You might also like
- Advanced Anabolic WorkshopDocument135 pagesAdvanced Anabolic WorkshopVipul89% (9)
- Sample ChapterDocument48 pagesSample ChapterRicardo Jose Soto FontalvoNo ratings yet
- KDIGO 2022 Diabetes Management in CKD Guideline Top 10 Takeaways For CliniciansDocument1 pageKDIGO 2022 Diabetes Management in CKD Guideline Top 10 Takeaways For Cliniciansmanuel nampulaNo ratings yet
- Adults Parenteral Dilution Manual: Yousef AlomiDocument55 pagesAdults Parenteral Dilution Manual: Yousef AlomiAmeng GosimNo ratings yet
- Ratio and Proportion Dosage Calculations 2nd Edition Giangrasso Solutions ManualDocument7 pagesRatio and Proportion Dosage Calculations 2nd Edition Giangrasso Solutions Manualdavidphillipsmcyaqbeogf100% (33)
- Dementia TreatmentDocument76 pagesDementia TreatmentAxel Robinson HerreraNo ratings yet
- Dementia TreatmentDocument76 pagesDementia TreatmentAxel Robinson HerreraNo ratings yet
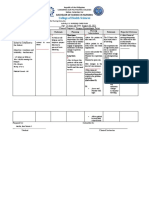
- College of Health Sciences: Bachelor of Science in NursingDocument2 pagesCollege of Health Sciences: Bachelor of Science in NursingLib Kyron MendozaNo ratings yet
- Pi Is 1059131198800678Document7 pagesPi Is 1059131198800678Maghfirani Faroh. FNo ratings yet
- Tutorial Pharmacy Calculation 1Document2 pagesTutorial Pharmacy Calculation 1Siti Nor Dalilawati Binti Syahrin PCNo ratings yet
- Rheumatoid Arthritis Drug Treatment For Rheumatoid ArthritisDocument29 pagesRheumatoid Arthritis Drug Treatment For Rheumatoid ArthritisSundas EjazNo ratings yet
- Donepezil Galantamine Rivastigmine and Memantine For The Treatment of Alzheimers Disease PDF 82600254699973Document76 pagesDonepezil Galantamine Rivastigmine and Memantine For The Treatment of Alzheimers Disease PDF 82600254699973Vanessa HernandezNo ratings yet
- New Rheumatoid Arthritis Management GuidelinesDocument7 pagesNew Rheumatoid Arthritis Management Guidelinesrainmaker77771121No ratings yet
- Practice BrochureDocument12 pagesPractice BrochureMzee321No ratings yet
- Clinical Pharmacokinetics Equations and Calculations IIDocument7 pagesClinical Pharmacokinetics Equations and Calculations IILama SaudNo ratings yet
- HTN Treatment AlgorithmDocument1 pageHTN Treatment AlgorithmKati GrissomNo ratings yet
- Cost Management LectureDocument22 pagesCost Management Lecturespd3ictproNo ratings yet
- Uncomplicated and Complicated Case Management ChartsDocument2 pagesUncomplicated and Complicated Case Management ChartsHudaNo ratings yet
- EDC CE UTD Changes Decisions Improves Care IG WEB1Document1 pageEDC CE UTD Changes Decisions Improves Care IG WEB1lakshminivas PingaliNo ratings yet
- Atogepant For The Prevention of Episodic Migraine in AdultsDocument10 pagesAtogepant For The Prevention of Episodic Migraine in AdultsLorena FNNo ratings yet
- Medication MathDocument48 pagesMedication MathAlice Choi100% (1)
- Vascular Endothelial Growth Factor Receptors (VEGFR) As Target in Breast Cancer Treatment: Current Status in Preclinical and Clinical Studies and Future DirectionsDocument30 pagesVascular Endothelial Growth Factor Receptors (VEGFR) As Target in Breast Cancer Treatment: Current Status in Preclinical and Clinical Studies and Future Directionsmohammad malekanNo ratings yet
- Ratio and Proportion Dosage Calculations 2Nd Edition Giangrasso Solutions Manual Full Chapter PDFDocument17 pagesRatio and Proportion Dosage Calculations 2Nd Edition Giangrasso Solutions Manual Full Chapter PDFdecagrambarrymfh100% (8)
- Whatevidencefor RCTJournalof Diabetes 2009173Document3 pagesWhatevidencefor RCTJournalof Diabetes 2009173api-26007957No ratings yet
- Drug Calclation PLPDocument4 pagesDrug Calclation PLPDarren RobertoNo ratings yet
- Temporary Abdominal Closure: Positive ResultsDocument8 pagesTemporary Abdominal Closure: Positive ResultsCarlos HernándezNo ratings yet
- Drugs StudyDocument1 pageDrugs StudyPrecious UncianoNo ratings yet
- TPT IDAI JAYA 31JAN2021 Nastiti Copy Untuk PesertaDocument39 pagesTPT IDAI JAYA 31JAN2021 Nastiti Copy Untuk PesertaPutri CempakaNo ratings yet
- BC - Jurisprudence - FAQDocument7 pagesBC - Jurisprudence - FAQsanjayNo ratings yet
- Why Heterogeneous Treatment Effects?Document6 pagesWhy Heterogeneous Treatment Effects?Hafiz Saddique MalikNo ratings yet
- HTTPSWWW - Cdc.govvaccinesschedulesdownloadschild0 18yrs Child Combined Schedule PDFDocument12 pagesHTTPSWWW - Cdc.govvaccinesschedulesdownloadschild0 18yrs Child Combined Schedule PDFKhang NgôNo ratings yet
- Scipharm 89 00008Document13 pagesScipharm 89 00008mtmpivvsNo ratings yet
- Electronic Dispensing Handbook - Digital - WEB - S-1589995676Document38 pagesElectronic Dispensing Handbook - Digital - WEB - S-1589995676tony.olay12No ratings yet
- Chapter 5 P: Harmaceutical Care ConceptDocument31 pagesChapter 5 P: Harmaceutical Care ConceptPrashanth RajuNo ratings yet
- Drug Study BipolarDocument13 pagesDrug Study BipolarrahimsyusophNo ratings yet
- Usp36-Nf31 01 216Document12 pagesUsp36-Nf31 01 216AkshayKumarSinghNo ratings yet
- A Review of Bempedoic Acid - A New Drug For Old ProblemDocument6 pagesA Review of Bempedoic Acid - A New Drug For Old ProblemVõ Ngọc Bích VânNo ratings yet
- Pharma Lesson 4Document2 pagesPharma Lesson 4BabyJane GRomeroNo ratings yet
- Diabetes Obesity Metabolism - 2018 - Viljoen - Evaluation of The Long Term Cost Effectiveness of Once Weekly SemaglutideDocument11 pagesDiabetes Obesity Metabolism - 2018 - Viljoen - Evaluation of The Long Term Cost Effectiveness of Once Weekly SemaglutideGonzalo MoragaNo ratings yet
- The Nutrition Consultant in Private Practice 10Document4 pagesThe Nutrition Consultant in Private Practice 10Number MathematicianNo ratings yet
- ISH Hypertension 2020Document6 pagesISH Hypertension 2020drguillermomoNo ratings yet
- Common Verbs For Medical TreatmentDocument2 pagesCommon Verbs For Medical TreatmentMaría CNo ratings yet
- A Study About The Consumer Satisfaction of Ayurvedic Medicines With Special Reference To Cherur Area.Document2 pagesA Study About The Consumer Satisfaction of Ayurvedic Medicines With Special Reference To Cherur Area.PP AshifNo ratings yet
- Pharmacologic Therapy For Type 2 Diabetes: Synopsis of The 2017 American Diabetes Association Standards of Medical Care in DiabetesDocument8 pagesPharmacologic Therapy For Type 2 Diabetes: Synopsis of The 2017 American Diabetes Association Standards of Medical Care in DiabetesSharan KaurNo ratings yet
- Efficacy Corticosteroid On GBSDocument11 pagesEfficacy Corticosteroid On GBSRestu TriwulandaniNo ratings yet
- Adjuvant Laser Meridian Massage in Men With Opioid.72Document5 pagesAdjuvant Laser Meridian Massage in Men With Opioid.72Helena GaribottiNo ratings yet
- Adimea™: Accurate Dialysis Measurement Users GuideDocument2 pagesAdimea™: Accurate Dialysis Measurement Users GuideVia AngelinaNo ratings yet
- CTG Wall ChartDocument1 pageCTG Wall ChartMariaNo ratings yet
- Effect of Semaglutide and Liraglutide in Individuals With Obesity or Overweight Without Diabetes-A Systematic ReviewDocument14 pagesEffect of Semaglutide and Liraglutide in Individuals With Obesity or Overweight Without Diabetes-A Systematic ReviewNewtonRibeiroNo ratings yet
- A Review of The New GLP-1 Receptor Agonist/basal Insulin Fixed-Ratio Combination ProductsDocument11 pagesA Review of The New GLP-1 Receptor Agonist/basal Insulin Fixed-Ratio Combination Productsarief hakikiNo ratings yet
- Hypertension Ideal Care Plan - 2018Document2 pagesHypertension Ideal Care Plan - 2018DanNo ratings yet
- Diabetic Foot Self-Care PractiDocument9 pagesDiabetic Foot Self-Care PractiTiaraNo ratings yet
- Pil 3971Document2 pagesPil 3971Rizqi Dinni FauziaNo ratings yet
- Dmso 202024 Dipeptidyl Peptidase 4 Inhibitors As Add On Therapy To Insul 2Document14 pagesDmso 202024 Dipeptidyl Peptidase 4 Inhibitors As Add On Therapy To Insul 2Miss AmyNo ratings yet
- Synovial Fluid AnalysisDocument6 pagesSynovial Fluid AnalysisFaryalBalochNo ratings yet
- MeningitisDocument11 pagesMeningitisallymyly88No ratings yet
- Journal Club Presentation: DR Waleed AhmadDocument30 pagesJournal Club Presentation: DR Waleed Ahmadkaram aliNo ratings yet
- Prof Ketut Suastika - Diab Manag DEEP Padang 18 Agus 2019Document24 pagesProf Ketut Suastika - Diab Manag DEEP Padang 18 Agus 2019Mita SanryaniNo ratings yet
- Topic 12. Multiple DosesDocument25 pagesTopic 12. Multiple DosesjoseNo ratings yet
- Numeracy and Clinical Calculations for Nurses, second editionFrom EverandNumeracy and Clinical Calculations for Nurses, second editionRating: 1 out of 5 stars1/5 (1)
- Zonio V AcesDocument9 pagesZonio V AceskdchengNo ratings yet
- Insulin Resistance PDFDocument275 pagesInsulin Resistance PDFuzzal ahmedNo ratings yet
- Obesity 1. Basic Science of ObesityDocument10 pagesObesity 1. Basic Science of ObesitygraceNo ratings yet
- Optical Based Non Invasive Glucometer With IoTDocument3 pagesOptical Based Non Invasive Glucometer With IoTSuwetha I GNo ratings yet
- Lecture 2 Diabetes Mellitus TherapyDocument155 pagesLecture 2 Diabetes Mellitus Therapyaleen qawareet100% (1)
- SHPT+PHASE+1 0+pdfDocument12 pagesSHPT+PHASE+1 0+pdfWilliam Stoller100% (1)
- Drugs For Diabetes MellitusDocument3 pagesDrugs For Diabetes MellitusGerardLum100% (1)
- By: Maria Cristina Pamintuan, RMT, MPHDocument74 pagesBy: Maria Cristina Pamintuan, RMT, MPHSanly Duran BambaNo ratings yet
- Buildup of Fatty Plaque in The Arteries, Is The MostDocument7 pagesBuildup of Fatty Plaque in The Arteries, Is The MostCherry Bobier100% (1)
- Diabetes and HerbsDocument132 pagesDiabetes and HerbsAjmal KhanNo ratings yet
- Beta-Cell-Mimetic Designer Cells Provide Closed-Loop Glycemic ControlDocument7 pagesBeta-Cell-Mimetic Designer Cells Provide Closed-Loop Glycemic ControlNando93No ratings yet
- Recombinant DNA TechnologyDocument25 pagesRecombinant DNA Technologymithramithun001No ratings yet
- Vol. 1 Isu. 1Document15 pagesVol. 1 Isu. 1Abdiaziz Mo HagiNo ratings yet
- Fructose-1,6-Bisphosphatase Inhibitors A Review 2017Document33 pagesFructose-1,6-Bisphosphatase Inhibitors A Review 2017alejandra vazquez vazquezNo ratings yet
- Uap Handout 003 Labor Juris 2019 2020Document103 pagesUap Handout 003 Labor Juris 2019 2020Xaba RahNo ratings yet
- The Pathogenesis and Pathophysiology of Type 1 and Type 2 Diabetes MellitusDocument13 pagesThe Pathogenesis and Pathophysiology of Type 1 and Type 2 Diabetes MellitusKimberlyn CustodioNo ratings yet
- TKGS Sec 4 Prelim 2020 Answer Scheme (P1 P2 P3) (Sharing)Document7 pagesTKGS Sec 4 Prelim 2020 Answer Scheme (P1 P2 P3) (Sharing)Anshul BhangaleNo ratings yet
- Endo NclexDocument17 pagesEndo Nclexal-obinay shereenNo ratings yet
- Homeostasis and The Regulation of Blood GlucoseDocument7 pagesHomeostasis and The Regulation of Blood GlucoseElgin SammonsNo ratings yet
- Minimal Model: Perspective From 2005: ResearchDocument9 pagesMinimal Model: Perspective From 2005: ResearchEddy CorNo ratings yet
- PMFIAS CA 2022-06-12 AgricultureDocument73 pagesPMFIAS CA 2022-06-12 Agriculturesiddharth bhatiNo ratings yet
- 1000 - 1500 AbstractBook - BookOfAbstractsDocument500 pages1000 - 1500 AbstractBook - BookOfAbstractsHasan Ibrahim KozanNo ratings yet
- Hormones and The Coordinating System of AnimalsDocument48 pagesHormones and The Coordinating System of AnimalsElaine MontealtoNo ratings yet
- Type 2 DiabetesDocument543 pagesType 2 DiabetesSofija VukadinovićNo ratings yet
- Guduchi A Potential Drug in AyurvedaDocument8 pagesGuduchi A Potential Drug in AyurvedaSunnyNo ratings yet
- DiabetesDocument15 pagesDiabetesSalman KhawarNo ratings yet
- Eur Heart J 2013 Eurheartj - Eht108Document63 pagesEur Heart J 2013 Eurheartj - Eht108Liman SetiawanNo ratings yet
- Ada 2015 Summary PDFDocument41 pagesAda 2015 Summary PDFcuambyahooNo ratings yet
- Hba1C HPLC Assay: Package InsertDocument9 pagesHba1C HPLC Assay: Package InsertKery B. SantsNo ratings yet