You might also like
- Gale Researcher Guide for: The Frontal Lobe and Executive FunctionsFrom EverandGale Researcher Guide for: The Frontal Lobe and Executive FunctionsRating: 2 out of 5 stars2/5 (1)
- Stroke AssessmentDocument10 pagesStroke AssessmentUzra ShujaatNo ratings yet
- Sensory Reception-The Process of Recieving Stimuli or Data. This Stimuli Is EitherDocument7 pagesSensory Reception-The Process of Recieving Stimuli or Data. This Stimuli Is EitherJunaiza Adrayan MariNo ratings yet
- Glasgow Coma Scale Zen2Document7 pagesGlasgow Coma Scale Zen2Zen Firhan ShahabNo ratings yet
- Cognition and Perception - Neurological AssessmentDocument6 pagesCognition and Perception - Neurological AssessmentanditejoNo ratings yet
- Lab Act 1 - Motor AssessmentDocument6 pagesLab Act 1 - Motor AssessmentZgama AbdulrahmanNo ratings yet
- In General, Amputation of Limbs Is TheDocument11 pagesIn General, Amputation of Limbs Is TheCay Sevilla100% (1)
- A Simple Guide to Post-stroke Recovery, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Post-stroke Recovery, Diagnosis, Treatment and Related ConditionsNo ratings yet
- Unit 1Document9 pagesUnit 1Aaron Clarence CalimagNo ratings yet
- What Happens When You Touch the Body?: The Psychology of Body-Work.From EverandWhat Happens When You Touch the Body?: The Psychology of Body-Work.No ratings yet
- Mse 1Document27 pagesMse 1Ladybelle GototosNo ratings yet
- Impairments Associated With Traumatic Brain InjuryDocument3 pagesImpairments Associated With Traumatic Brain Injurykyoko08No ratings yet
- NUR 213 Weekly Care Plan StrokeDocument11 pagesNUR 213 Weekly Care Plan StrokeSarah MoffattNo ratings yet
- ASESSMENT of Client With Diseases in Nervous SystemDocument16 pagesASESSMENT of Client With Diseases in Nervous SystemChristian San Jose TanNo ratings yet
- IC ProsthesisDocument6 pagesIC ProsthesisTalles JesusNo ratings yet
- Unit 1 Introduction To The Human Body (2 Hours LEC/3 Hours LAB)Document4 pagesUnit 1 Introduction To The Human Body (2 Hours LEC/3 Hours LAB)knkjnNo ratings yet
- L7 Psychopathology and Symptomatology - HTDocument18 pagesL7 Psychopathology and Symptomatology - HTrajayasminNo ratings yet
- Assessment of The Nervous System - FinalDocument76 pagesAssessment of The Nervous System - FinalRona Lucido100% (1)
- Head To Toe AssessmentDocument56 pagesHead To Toe AssessmentAna95% (39)
- BioGeometry Shapes and Brain BalancingDocument13 pagesBioGeometry Shapes and Brain Balancingn13l13100% (15)
- Teaching Psychomotor SkillsDocument4 pagesTeaching Psychomotor SkillsKlara Abeja100% (1)
- Assessing The Musculoskeletal & Neurological SystemDocument34 pagesAssessing The Musculoskeletal & Neurological SystemalelichengNo ratings yet
- Head To Toe AssessmentDocument56 pagesHead To Toe AssessmentmisshieNo ratings yet
- The Single Most Important AssessmentDocument7 pagesThe Single Most Important Assessmenthellfire222No ratings yet
- Ten Daily Lessons Plan Unit 10. Reproductive System: Consuelo SnowDocument6 pagesTen Daily Lessons Plan Unit 10. Reproductive System: Consuelo SnowBryan S MaderaNo ratings yet
- Neurological AssessmentDocument10 pagesNeurological AssessmentKristine AlejandroNo ratings yet
- Mental Status ExaminationDocument10 pagesMental Status Examinationlatasha deshmukhNo ratings yet
- Neurological Exam Lecture NotesDocument26 pagesNeurological Exam Lecture NotesNaveen KovalNo ratings yet
- Assignment As 1 Intro To Anatomy: A. Give Your Responses To The FollowingDocument8 pagesAssignment As 1 Intro To Anatomy: A. Give Your Responses To The FollowingNINA NORELLE GALVEZNo ratings yet
- The Mental Status ExaminationDocument15 pagesThe Mental Status ExaminationDulce RodriguezNo ratings yet
- Module-2 UTSDocument46 pagesModule-2 UTSPaul Stephen SorianoNo ratings yet
- Lab Act 1 - Motor AssessmentDocument5 pagesLab Act 1 - Motor AssessmentJan Christian Gaudia 24No ratings yet
- Mental Status ExaminationDocument17 pagesMental Status ExaminationDharek IleshNo ratings yet
- Solution Manual For Seeleys Anatomy Physiology 12th Edition Cinnamon Vanputte Jennifer Regan Andrew Russo Rod Seeley Trent Stephens Philip TateDocument36 pagesSolution Manual For Seeleys Anatomy Physiology 12th Edition Cinnamon Vanputte Jennifer Regan Andrew Russo Rod Seeley Trent Stephens Philip Tateatworossel.qxwbv100% (46)
- Understanding Human Consciousness:: A Physiological ApproachDocument53 pagesUnderstanding Human Consciousness:: A Physiological ApproachJasvictorioNo ratings yet
- Daily Life Activities AssessmentDocument3 pagesDaily Life Activities AssessmentCristhian Agustin ParedesNo ratings yet
- Neurologic ExamDocument53 pagesNeurologic ExamRuaa HdeibNo ratings yet
- Cues Nursing Diagnosis Scientific Rationale Objectives Nursing Intervention Rationale EvaluationDocument3 pagesCues Nursing Diagnosis Scientific Rationale Objectives Nursing Intervention Rationale EvaluationDaniel Vergara ArceNo ratings yet
- Sensory Integration Processing Jargon GuideDocument4 pagesSensory Integration Processing Jargon Guideapi-660820048No ratings yet
- The Neurological Exam: Mental Status ExaminationDocument13 pagesThe Neurological Exam: Mental Status ExaminationShitaljit IromNo ratings yet
- Neuro Assessment: The Single Most Important AssessmentDocument10 pagesNeuro Assessment: The Single Most Important AssessmentpapadaadNo ratings yet
- Summary - Frogs Into PrincesDocument5 pagesSummary - Frogs Into PrincesMartinNo ratings yet
- MseDocument11 pagesMseClyde R.OrtegaNo ratings yet
- Paediatric Neurology:: Management Practices and Evidence Based PracticesDocument41 pagesPaediatric Neurology:: Management Practices and Evidence Based PracticesNikita ChaubeNo ratings yet
- Preperation Tasks - Week 2Document3 pagesPreperation Tasks - Week 2Άγγελος ΧαβέλαςNo ratings yet
- Module 3Document6 pagesModule 3Lawrence Jim BongstarNo ratings yet
- Physical Assessment On Musculosceletal SystemDocument14 pagesPhysical Assessment On Musculosceletal SystemilhamNo ratings yet
- Mental Status Examination: Level of ConsciousnessDocument4 pagesMental Status Examination: Level of Consciousnessmonica bayaoaNo ratings yet
- Psychology Individual AssignmentDocument9 pagesPsychology Individual Assignmentfiker tesfaNo ratings yet
- Activity 2.1: Organization of The BodyDocument5 pagesActivity 2.1: Organization of The BodyJustine PalasigueNo ratings yet
- Full Solution Manual For Seeleys Anatomy Physiology 12Th Edition Cinnamon Vanputte Jennifer Regan Andrew Russo Rod Seeley Trent Stephens Philip Tate 13 9781 PDF Docx Full Chapter ChapterDocument36 pagesFull Solution Manual For Seeleys Anatomy Physiology 12Th Edition Cinnamon Vanputte Jennifer Regan Andrew Russo Rod Seeley Trent Stephens Philip Tate 13 9781 PDF Docx Full Chapter Chapteryen.resiege.ffrq100% (15)
- Gender InequalityDocument9 pagesGender InequalityRhzNo ratings yet
- EgoismDocument3 pagesEgoism123014stephenNo ratings yet
- Physical Computing and Android in RoboticsDocument4 pagesPhysical Computing and Android in Roboticsnniikkoolliiccaa100% (1)
- 1300 Rev01Document15 pages1300 Rev01Manuel AltamiranoNo ratings yet
- Joshi C M, Vyas Y - Extensions of Certain Classical Integrals of Erdélyi For Gauss Hypergeometric Functions - J. Comput. and Appl. Mat. 160 (2003) 125-138Document14 pagesJoshi C M, Vyas Y - Extensions of Certain Classical Integrals of Erdélyi For Gauss Hypergeometric Functions - J. Comput. and Appl. Mat. 160 (2003) 125-138Renee BravoNo ratings yet
- Cee 2005 - 06Document129 pagesCee 2005 - 06iloveeggxPNo ratings yet
- DataStage Interview QuestionsDocument3 pagesDataStage Interview QuestionsvrkesariNo ratings yet
- Job Stress, Workload, Environment and Employee Turnover IntentionsDocument13 pagesJob Stress, Workload, Environment and Employee Turnover IntentionsYuni SasieNo ratings yet
- Heat Transfer Enhancement Using Nano FluidsDocument17 pagesHeat Transfer Enhancement Using Nano FluidsranjithkrajNo ratings yet
- Role of Wickability On The Critical Heat Flux of Structured Superhydrophilic SurfacesDocument10 pagesRole of Wickability On The Critical Heat Flux of Structured Superhydrophilic Surfacesavi0341No ratings yet
- Lesson 2 (Locating Main Ideas)Document18 pagesLesson 2 (Locating Main Ideas)Glyneth Dela TorreNo ratings yet
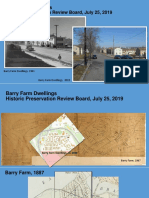
- Barry Farm Powerpoint SlidesDocument33 pagesBarry Farm Powerpoint SlidessarahNo ratings yet
- HS ĐỀ CƯƠNG KIỂM TRA GIỮA KỲ I KHOI 10 NH 23 24Document6 pagesHS ĐỀ CƯƠNG KIỂM TRA GIỮA KỲ I KHOI 10 NH 23 24Ngô Hiểu NhiênNo ratings yet
- Augmented FeedbackDocument54 pagesAugmented FeedbackAhmad KhuwarizmyNo ratings yet
- Transportation UnitDocument3 pagesTransportation UnitShannon MartinNo ratings yet
- What Are The Subjects Which Come in UPSC Engineering Services - Electronics - Communication - ExamDocument2 pagesWhat Are The Subjects Which Come in UPSC Engineering Services - Electronics - Communication - ExamVikas ChandraNo ratings yet
- My Publications and Workshops ListDocument4 pagesMy Publications and Workshops Listraviteja tankalaNo ratings yet
- Chapter 17Document78 pagesChapter 17Romar PanopioNo ratings yet
- Math Internal Assessment:: Investigating Parametric Equations in Motion ProblemsDocument16 pagesMath Internal Assessment:: Investigating Parametric Equations in Motion ProblemsByron JimenezNo ratings yet
- A Modified Newton's Method For Solving Nonlinear Programing ProblemsDocument15 pagesA Modified Newton's Method For Solving Nonlinear Programing Problemsjhon jairo portillaNo ratings yet
- D027B OmronDocument141 pagesD027B OmronirfanWPKNo ratings yet
- Matte Sanjeev Kumar: Professional SummaryDocument3 pagesMatte Sanjeev Kumar: Professional SummaryAlla VijayNo ratings yet
- Reserach MethoodolgyDocument38 pagesReserach MethoodolgyShubashPoojariNo ratings yet
- Heat and Cooling LoadDocument2 pagesHeat and Cooling LoadAshokNo ratings yet
- Non-Display Industrial Computers: User ManualDocument100 pagesNon-Display Industrial Computers: User ManualJason100% (1)
- Internship Report On Service IndustryDocument50 pagesInternship Report On Service Industrybbaahmad89No ratings yet
- Oracle Database Administrator TasksDocument2 pagesOracle Database Administrator TasksPratik GandhiNo ratings yet
- Mixed Methods Research PDFDocument14 pagesMixed Methods Research PDFChin Ing KhangNo ratings yet
- Partnerships Program For Education and Training (PAEC)Document6 pagesPartnerships Program For Education and Training (PAEC)LeslieNo ratings yet
- Canada Post ReportDocument202 pagesCanada Post ReportrgranatsteinNo ratings yet
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (32)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)From EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Rating: 3 out of 5 stars3/5 (1)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (404)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDFrom EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDRating: 5 out of 5 stars5/5 (3)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeRating: 2 out of 5 stars2/5 (1)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (170)
- Manipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesFrom EverandManipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesRating: 4.5 out of 5 stars4.5/5 (1412)
- Empath: The Survival Guide For Highly Sensitive People: Protect Yourself From Narcissists & Toxic Relationships. Discover How to Stop Absorbing Other People's PainFrom EverandEmpath: The Survival Guide For Highly Sensitive People: Protect Yourself From Narcissists & Toxic Relationships. Discover How to Stop Absorbing Other People's PainRating: 4 out of 5 stars4/5 (95)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 4.5 out of 5 stars4.5/5 (82)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 4 out of 5 stars4/5 (4)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsFrom EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo ratings yet
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (46)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisFrom EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisRating: 3.5 out of 5 stars3.5/5 (2)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4.5 out of 5 stars4.5/5 (6)
- The Twentysomething Treatment: A Revolutionary Remedy for an Uncertain AgeFrom EverandThe Twentysomething Treatment: A Revolutionary Remedy for an Uncertain AgeRating: 4.5 out of 5 stars4.5/5 (2)
- How to ADHD: The Ultimate Guide and Strategies for Productivity and Well-BeingFrom EverandHow to ADHD: The Ultimate Guide and Strategies for Productivity and Well-BeingRating: 1 out of 5 stars1/5 (2)
- Critical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsFrom EverandCritical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsRating: 4.5 out of 5 stars4.5/5 (39)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (254)
- The Marshmallow Test: Mastering Self-ControlFrom EverandThe Marshmallow Test: Mastering Self-ControlRating: 4.5 out of 5 stars4.5/5 (60)
- Troubled: A Memoir of Foster Care, Family, and Social ClassFrom EverandTroubled: A Memoir of Foster Care, Family, and Social ClassRating: 4.5 out of 5 stars4.5/5 (27)
- Summary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisFrom EverandSummary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisRating: 5 out of 5 stars5/5 (8)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (328)
- Summary: $100M Offers: How to Make Offers So Good People Feel Stupid Saying No: by Alex Hormozi: Key Takeaways, Summary & AnalysisFrom EverandSummary: $100M Offers: How to Make Offers So Good People Feel Stupid Saying No: by Alex Hormozi: Key Takeaways, Summary & AnalysisRating: 3.5 out of 5 stars3.5/5 (17)