You might also like
- Pygas Product Safety SummaryDocument3 pagesPygas Product Safety SummaryBagus Wahyu MurtiantoNo ratings yet
- Application For Provident Benefits (Apb) ClaimDocument2 pagesApplication For Provident Benefits (Apb) ClaimJoey Singson100% (1)
- Application For License To Operate A General Clinical LaboratoryDocument6 pagesApplication For License To Operate A General Clinical LaboratoryAlianna Arnica MambataoNo ratings yet
- Using SSPC Coating Material Standards 1Document18 pagesUsing SSPC Coating Material Standards 1achusanachu100% (1)
- CARPER LAD FormNo.70 Inventory of Existing CCLOADocument1 pageCARPER LAD FormNo.70 Inventory of Existing CCLOARobert WeissNo ratings yet
- RMO Claim FormDocument1 pageRMO Claim FormNirubhana ArunthavasothyNo ratings yet
- CataratanDocument6 pagesCataratanAlodia RiveraNo ratings yet
- Addendum AE UPODocument1 pageAddendum AE UPOVEER ERINGNo ratings yet
- Government of West Bengal Health Family Welfare Department National Health Mission (NHM) GN - 29, 2 FloorDocument10 pagesGovernment of West Bengal Health Family Welfare Department National Health Mission (NHM) GN - 29, 2 FloorNicolas FabianNo ratings yet
- UPDATE FORM PensionersDocument2 pagesUPDATE FORM PensionersMahaplag FS BfpNo ratings yet
- Winston Field Validation Cervantes 3Document4 pagesWinston Field Validation Cervantes 3Dave Matthew AbellaNo ratings yet
- AO 1 GUIDELINES SIMPLIFYING THE LAND ACQUISITION AND DISTRIBUTION PROCESS ON CARP-COVERED PRIVATE AGRICULTURAL LANDS-merged-2 PDFDocument35 pagesAO 1 GUIDELINES SIMPLIFYING THE LAND ACQUISITION AND DISTRIBUTION PROCESS ON CARP-COVERED PRIVATE AGRICULTURAL LANDS-merged-2 PDFMer CyNo ratings yet
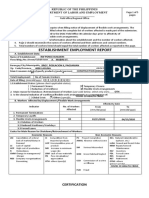
- Establishment Employment ReportDocument7 pagesEstablishment Employment ReportRW Ponce BuildersNo ratings yet
- Profile of Displaced Workers (Informal Sector Workers) : Department of Labor and EmploymentDocument1 pageProfile of Displaced Workers (Informal Sector Workers) : Department of Labor and EmploymentDrake ManNo ratings yet
- Kardex: GCS: 12-13/15 (M:5, V:4-5, E:3)Document11 pagesKardex: GCS: 12-13/15 (M:5, V:4-5, E:3)Dienizs Labini TadenaNo ratings yet
- Old Users With ProblemsDocument2 pagesOld Users With Problemselena.robles001No ratings yet
- Niug NorteDocument6 pagesNiug NorteAlodia RiveraNo ratings yet
- Informal S. Form No. 1: Aklan Field OfficeDocument1 pageInformal S. Form No. 1: Aklan Field OfficeMohammad Sa-ad L IndarNo ratings yet
- CARPER LAD Form No. 70Document1 pageCARPER LAD Form No. 70skar lett100% (1)
- NPQSD CSF-Ver2Document1 pageNPQSD CSF-Ver2Eduardo CasesNo ratings yet
- LPC - of - L.T. Lalrinmawia April-2023Document2 pagesLPC - of - L.T. Lalrinmawia April-2023David ZD ChawngthuNo ratings yet
- Jurisdiction DetailsDocument7 pagesJurisdiction DetailstvsshindeNo ratings yet
- For Instructions, See Back of Form: NJV - Indexed AuditedDocument1 pageFor Instructions, See Back of Form: NJV - Indexed AuditedZach EdwardsNo ratings yet
- Ob Ward Duty PapersDocument29 pagesOb Ward Duty PapersJeann ManlangitNo ratings yet
- AMF CRM FormatDocument2 pagesAMF CRM FormatNarasimman NarayananNo ratings yet
- Update Form SurvivorsDocument2 pagesUpdate Form SurvivorsAbbie NunezNo ratings yet
- DENR-EMB QSMR 1st Quarter Jan-Mar2020Document8 pagesDENR-EMB QSMR 1st Quarter Jan-Mar2020Jennifer DYNo ratings yet
- Establishment Employment Report RKS-Form5Document2 pagesEstablishment Employment Report RKS-Form5Richelle WskiNo ratings yet
- Data of Interview TodayDocument3 pagesData of Interview TodayManjeet SinghNo ratings yet
- First Congressional District of Iowa COPE AFL-CIO - 6127 - ScannedDocument4 pagesFirst Congressional District of Iowa COPE AFL-CIO - 6127 - ScannedZach EdwardsNo ratings yet
- FoP Session 3 CRFs Computer FillDocument4 pagesFoP Session 3 CRFs Computer FillMustafa Al-SayadNo ratings yet
- 70-E.1 Alternative Lot Allocation AgreementDocument3 pages70-E.1 Alternative Lot Allocation AgreementRome VonhartNo ratings yet
- CAF 2012 Form 25Document6 pagesCAF 2012 Form 25jeremydejesusNo ratings yet
- Scorecard TemplateDocument3 pagesScorecard TemplateJessilou LagonNo ratings yet
- PASS Data Capture Form 2021Document8 pagesPASS Data Capture Form 2021Rhea TiemsemNo ratings yet
- 2003-07-08 DR2 SummaryDocument2 pages2003-07-08 DR2 SummaryZach EdwardsNo ratings yet
- Quarterly Reports 2021Document58 pagesQuarterly Reports 2021Joemar CafrancaNo ratings yet
- Scan Aug 21, 2020Document1 pageScan Aug 21, 2020maheshkumarNo ratings yet
- Register Formats For GP FinalDocument58 pagesRegister Formats For GP FinalCHAPORERPAR-II GPNo ratings yet
- Map Description of The Existing SystemDocument6 pagesMap Description of The Existing SystemYibe WkNo ratings yet
- Shearline RHASDocument2 pagesShearline RHASMarie JeanNo ratings yet
- CARPER-LAD-FormNo.70-B - REVISED FIELD VALIDATION REPORTDocument4 pagesCARPER-LAD-FormNo.70-B - REVISED FIELD VALIDATION REPORTjencaringggNo ratings yet
- CAF 2012 Form 26Document6 pagesCAF 2012 Form 26jeremydejesusNo ratings yet
- FHSIS Report Forms A1 M1 Q1 All ProgramsDocument70 pagesFHSIS Report Forms A1 M1 Q1 All ProgramsmynameissaiNo ratings yet
- Delartment: @luutionDocument13 pagesDelartment: @luutionLambino Adonis HiramiaNo ratings yet
- Name Received Collected Dummy N168: InterpretationDocument2 pagesName Received Collected Dummy N168: InterpretationSs LaptopNo ratings yet
- Performance Output: Employee: Edelia S. Gonoy Mpdo/MenroDocument1 pagePerformance Output: Employee: Edelia S. Gonoy Mpdo/MenroMeljoy Montecillo Yorong CabatuanNo ratings yet
- Revised Format of Physical-Life CertificateDocument3 pagesRevised Format of Physical-Life CertificatePrabhat SinghNo ratings yet
- CARPER-LAD-FormNo.70-G RQST FOR GNRTN RGSTRN ISSUANCE FEB2021Document1 pageCARPER-LAD-FormNo.70-G RQST FOR GNRTN RGSTRN ISSUANCE FEB2021jencaringggNo ratings yet
- Pulses Importers 10.12.2019 PDFDocument177 pagesPulses Importers 10.12.2019 PDFsureshNo ratings yet
- (Notification-Cum-Prospectus No:) : Only For FemaleDocument3 pages(Notification-Cum-Prospectus No:) : Only For FemaleDinesh kumarNo ratings yet
- Petrol Pump List of Locations - 2023Document90 pagesPetrol Pump List of Locations - 2023towaf57520No ratings yet
- Instructions, See Back of For CK One: DR-1 OF: This Is Initial This Is Amended" Reset - Form For OfficeDocument1 pageInstructions, See Back of For CK One: DR-1 OF: This Is Initial This Is Amended" Reset - Form For OfficeZach EdwardsNo ratings yet
- National Biogas & Manure Management ProgrammeDocument4 pagesNational Biogas & Manure Management ProgrammeNITIN SHARMANo ratings yet
- Delegation of Fin Powers - 92Document5 pagesDelegation of Fin Powers - 92BhavithavNo ratings yet
- Courtesy Lane Passport Application Form FillableDocument1 pageCourtesy Lane Passport Application Form Fillable9cwkwgccdjNo ratings yet
- Courtesy Lane Passport Application Form FillableDocument1 pageCourtesy Lane Passport Application Form Fillabledhie bumNo ratings yet
- Vawc Form2Document1 pageVawc Form2Kookie KokoyNo ratings yet
- Department of Labor and Employment Caraga Regional OfficeDocument1 pageDepartment of Labor and Employment Caraga Regional OfficechoyNo ratings yet
- Philippine Electrical CodeDocument14 pagesPhilippine Electrical CodeJohn Oyan EstilloreNo ratings yet
- Appointment RecieptDocument1 pageAppointment Recieptaqil faizanNo ratings yet
- Lovely LungsDocument6 pagesLovely Lungsapi-285970439No ratings yet
- Ethics in Clinical TrialDocument28 pagesEthics in Clinical TrialRanjeet PrasadNo ratings yet
- (Susan Aldridge) The Thread of Life The Story ofDocument272 pages(Susan Aldridge) The Thread of Life The Story ofsergioNo ratings yet
- Chapter 4 Scintillation Detectors: 4.1. Basic Principle of The ScintillatorDocument10 pagesChapter 4 Scintillation Detectors: 4.1. Basic Principle of The ScintillatorbbkanilNo ratings yet
- IPM Indore 2022 Original Paper With Answer KeyDocument19 pagesIPM Indore 2022 Original Paper With Answer KeyGod Plan100% (1)
- Delight in Sight: Corneal Topographer Tms-4NDocument2 pagesDelight in Sight: Corneal Topographer Tms-4NWaleed Ah-DhaifiNo ratings yet
- COMEDK UGET-2011 Medical Rank ListDocument147 pagesCOMEDK UGET-2011 Medical Rank ListiamvarkeyNo ratings yet
- Indumax CLS54D EN - 0218Document12 pagesIndumax CLS54D EN - 0218Carlos LeonNo ratings yet
- 4099 0002Document4 pages4099 0002kikeecpNo ratings yet
- Collection Plan 7134Document57 pagesCollection Plan 7134Tony CombsNo ratings yet
- Nursing Care Plan: Chronic Pain and COPDDocument11 pagesNursing Care Plan: Chronic Pain and COPDneuronurse100% (1)
- Water Demand All SlidesDocument23 pagesWater Demand All Slidesrajat debnathNo ratings yet
- Final Examination Rubric On The Zumba Exercises RoutineDocument1 pageFinal Examination Rubric On The Zumba Exercises RoutinePizzaTobacco123100% (1)
- Pnoz S2 24Vdc 3 N/O 1 N/C 750102: Pilz GMBH & Co. KG, Felix-Wankel-Strasse 2, 73760 Ostfildern, Germany Page 1/3Document3 pagesPnoz S2 24Vdc 3 N/O 1 N/C 750102: Pilz GMBH & Co. KG, Felix-Wankel-Strasse 2, 73760 Ostfildern, Germany Page 1/3Ibraheem AlfalahatNo ratings yet
- Catherine DunbarDocument2 pagesCatherine Dunbardylanmore1223No ratings yet
- The Current Status of The "Food Security Doctrine" Implementation in The Russian Federation and Tasks For 2013-2020Document5 pagesThe Current Status of The "Food Security Doctrine" Implementation in The Russian Federation and Tasks For 2013-2020gautham28No ratings yet
- Site Selection Criteria For Coal Power PlantsDocument7 pagesSite Selection Criteria For Coal Power Plantsmrizvi33No ratings yet
- Brain Breaks: Animal WalksDocument6 pagesBrain Breaks: Animal WalksMárcia DiasNo ratings yet
- Mind Blowing Magic Collection PDFDocument41 pagesMind Blowing Magic Collection PDFjules629450% (2)
- Golf Pei Course Comparison ChartDocument1 pageGolf Pei Course Comparison ChartSteve DimondNo ratings yet
- Bkf1243-Analytical Chemistry 21314 PDFDocument9 pagesBkf1243-Analytical Chemistry 21314 PDFrushdiNo ratings yet
- Tds 108277427 ProMix PCE 300Document3 pagesTds 108277427 ProMix PCE 300Chetal BholeNo ratings yet
- 2018 - Shiau - Evaluation of A Flipped Classroom Approach To Learning Introductory EpidemiologyDocument9 pages2018 - Shiau - Evaluation of A Flipped Classroom Approach To Learning Introductory EpidemiologySocorro Moreno LunaNo ratings yet
- Method Used For The Prevention of RustingDocument9 pagesMethod Used For The Prevention of RustingSaadiah MohammadNo ratings yet
- Lifespan Development Lives in Context 1st Edition Kuther Solutions ManualDocument8 pagesLifespan Development Lives in Context 1st Edition Kuther Solutions Manualgiangdoankqb1rc100% (34)
- Foundations of Group BehaviorDocument31 pagesFoundations of Group BehaviorRaunakNo ratings yet