You might also like
- COVID-19 Vaccination Perception and Attitude Among Healthcare Workers in EgyptDocument9 pagesCOVID-19 Vaccination Perception and Attitude Among Healthcare Workers in Egyptnene100% (1)
- 02 Behrmann 2022Document17 pages02 Behrmann 2022Ximena PerdomoNo ratings yet
- JKNKLKLDocument10 pagesJKNKLKLCyntia AndrinaNo ratings yet
- Factors Associated With Mental Health Disorders Among University Students in France Confined During The COVID-19 PandemicDocument13 pagesFactors Associated With Mental Health Disorders Among University Students in France Confined During The COVID-19 PandemicManoj MaggotNo ratings yet
- Psychological Health During The Coronavirus Disease 2019 Pandemic OutbreakDocument5 pagesPsychological Health During The Coronavirus Disease 2019 Pandemic OutbreakStefenie Katrin SibosNo ratings yet
- Correlation of Anxiety Level With Clinical Description in Covid-19 Patients Using Coronavirus Anxiety Scale at H. Adam Malik RSUPDocument6 pagesCorrelation of Anxiety Level With Clinical Description in Covid-19 Patients Using Coronavirus Anxiety Scale at H. Adam Malik RSUPInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Covid 19 Psychological Effects and Associated Factors in Mexican NursesDocument7 pagesCovid 19 Psychological Effects and Associated Factors in Mexican NursesDelgado Valdez AndrésNo ratings yet
- Knowledge, Attitudes, and Practices Regarding COVID-19 Prevention Among Vietnamese Healthcare Workers in 2020Document7 pagesKnowledge, Attitudes, and Practices Regarding COVID-19 Prevention Among Vietnamese Healthcare Workers in 2020Manasi PandaNo ratings yet
- Pandemic Worry and Preventive Health Behaviors During The COVID-19 OutbreakDocument8 pagesPandemic Worry and Preventive Health Behaviors During The COVID-19 OutbreakFabiola NogaNo ratings yet
- COVID-19 Pandemic Worry and Vaccination Intention: The Mediating Role of The Health Belief Model ComponentsDocument8 pagesCOVID-19 Pandemic Worry and Vaccination Intention: The Mediating Role of The Health Belief Model ComponentsClauNo ratings yet
- Fpsyt 12 608730Document21 pagesFpsyt 12 608730dinarNo ratings yet
- 12 LilyDocument17 pages12 LilyDave PeriaNo ratings yet
- Effects of COVID-19 Stress Proximity and Adverse CDocument13 pagesEffects of COVID-19 Stress Proximity and Adverse CKrishnapriya T SNo ratings yet
- The Outbreak of COVID-19 Coronavirus and Its Impact On Global Mental HealthDocument4 pagesThe Outbreak of COVID-19 Coronavirus and Its Impact On Global Mental HealthDilla AmeliaNo ratings yet
- Editorial: Impact of The Coronavirus Pandemic (COVID-19) On Mood Disorders and SuicideDocument3 pagesEditorial: Impact of The Coronavirus Pandemic (COVID-19) On Mood Disorders and SuicideAishwaryaNo ratings yet
- Misc 1Document12 pagesMisc 1Rupesh ShresthaNo ratings yet
- 1 s2.0 S2405844022007101 MainDocument7 pages1 s2.0 S2405844022007101 MainHung TranNo ratings yet
- COVID-19 and Mental Health A Systematic Review of International Medical Student SurveysDocument13 pagesCOVID-19 and Mental Health A Systematic Review of International Medical Student SurveysEsteban MatusNo ratings yet
- 1 s2.0 S0196655320306386 MainDocument7 pages1 s2.0 S0196655320306386 MainOktomi WijayaNo ratings yet
- Akk Jurnal Internasional 1Document7 pagesAkk Jurnal Internasional 1Onnii SltrNo ratings yet
- Our Elderly's Mental Health in Times of COVID-19Document12 pagesOur Elderly's Mental Health in Times of COVID-19Seba FuzzNo ratings yet
- Knowledge, Attitude, and Practices Towards The COVID-19 Pandemic Among Undergraduate StudentsDocument13 pagesKnowledge, Attitude, and Practices Towards The COVID-19 Pandemic Among Undergraduate StudentsSiti NurawaliahNo ratings yet
- CureusDocument10 pagesCureuspopasorinemilianNo ratings yet
- The Psychological Impact of COVID-19 On Front Line NursesDocument17 pagesThe Psychological Impact of COVID-19 On Front Line NursesPetar PanNo ratings yet
- Article 2Document5 pagesArticle 2Ecnal JeremiahNo ratings yet
- F-4 (BD 1) Mental Health-HCPsDocument18 pagesF-4 (BD 1) Mental Health-HCPstowhidul alamNo ratings yet
- Loneliness During The COVID-19 Pandemic Among Older Adults With Chronic ConditionsDocument10 pagesLoneliness During The COVID-19 Pandemic Among Older Adults With Chronic ConditionsCHETHANNo ratings yet
- Psychological Impact of The Quarantine During The COVID-19 Pandemic On The General European Adult Population: A Systematic Review of The EvidenceDocument19 pagesPsychological Impact of The Quarantine During The COVID-19 Pandemic On The General European Adult Population: A Systematic Review of The EvidenceRizky Adib KurniaqilNo ratings yet
- Determining Depression and Related Factors in A Society Affected by COVID-19 PandemicDocument10 pagesDetermining Depression and Related Factors in A Society Affected by COVID-19 Pandemicverdeoros uaemexNo ratings yet
- Stigmatisation Associated With COVID-19 in The General Colombian PopulationDocument9 pagesStigmatisation Associated With COVID-19 in The General Colombian PopulationAzzalfaAftaniNo ratings yet
- Stress Among The Nurses and Their Family InvolvedDocument7 pagesStress Among The Nurses and Their Family InvolvedAditya SutarNo ratings yet
- Mental Health Implications of COVID-19 Pandemic and Its Response in IndiaDocument14 pagesMental Health Implications of COVID-19 Pandemic and Its Response in IndiaRomy HidayatNo ratings yet
- Journal Pone 0249716Document16 pagesJournal Pone 0249716Abhinaya A Saravanan UdayarNo ratings yet
- Kirana 2021 IOP Conf. Ser. Earth Environ. Sci. 755 012080Document5 pagesKirana 2021 IOP Conf. Ser. Earth Environ. Sci. 755 012080febryanti 29No ratings yet
- Ijerph 18 09880 v2Document19 pagesIjerph 18 09880 v2Anne Caitlene PamintuanNo ratings yet
- JURNALDocument20 pagesJURNALDewi SunnnNo ratings yet
- Research Paper:: Health Responses During The COVID-19 Pandemic: An International Strategy and Experience AnalysisDocument14 pagesResearch Paper:: Health Responses During The COVID-19 Pandemic: An International Strategy and Experience AnalysisRobert BretonNo ratings yet
- Student Mental Health in The Midst of The COVID-19 Pandemic: A Call For Further Research and Immediate SolutionsDocument2 pagesStudent Mental Health in The Midst of The COVID-19 Pandemic: A Call For Further Research and Immediate SolutionsRONALD ANDRe BULEJE HINOSTROZANo ratings yet
- Psychological Impacts and Online Interventions of Social Isolation Amongst Older Adults During COVID-19 Pandemic: A Scoping ReviewDocument39 pagesPsychological Impacts and Online Interventions of Social Isolation Amongst Older Adults During COVID-19 Pandemic: A Scoping ReviewEmmanuel Ayodele DavidNo ratings yet
- Jurnal (Psikiatric TTG Covid)Document10 pagesJurnal (Psikiatric TTG Covid)Forensik UMINo ratings yet
- Impact of COVID-19 On University Students An Analysis of ItsDocument15 pagesImpact of COVID-19 On University Students An Analysis of ItsNadhif IlyasaNo ratings yet
- Ijerph 18 00861Document10 pagesIjerph 18 00861shameless.No ratings yet
- Family Resilience During COVID-19 Pandemic: A Literature ReviewDocument7 pagesFamily Resilience During COVID-19 Pandemic: A Literature ReviewCorina PaicaNo ratings yet
- The Psychological Impact of The COVID-19 Pandemic On Adults and Children in The United Arab Emirates: A Nationwide Cross-Sectional StudyDocument18 pagesThe Psychological Impact of The COVID-19 Pandemic On Adults and Children in The United Arab Emirates: A Nationwide Cross-Sectional StudyRafa MSánchezNo ratings yet
- Physio-Social Impact of Covid19Document10 pagesPhysio-Social Impact of Covid19Low Wai LeongNo ratings yet
- Risk Factors For Covid 19 Related Stress Among College Going StudentsDocument7 pagesRisk Factors For Covid 19 Related Stress Among College Going Studentsvan deNo ratings yet
- Mental Health Tele MedicineDocument7 pagesMental Health Tele Medicineसारथी समयNo ratings yet
- The Global Prevalence of Anxiety DepressDocument19 pagesThe Global Prevalence of Anxiety DepresswalkensiocsNo ratings yet
- Influence of COVID-19 Social Distancing Preventive Measure On The Psychological Well-Being of Kenya Certificate of Secondary Education (KCSE) 2021 Candidates in Mombasa County, KenyaDocument10 pagesInfluence of COVID-19 Social Distancing Preventive Measure On The Psychological Well-Being of Kenya Certificate of Secondary Education (KCSE) 2021 Candidates in Mombasa County, KenyaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Paper 1Document14 pagesPaper 1warface98No ratings yet
- Referensi 47Document7 pagesReferensi 47SaebaNo ratings yet
- Epidemiology of Mental Health Problems in COVID-19 - A ReviewDocument16 pagesEpidemiology of Mental Health Problems in COVID-19 - A ReviewIrinNo ratings yet
- Levels and Predictors of Anxiety, Depression and Health Anxiety During COVID-19 Pandemic in Turkish Society: The Importance of GenderDocument8 pagesLevels and Predictors of Anxiety, Depression and Health Anxiety During COVID-19 Pandemic in Turkish Society: The Importance of GendernadiaNo ratings yet
- Mental Health Problems and Correlates Among 746 217 College Students During The Coronavirus Disease 2019 Outbreak in ChinaDocument10 pagesMental Health Problems and Correlates Among 746 217 College Students During The Coronavirus Disease 2019 Outbreak in ChinaReyes Ivan García CuevasNo ratings yet
- SARS - MERS - SARS - CoV - 2 Outbreaks and Burnout Syndrome Among Healthcare Workers. An Umbrella Systematic ReviewDocument14 pagesSARS - MERS - SARS - CoV - 2 Outbreaks and Burnout Syndrome Among Healthcare Workers. An Umbrella Systematic ReviewNatalia BettancourtNo ratings yet
- Fear, Stress, Resilience and Coping Strategies During COVID-19 in Spanish University StudentsDocument19 pagesFear, Stress, Resilience and Coping Strategies During COVID-19 in Spanish University StudentsSassy BlaireNo ratings yet
- Covid 19Document7 pagesCovid 19Saurav KumarNo ratings yet
- Jurnal JiwaDocument9 pagesJurnal JiwasanidysaNo ratings yet
- 2 COVID-19 Survivors' Psychological Health An Exploratory StudyDocument20 pages2 COVID-19 Survivors' Psychological Health An Exploratory StudyApplied Psychology Review (APR)No ratings yet
- Certificate For COVID-19 Vaccination: Beneficiary DetailsDocument1 pageCertificate For COVID-19 Vaccination: Beneficiary DetailsHari AmaNo ratings yet
- Visitor Health Declaration FormDocument1 pageVisitor Health Declaration FormHung Kwan1 KeungNo ratings yet
- Covid-19 Impact: To The Philippines and The Rest of The WorldDocument1 pageCovid-19 Impact: To The Philippines and The Rest of The WorldSelene BrondialNo ratings yet
- Accomplishment Report DRRM 2022Document2 pagesAccomplishment Report DRRM 2022Nico GarciaNo ratings yet
- TAFFIX SCIENCE PAPER Feb 2021Document10 pagesTAFFIX SCIENCE PAPER Feb 2021Sanja IlićNo ratings yet
- Grade 5 - ISSUES-AND-CONCERNS-FOR-HEALTH-SCHOOL-READINESS-OTHER-CONCERNSDocument2 pagesGrade 5 - ISSUES-AND-CONCERNS-FOR-HEALTH-SCHOOL-READINESS-OTHER-CONCERNSDanny LineNo ratings yet
- December 5,2021 Until Recommended by Medical Team: Post Duty Quarantine: Specimen DriverDocument7 pagesDecember 5,2021 Until Recommended by Medical Team: Post Duty Quarantine: Specimen DriverMichael MedrosoNo ratings yet
- Maklumat Vaksinasi: Vaccination DetailsDocument2 pagesMaklumat Vaksinasi: Vaccination DetailsShasha BakarNo ratings yet
- (SOAL) Literasi Bahasa Inggris SAINSINDocument7 pages(SOAL) Literasi Bahasa Inggris SAINSIN07Neaura raraNo ratings yet
- The Debate Final ScriptDocument4 pagesThe Debate Final ScriptKathrina HuertoNo ratings yet
- Cesc Day3Document11 pagesCesc Day3Emily DayaNo ratings yet
- Mgt368-Individual Assignment PDFDocument8 pagesMgt368-Individual Assignment PDFAfrida Hoque Purba 2022129630No ratings yet
- Soal B.ing WJB AAT Kls XIDocument30 pagesSoal B.ing WJB AAT Kls XIVincentia Intan Andini AyuningatiNo ratings yet
- 213 1940 1 PBDocument5 pages213 1940 1 PBDuma PanjaitanNo ratings yet
- The Impact of Covid-19 On The Household Economy and Consumption Preferences: An International SurveyDocument26 pagesThe Impact of Covid-19 On The Household Economy and Consumption Preferences: An International SurveysompasongNo ratings yet
- ĐỀ CHÍNH THỨC VÀO 10Document8 pagesĐỀ CHÍNH THỨC VÀO 10Azura LouisaNo ratings yet
- Narrative ReportDocument5 pagesNarrative ReportRaffyNo ratings yet
- WHO PHL COVID 19 Situation Report 114Document9 pagesWHO PHL COVID 19 Situation Report 114jessica sugaboNo ratings yet
- MutationDocument6 pagesMutationALEJANDRO COUTIÑO VALDOVINOSNo ratings yet
- 1 - The Covid-19 Vaccine Is GENE THERAPY - David Martin BotW - Transcript - 01!11!2021Document7 pages1 - The Covid-19 Vaccine Is GENE THERAPY - David Martin BotW - Transcript - 01!11!2021bigbill138No ratings yet
- PSC Minutes Jan 2023Document2 pagesPSC Minutes Jan 2023KAUSPH NURSING SERVICENo ratings yet
- Covid 19 Vaccine Breakthrough British English TeacherDocument7 pagesCovid 19 Vaccine Breakthrough British English TeacherИллаNo ratings yet
- Evolutionary Artificial Intelligence Based Peptide Discoveries For EffectiveDocument13 pagesEvolutionary Artificial Intelligence Based Peptide Discoveries For EffectiveLucas PalmeiraNo ratings yet
- Verify Gov SGDocument4 pagesVerify Gov SGTha OoNo ratings yet
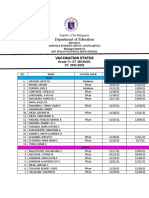
- Department of Education: Vaccination StatusDocument2 pagesDepartment of Education: Vaccination StatusKristelle BigawNo ratings yet
- A Mathematical Model For The Spatiotemporal Epidemic Spreading of COVID19Document13 pagesA Mathematical Model For The Spatiotemporal Epidemic Spreading of COVID19Barbara BusanelloNo ratings yet
- Trial Registered Prospectively: Modification(s)Document6 pagesTrial Registered Prospectively: Modification(s)dincina70No ratings yet
- Soal TO TOEFLDocument11 pagesSoal TO TOEFLIis AnnaNo ratings yet
- Tirumala Tirupati Devasthanams (Official Booking Portal)Document2 pagesTirumala Tirupati Devasthanams (Official Booking Portal)Selvakumar SNo ratings yet
- Points To Note For Persons Tested Preliminarily Positive / Positive Pending Admission To Hospitals or Isolation Facilities LeafletDocument2 pagesPoints To Note For Persons Tested Preliminarily Positive / Positive Pending Admission To Hospitals or Isolation Facilities LeafletHKFPNo ratings yet