You might also like
- DR - Sundaravadivel Trichy PMFDocument2 pagesDR - Sundaravadivel Trichy PMFNarasimman NarayananNo ratings yet
- Nest Pharma Tour Programme Name: HQ: Date Day Work PlannedDocument35 pagesNest Pharma Tour Programme Name: HQ: Date Day Work PlannedtomeshNo ratings yet
- Regd. Office: Vidyutbhawan, Jyoti Nagar, Jaipur 302005 Tele-Fax: +91-141-2740455, Website: WWW - Rvpn.Co - inDocument1 pageRegd. Office: Vidyutbhawan, Jyoti Nagar, Jaipur 302005 Tele-Fax: +91-141-2740455, Website: WWW - Rvpn.Co - invinodk33506No ratings yet
- Survery Off Report ProformaDocument1 pageSurvery Off Report ProformaaditiNo ratings yet
- BPLO - Unified Application Form For Business Permit NEW BUSINESS PERMIT 2023Document3 pagesBPLO - Unified Application Form For Business Permit NEW BUSINESS PERMIT 2023Jlj ChuaNo ratings yet
- New Joinee TrackerDocument10 pagesNew Joinee TrackerSundaravel ChelladuraiNo ratings yet
- SOA PhilHealthDocument1 pageSOA PhilHealthMilagrosBautistaNo ratings yet
- Vendor Data To Be Completed by Requestor (TNB Department/Subsidiary)Document4 pagesVendor Data To Be Completed by Requestor (TNB Department/Subsidiary)Mohd Kahirol NizamNo ratings yet
- LicenceDocument6 pagesLicencePremananth ANo ratings yet
- DeoriaDocument5 pagesDeoriaArvind TomarNo ratings yet
- Item Code Quantity UOM Description Stock / Non Stock Item Estimated Unit Cost ($) Total Cost ($)Document2 pagesItem Code Quantity UOM Description Stock / Non Stock Item Estimated Unit Cost ($) Total Cost ($)DILNo ratings yet
- License CT CathDocument7 pagesLicense CT CathHappylifeNo ratings yet
- GeM Bidding 6215082Document5 pagesGeM Bidding 6215082myname nameNo ratings yet
- Nama Vendor: PT. Wahana Karsa Sinergi Manual and Procedure (Request To Vendor) Not To Be Copied Without Permision Job Order For Vendor OutsourcingDocument4 pagesNama Vendor: PT. Wahana Karsa Sinergi Manual and Procedure (Request To Vendor) Not To Be Copied Without Permision Job Order For Vendor OutsourcingAndre MahardhikaNo ratings yet
- Project Procurement Management PlanDocument8 pagesProject Procurement Management PlanRoderick MalubagNo ratings yet
- Distriphil Cif FormDocument3 pagesDistriphil Cif Formjimabil ramirezNo ratings yet
- GeM Bidding 3261984Document5 pagesGeM Bidding 3261984masoodNo ratings yet
- Sample Form: DNB - CardiologyDocument6 pagesSample Form: DNB - CardiologypradeephdNo ratings yet
- Dr. Varsha Rangari Pune-2 SAS UpdatedDocument9 pagesDr. Varsha Rangari Pune-2 SAS UpdatedSantosh BoradeNo ratings yet
- Basic Details: Date: 10-Jul-2019 02:25 AMDocument2 pagesBasic Details: Date: 10-Jul-2019 02:25 AMAnonymous NJDmHvjNo ratings yet
- Item Code Quantity UOM Description Stock / Non Stock Item Estimated Unit Cost ($) Total Cost ($)Document6 pagesItem Code Quantity UOM Description Stock / Non Stock Item Estimated Unit Cost ($) Total Cost ($)DILNo ratings yet
- FP 01 Application Form For New RecruitsDocument4 pagesFP 01 Application Form For New Recruitsthakurvikas434No ratings yet
- GeM Bidding 6006058Document6 pagesGeM Bidding 6006058mepNo ratings yet
- I Would Like To Apply For Accreditation As:: AF-PCN-A1Document3 pagesI Would Like To Apply For Accreditation As:: AF-PCN-A1ThE EyE KaRmANo ratings yet
- Pco Application For Accreditation For New RenewalDocument3 pagesPco Application For Accreditation For New RenewalcharleneNo ratings yet
- Form 4-06Document1 pageForm 4-06Priscilla BacunganNo ratings yet
- Bihar Gramin Bank: Region: Lakhisarai Branch / Office: Branch / Office Ref. No. DateDocument3 pagesBihar Gramin Bank: Region: Lakhisarai Branch / Office: Branch / Office Ref. No. DateAvinash SinghNo ratings yet
- SN Checklist Items Remarks: Site Visit Checklist GuideDocument2 pagesSN Checklist Items Remarks: Site Visit Checklist GuideRoseNo ratings yet
- Form 1 BCLTE EOPT Mandatory RegistrantsDocument1 pageForm 1 BCLTE EOPT Mandatory RegistrantsRapha JohnNo ratings yet
- Policy Amendment Request Form PARF For Individual PolicyownerDocument6 pagesPolicy Amendment Request Form PARF For Individual PolicyownerCamille FreoNo ratings yet
- Application Form - 144Document6 pagesApplication Form - 144Pankaj SalunkheNo ratings yet
- Application Form - 1Document6 pagesApplication Form - 1Pankaj SalunkheNo ratings yet
- FM-CSVlrd-01 S2 Application Rev 0 April 30 2018 02AUG2018Document2 pagesFM-CSVlrd-01 S2 Application Rev 0 April 30 2018 02AUG2018Noel IV T. Borromeo50% (4)
- D3 Application Form For Renewal-UpdatedDocument3 pagesD3 Application Form For Renewal-UpdatedFlorence Benette Gallego100% (1)
- GeM Bidding 5545117Document7 pagesGeM Bidding 5545117rakeshNo ratings yet
- HardoiDocument5 pagesHardoiArvind TomarNo ratings yet
- Qud 0014 R1 PDFDocument1 pageQud 0014 R1 PDFcdnaveenNo ratings yet
- Advance Payment Requisition Form: Customer Vendor OthersDocument1 pageAdvance Payment Requisition Form: Customer Vendor OthersSMTT WORK OFFICIALNo ratings yet
- GPF CPF Advance FormDocument2 pagesGPF CPF Advance FormMuhammad Rameez SialNo ratings yet
- PSR&LLDocument15 pagesPSR&LLZain AbidiNo ratings yet
- For Printing - A4Document5 pagesFor Printing - A4Andie GalangNo ratings yet
- Customer Application FormDocument2 pagesCustomer Application Formartha permataNo ratings yet
- Phenyl (1400) : Bid Document Bid DetailsDocument2 pagesPhenyl (1400) : Bid Document Bid DetailsRajatMerchantNo ratings yet
- History Sheet-Development - Nichi-InDocument2 pagesHistory Sheet-Development - Nichi-Inswapnilpa1122No ratings yet
- Item Code Quantity UOM Description Stock / Non Stock Item Estimated Unit Cost ($) Total Cost ($)Document2 pagesItem Code Quantity UOM Description Stock / Non Stock Item Estimated Unit Cost ($) Total Cost ($)DILNo ratings yet
- Application Form For Accreditation, OSH Practitioner, ConsultantDocument3 pagesApplication Form For Accreditation, OSH Practitioner, ConsultantTOTSNo ratings yet
- GeM Bidding 5674803Document7 pagesGeM Bidding 5674803givejiw432No ratings yet
- QW 33333333 XeeaDocument1 pageQW 33333333 XeeaDharryl Dharryl DharrylNo ratings yet
- s2 ApplicationDocument2 pagess2 ApplicationIze MarieNo ratings yet
- Extra Duty Claim Form For Surgery STHDocument2 pagesExtra Duty Claim Form For Surgery STHZieshNo ratings yet
- Application Form For Accreditation, OSH Practitioner, ConsultantDocument3 pagesApplication Form For Accreditation, OSH Practitioner, ConsultantLyn EscanoNo ratings yet
- GeM Bidding 6198946Document4 pagesGeM Bidding 6198946subrata sarkarNo ratings yet
- R-PRC-001-007 PR Form For Colleagues Latest VersionDocument1 pageR-PRC-001-007 PR Form For Colleagues Latest VersionSiu Fai LONo ratings yet
- Uttar Haryana Bijli Vitran Nigam Sales Instruction No. U-15 /2014Document5 pagesUttar Haryana Bijli Vitran Nigam Sales Instruction No. U-15 /2014GouravKhartaNo ratings yet
- Water Sampling - 0631 - Pgo (1188)Document1 pageWater Sampling - 0631 - Pgo (1188)Mark Arthur MarteNo ratings yet
- GeM Bidding 5965676Document5 pagesGeM Bidding 5965676NE-II Circle Electrical Division - DimapurNo ratings yet
- AC 2.1 Application Form and Accreditation Agreement V9.1Document11 pagesAC 2.1 Application Form and Accreditation Agreement V9.1Ahmad ENo ratings yet
- Pillar Drilling Machine 25 MMDocument1 pagePillar Drilling Machine 25 MMArun KumarNo ratings yet
- Particulars April MAY JUN JUL AUG SEP Trichy Achievement DetailsDocument2 pagesParticulars April MAY JUN JUL AUG SEP Trichy Achievement DetailsNarasimman NarayananNo ratings yet
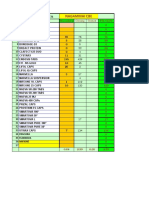
- CBE 10 DRS FOR CONVERSION DecDocument4 pagesCBE 10 DRS FOR CONVERSION DecNarasimman NarayananNo ratings yet
- Nagammai StatementReportDocument1 pageNagammai StatementReportNarasimman NarayananNo ratings yet
- CBE BUSINESS PLANNING Dec 18Document11 pagesCBE BUSINESS PLANNING Dec 18Narasimman NarayananNo ratings yet
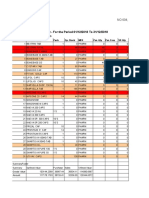
- Stock and Sales Statement - For The Period 01/12/2018 To 31/12/2018Document6 pagesStock and Sales Statement - For The Period 01/12/2018 To 31/12/2018Narasimman NarayananNo ratings yet
- TRICHY RGION BUSINESS PLANNING Dec 18Document9 pagesTRICHY RGION BUSINESS PLANNING Dec 18Narasimman NarayananNo ratings yet
- Business Planning Mar'2020Document16 pagesBusiness Planning Mar'2020Narasimman NarayananNo ratings yet
- PMF DRS Support Feb'2020Document6 pagesPMF DRS Support Feb'2020Narasimman NarayananNo ratings yet
- Stockistwise SecDocument93 pagesStockistwise SecNarasimman NarayananNo ratings yet
- PMF DRS Support Feb'2020Document6 pagesPMF DRS Support Feb'2020Narasimman NarayananNo ratings yet
- Business Planning Mar'2020Document16 pagesBusiness Planning Mar'2020Narasimman NarayananNo ratings yet
- PMF DRS Support Feb'2020Document6 pagesPMF DRS Support Feb'2020Narasimman NarayananNo ratings yet
- Head Qtr. Dr. Name Speciality Area: Business Value (In PTS) Apr-19Document6 pagesHead Qtr. Dr. Name Speciality Area: Business Value (In PTS) Apr-19Narasimman NarayananNo ratings yet
- PMF DRS SupportDocument6 pagesPMF DRS SupportNarasimman NarayananNo ratings yet
- Business Planning Mar'2020Document16 pagesBusiness Planning Mar'2020Narasimman NarayananNo ratings yet
- ParvathyDocument2 pagesParvathyNarasimman NarayananNo ratings yet
- Business Tracker Cuddalore Feb'2020Document45 pagesBusiness Tracker Cuddalore Feb'2020Narasimman NarayananNo ratings yet
- Coimbatoe JAN 2018 SEC. Format SECONDARY. CLOSINGDocument9 pagesCoimbatoe JAN 2018 SEC. Format SECONDARY. CLOSINGNarasimman NarayananNo ratings yet
- Coimbatoe Empty Format SECONDARY. CLOSINGDocument9 pagesCoimbatoe Empty Format SECONDARY. CLOSINGNarasimman NarayananNo ratings yet
- Nagammai StatementReport PDFDocument1 pageNagammai StatementReport PDFNarasimman NarayananNo ratings yet
- PMF DRS Support Feb'2020Document6 pagesPMF DRS Support Feb'2020Narasimman NarayananNo ratings yet
- Business Tracker Cuddalore Feb'2020Document45 pagesBusiness Tracker Cuddalore Feb'2020Narasimman NarayananNo ratings yet
- Manager Work Analysis: Name of Manager: K.VIBASUKAMAN Desig:RBM HQ: Chennai APR MAY JUN JULDocument8 pagesManager Work Analysis: Name of Manager: K.VIBASUKAMAN Desig:RBM HQ: Chennai APR MAY JUN JULNarasimman NarayananNo ratings yet
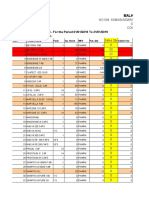
- BalajiDocument6 pagesBalajiNarasimman NarayananNo ratings yet
- PMF DRS SupportDocument6 pagesPMF DRS SupportNarasimman NarayananNo ratings yet
- Business Tracker Cuddalore Feb'2020Document45 pagesBusiness Tracker Cuddalore Feb'2020Narasimman NarayananNo ratings yet
- Manager Work Analysis: Name of Manager: K.VIBASUKAMAN Desig:RBM HQ: Chennai APR MAY JUN JULDocument8 pagesManager Work Analysis: Name of Manager: K.VIBASUKAMAN Desig:RBM HQ: Chennai APR MAY JUN JULNarasimman NarayananNo ratings yet
- Business Tracker Cuddalore Feb'2020Document45 pagesBusiness Tracker Cuddalore Feb'2020Narasimman NarayananNo ratings yet
- PMF DRS SupportDocument6 pagesPMF DRS SupportNarasimman NarayananNo ratings yet
- Business Planning Mar'2020Document16 pagesBusiness Planning Mar'2020Narasimman NarayananNo ratings yet
- Sales Engineer in Rochester NY Resume Lance DumiganDocument2 pagesSales Engineer in Rochester NY Resume Lance DumiganLanceDumiganNo ratings yet
- Threat and Risk Assessment TemplateDocument30 pagesThreat and Risk Assessment TemplateMarija PetkovicNo ratings yet
- This Research Paper Is Written by Naveed Iqbal ChaudhryDocument5 pagesThis Research Paper Is Written by Naveed Iqbal ChaudhryAleem MalikNo ratings yet
- Acctg 202 Di Pa FinalDocument10 pagesAcctg 202 Di Pa FinalJoshua CabinasNo ratings yet
- Distance Learning 2016 Telecom AcademyDocument17 pagesDistance Learning 2016 Telecom AcademyDyego FelixNo ratings yet
- CH 8Document64 pagesCH 8Anonymous 0cdKGOBBNo ratings yet
- Product Differentiation and Market Segmentation As Alternative Marketing StrategiesDocument7 pagesProduct Differentiation and Market Segmentation As Alternative Marketing Strategiesshoka1388No ratings yet
- Announcement Invitation For Psychotest (October)Document17 pagesAnnouncement Invitation For Psychotest (October)bgbfbvmnmNo ratings yet
- Utility BillDocument1 pageUtility BillIsaiah Kipyego0% (1)
- Godown Creation in Tally 9 Tutorial Youtube PDFDocument3 pagesGodown Creation in Tally 9 Tutorial Youtube PDFKristinNo ratings yet
- Issue 7: October 1998Document68 pagesIssue 7: October 1998Iin Mochamad SolihinNo ratings yet
- Defining Social InnovationDocument15 pagesDefining Social InnovationFasyaAfifNo ratings yet
- World Airports Freighters: FreighDocument16 pagesWorld Airports Freighters: FreighBobbie KhunthongchanNo ratings yet
- Example of RFP For Credit ScoringDocument4 pagesExample of RFP For Credit ScoringadaquilaNo ratings yet
- 10 Steps To Precision Maintenance Reliability SuccessDocument11 pages10 Steps To Precision Maintenance Reliability SuccessElvis DiazNo ratings yet
- Hire Purchase SystemDocument13 pagesHire Purchase SystemDeepak Dhingra100% (1)
- Laguna y Markklund PDFDocument668 pagesLaguna y Markklund PDFjuan carlos sanchezNo ratings yet
- B2B E-Marketplace Adoption in Agriculture: Zheng XiaopingDocument8 pagesB2B E-Marketplace Adoption in Agriculture: Zheng XiaopingNikhil MalhotraNo ratings yet
- Paying Quantities Key & Charest - CLE - Oil and Gas Disputes 2019Document22 pagesPaying Quantities Key & Charest - CLE - Oil and Gas Disputes 2019Daniel CharestNo ratings yet
- 1 Zong Net Package PDFDocument8 pages1 Zong Net Package PDFHafiz Abid Malik0% (1)
- Permission To MortgageDocument14 pagesPermission To MortgageAabad BrandNo ratings yet
- Business Plan On HIRING A MAIDDocument21 pagesBusiness Plan On HIRING A MAIDharsha100% (1)
- Sameer Amale, Mohsin Dalvi - Industrial Relations and Collective Bargaining, Ethics and Justice in HRMDocument71 pagesSameer Amale, Mohsin Dalvi - Industrial Relations and Collective Bargaining, Ethics and Justice in HRMmohsindalvi87No ratings yet
- Managerial Economics and Business Strategy, 8E Baye Chap. 3Document36 pagesManagerial Economics and Business Strategy, 8E Baye Chap. 3love75% (4)
- Microsoft Project Training ManualDocument15 pagesMicrosoft Project Training ManualAfif Kamal Fiska100% (1)
- Okayyss Lang - SadDocument28 pagesOkayyss Lang - SadEngelbert Lutao PalisNo ratings yet
- Plan Bee Project To Empower 20 Women in Chitral Proposal - 10!12!2016Document17 pagesPlan Bee Project To Empower 20 Women in Chitral Proposal - 10!12!2016Cristal Montanez100% (1)
- Soga 37Document2 pagesSoga 37JohnsonBathNo ratings yet
- TCI Letter To Safran Chairman 2017-02-14Document4 pagesTCI Letter To Safran Chairman 2017-02-14marketfolly.comNo ratings yet
- ABS Summary TextDocument12 pagesABS Summary TextjesusmemNo ratings yet