You might also like
- Harvard Business Review on Fixing Healthcare from Inside & OutFrom EverandHarvard Business Review on Fixing Healthcare from Inside & OutNo ratings yet
- Literature ReviewDocument19 pagesLiterature Reviewapi-34163711675% (4)
- Access, Cost, and Quality For APNsDocument6 pagesAccess, Cost, and Quality For APNsMellyne SallyNo ratings yet
- Taking Action To Close The Nursing-Finance Gap: Learning From SuccessDocument3 pagesTaking Action To Close The Nursing-Finance Gap: Learning From SuccessRye Anch100% (1)
- Healthcare Cost ContainmentDocument26 pagesHealthcare Cost ContainmentSri ANo ratings yet
- A Medical Director's Perspective: Interview With Two Medical DirectorsDocument3 pagesA Medical Director's Perspective: Interview With Two Medical Directorsacma2010No ratings yet
- Porter y Kapplan (2011)Document18 pagesPorter y Kapplan (2011)ANA MARIA RIOSNo ratings yet
- Literature Review 1Document25 pagesLiterature Review 1kumar shubhamNo ratings yet
- Kaplan - Porter - 2011 9 - How To Solve The Cost Crisis in Health Care - HBRDocument15 pagesKaplan - Porter - 2011 9 - How To Solve The Cost Crisis in Health Care - HBRbayu prabuNo ratings yet
- Budgeting and Managing ResourcesDocument9 pagesBudgeting and Managing ResourcesEllen Grace Cañarejo BaroyNo ratings yet
- Ctu Medication ManagementnovoiceDocument12 pagesCtu Medication Managementnovoiceapi-240028260No ratings yet
- Medical Billing Best Practices Ebook GreenwayDocument26 pagesMedical Billing Best Practices Ebook GreenwayKiran KambleNo ratings yet
- E-Portfolio Term Project - Provider Relations Manager Bret Gashler - FinalDocument9 pagesE-Portfolio Term Project - Provider Relations Manager Bret Gashler - Finalapi-325641098No ratings yet
- 1.the Promise of Lean in Healthcare Article PDFDocument9 pages1.the Promise of Lean in Healthcare Article PDFP S Lakshmi KanthanNo ratings yet
- 8 Traits of A Successful Medical Practice: MGMA 2018Document2 pages8 Traits of A Successful Medical Practice: MGMA 2018Gerry FonziNo ratings yet
- 4 Big Challenges Facing HR Professionals in The Healthcare IndustryDocument4 pages4 Big Challenges Facing HR Professionals in The Healthcare IndustryMuhammad Junaid Bin YousufNo ratings yet
- Trends Report Cosmetic Surgery 2022Document17 pagesTrends Report Cosmetic Surgery 2022هشام العراقيNo ratings yet
- An RX For Health Care Woes - CPAs and Firms Can Manage Health Care Costs NowDocument4 pagesAn RX For Health Care Woes - CPAs and Firms Can Manage Health Care Costs NowJill Edmonds, Communications DirectorNo ratings yet
- Davidson, J. (2015) - What's All The Buzz About Change ManagementDocument3 pagesDavidson, J. (2015) - What's All The Buzz About Change ManagementBob SmithNo ratings yet
- Group Captives: Are They Right For You?: by - Jim HoittDocument6 pagesGroup Captives: Are They Right For You?: by - Jim HoittVicente TorresNo ratings yet
- Healthcare Process Management GuideDocument5 pagesHealthcare Process Management Guideapi-388173202No ratings yet
- Nurse Staffing RatioDocument6 pagesNurse Staffing Ratiomainaisaiah069No ratings yet
- Group Practice Journal: Key Success Factors For Private Practice Hospital Medicine GroupsDocument4 pagesGroup Practice Journal: Key Success Factors For Private Practice Hospital Medicine GroupsMhini Baba JayNo ratings yet
- Engaging Employees at VA Medical CentersDocument6 pagesEngaging Employees at VA Medical CentersFedSmith Inc.100% (1)
- All-Wharton-2009-Rethinking Lean Beyond The Shop Floor PDFDocument18 pagesAll-Wharton-2009-Rethinking Lean Beyond The Shop Floor PDFVishnupriya SharmaNo ratings yet
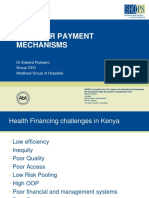
- Provider Payment MechanismsDocument20 pagesProvider Payment MechanismsCristhian LarrahondoNo ratings yet
- CH SlideDeck Presented by Jay DuvalDocument21 pagesCH SlideDeck Presented by Jay Duvaljordyn1990No ratings yet
- Promoting Planned Parenthood MGTDocument8 pagesPromoting Planned Parenthood MGTapi-508023811No ratings yet
- Compensation & Motivation: Thomas E. Catanzaro, DVM, MHA, FACHE Diplomate, American College of Healthcare ExecutivesDocument4 pagesCompensation & Motivation: Thomas E. Catanzaro, DVM, MHA, FACHE Diplomate, American College of Healthcare ExecutivesPaulos MpaltzidisNo ratings yet
- Qi ProjectDocument14 pagesQi Projectapi-641501601No ratings yet
- Evolving Health Care ModelDocument47 pagesEvolving Health Care Modelibson045001256No ratings yet
- One Medical - Ebook - Definitive Guide To Employee HealthcareDocument20 pagesOne Medical - Ebook - Definitive Guide To Employee HealthcareFaizal Rahman HakimNo ratings yet
- White Paper - IntegrationDocument3 pagesWhite Paper - Integrationapi-394732998No ratings yet
- Complete Issue Analysis PaperDocument10 pagesComplete Issue Analysis Paperapi-407581532No ratings yet
- The Pocket Guide to Practice Value Creation: Growing Your Medical Practice without Burning OutFrom EverandThe Pocket Guide to Practice Value Creation: Growing Your Medical Practice without Burning OutNo ratings yet
- April 2011 NewsletterDocument4 pagesApril 2011 Newsletterhhughes3950No ratings yet
- Frontline of Healthcare - It's Time To Elevate The Patient Experience in Healthcare - Bain & CompanyDocument5 pagesFrontline of Healthcare - It's Time To Elevate The Patient Experience in Healthcare - Bain & Companyb00810902No ratings yet
- Gateway HospitalDocument1 pageGateway HospitalMehreen ShamimNo ratings yet
- Thesis On Nurse RetentionDocument6 pagesThesis On Nurse Retentioncdayxnzcf100% (2)
- Physician Leaders of Medical Groups Face Increasing ChallengesDocument6 pagesPhysician Leaders of Medical Groups Face Increasing ChallengesAli RajaNo ratings yet
- Cvs Health Current and New Approaches To Making Drugs More AffordableDocument18 pagesCvs Health Current and New Approaches To Making Drugs More AffordableChrisball Dieter Inga RosalesNo ratings yet
- LYRA Value Impact Workforce HealthDocument13 pagesLYRA Value Impact Workforce HealthThomas WhittyNo ratings yet
- Assignment TasksDocument4 pagesAssignment TasksMuhammad Faraz HasanNo ratings yet
- Accenture Health Caring Employees BusinessDocument27 pagesAccenture Health Caring Employees Businessashish21bba043No ratings yet
- Rethinking Nursing Productivity To Enhance Organizational Performance - Final - 2Document17 pagesRethinking Nursing Productivity To Enhance Organizational Performance - Final - 2deepak162162No ratings yet
- Ar 495309Document88 pagesAr 495309wang jiaminNo ratings yet
- High Value Physician Guide - 2010!10!1Document12 pagesHigh Value Physician Guide - 2010!10!1Jennifer ChristianNo ratings yet
- Use Digital To Improve Healthcare Today While Creating A New TomorrowDocument4 pagesUse Digital To Improve Healthcare Today While Creating A New TomorrowMuhammad BilalNo ratings yet
- Chapter 2 - Tools of Positive Analysis Brief Outline: Part 1 - Getting StartedDocument3 pagesChapter 2 - Tools of Positive Analysis Brief Outline: Part 1 - Getting StartedTâm Trần Thị MinhNo ratings yet
- Running Header: Change Management 1Document12 pagesRunning Header: Change Management 1David Fluky FlukyNo ratings yet
- Creating An Environment That Attracts Top Physician TalentDocument3 pagesCreating An Environment That Attracts Top Physician TalentMuhammad BilalNo ratings yet
- Hospital CEO Best Practices: A Ab BSST TR Ra Ac CT TDocument6 pagesHospital CEO Best Practices: A Ab BSST TR Ra Ac CT Tfrancisco_expósitoNo ratings yet
- Derma 2 Version FinalDocument19 pagesDerma 2 Version FinalMuhammad Huzaifa RizwanNo ratings yet
- Final Paper MCDocument11 pagesFinal Paper MCapi-254038474No ratings yet
- The Cost of Wellness: A WELCOA Expert Interview With Dr. Ron GoetzelDocument4 pagesThe Cost of Wellness: A WELCOA Expert Interview With Dr. Ron GoetzelDonna HughesNo ratings yet
- Fall 2014 On RoundsDocument60 pagesFall 2014 On RoundsCCHSNo ratings yet
- StrengthbasedleadershipDocument7 pagesStrengthbasedleadershipapi-317112346No ratings yet
- Take Home ExamsDocument4 pagesTake Home Examshcny46wsjjNo ratings yet
- Students-Assignment-Sheet Nursing FormatDocument3 pagesStudents-Assignment-Sheet Nursing FormatMARY JOYCE S. HERNANDEZNo ratings yet
- Chairman: Director of Higher Education Vice-Chairman: Chairman of The Professional Members: Chairman: Pathologist, MembersDocument3 pagesChairman: Director of Higher Education Vice-Chairman: Chairman of The Professional Members: Chairman: Pathologist, MembersNiña Michelle AbeNo ratings yet
- Block Chain in HealthcareDocument1 pageBlock Chain in Healthcarenikitha2007No ratings yet
- Gov. Gretchen Whitmer's Letter To President BidenDocument2 pagesGov. Gretchen Whitmer's Letter To President BidenClickon DetroitNo ratings yet
- Etiqa Step by Step Guide For Availment and ReimbursementDocument18 pagesEtiqa Step by Step Guide For Availment and Reimbursementdauzjenny42No ratings yet
- BSN 4 PartialDocument3 pagesBSN 4 PartialJames AbendanNo ratings yet
- Case StudyDocument2 pagesCase StudyNetanya AlfadNo ratings yet
- Pharmacy Benefit Management HAAD ExqmDocument3 pagesPharmacy Benefit Management HAAD Exqmqariasif1900No ratings yet
- ProfileDocument2 pagesProfileHemant UpadhyayNo ratings yet
- Home Visit Reflection SamplesDocument9 pagesHome Visit Reflection SamplesJasmine CorreosNo ratings yet
- Healthcare Delivery System NotesDocument7 pagesHealthcare Delivery System NotesYsabellaPlarisanNo ratings yet
- Presentation On Hospital Management PolicyDocument11 pagesPresentation On Hospital Management PolicyMiriam ChristopherNo ratings yet
- Teaching AssignmentDocument7 pagesTeaching Assignment9pk8kk69jsNo ratings yet
- Mental Health Services in CubaDocument4 pagesMental Health Services in CubaKevin HancockNo ratings yet
- PART A Reflective CommunicationDocument5 pagesPART A Reflective CommunicationEvanNo ratings yet
- MBBSDocument5 pagesMBBSRajashree RNo ratings yet
- Christine Curamen: EducationDocument2 pagesChristine Curamen: Educationatty.elmanotarypublicNo ratings yet
- Jadwal Piket Poned 2022Document4 pagesJadwal Piket Poned 2022dara dwiNo ratings yet
- Gondiya MTPDocument1 pageGondiya MTPAbhishek Motiram JagtapNo ratings yet
- Ayushman Bharat - Pradhan Mantri Jan Arogya YojanaDocument3 pagesAyushman Bharat - Pradhan Mantri Jan Arogya YojanaRishitha NaveenkumarNo ratings yet
- MOM FileDocument24 pagesMOM FileNoor ButtNo ratings yet
- Written Assig Unit 5Document5 pagesWritten Assig Unit 5bnvjNo ratings yet
- cms1500 FormDocument2 pagescms1500 FormpalashNo ratings yet
- Sourav Mondal Assignment - 2Document91 pagesSourav Mondal Assignment - 2Cihhm Trainning & PlacementNo ratings yet
- Role of Care GiversDocument4 pagesRole of Care GiversJisna AlbyNo ratings yet
- DSP-List NamibiaDocument10 pagesDSP-List NamibiaPerera KusalNo ratings yet
- The Nature of Policy ChangeDocument2 pagesThe Nature of Policy ChangeArsh AhmadNo ratings yet
- Kashish KewalramaniDocument36 pagesKashish Kewalramanipriyanshu kesarwaniNo ratings yet
- Group Hospital and Surgical Claim FormDocument4 pagesGroup Hospital and Surgical Claim FormYiki TanNo ratings yet
- Ethics Documents For Physio TherapistsDocument21 pagesEthics Documents For Physio TherapistsDeeksha JainNo ratings yet