDocument2 pagesPartial Discharge - Open ElectricalBHALAJI BIRLANo ratings yet
- Electronic V-MAC IV Vehicle Mgmt. and Control With Co-Pilot Display Operator ManualDocument133 pagesElectronic V-MAC IV Vehicle Mgmt. and Control With Co-Pilot Display Operator Manualsanach0412No ratings yet
- 07 IRIS NV PCB OtherDocument15 pages07 IRIS NV PCB OtherArnaldo cordovaNo ratings yet
- EniSpA - The Corporate Strategy of An International Energy Major PDFDocument24 pagesEniSpA - The Corporate Strategy of An International Energy Major PDFAnonymous 9ZMbuR75% (4)
- Erotic MassageDocument113 pagesErotic MassageMahmoud El Mohamdy75% (4)
- NPT Pipe Thread Sizes and TapersDocument1 pageNPT Pipe Thread Sizes and TapersRajesh J BharadwajNo ratings yet
- Model Question Paper and Solution 2022Document14 pagesModel Question Paper and Solution 2022R Y AnushNo ratings yet
- Diagrama 4 AMBIENT AIR TEMPER..Document1 pageDiagrama 4 AMBIENT AIR TEMPER..Gustavo PérezNo ratings yet
- A History of The Jewish People in The Time of Jesus Christ (1891) Index Schürer, Emil, 1844-1910Document132 pagesA History of The Jewish People in The Time of Jesus Christ (1891) Index Schürer, Emil, 1844-1910David Bailey100% (2)
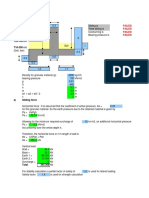
- Sliding, Overturning, Bearing Pressure and Bending Reinforcement Calculations for Retaining WallDocument4 pagesSliding, Overturning, Bearing Pressure and Bending Reinforcement Calculations for Retaining WallAbdul Aziz Julkarnain ZulkifliNo ratings yet