You might also like
- Carcinoembryonic Antigen As A Marker For Colorecta PDFDocument8 pagesCarcinoembryonic Antigen As A Marker For Colorecta PDFYuliana PratiwiNo ratings yet
- CEA StageDocument14 pagesCEA StageSugeng JitowiyonoNo ratings yet
- A Review of The Role of Carcinoembryonic Antigen IDocument12 pagesA Review of The Role of Carcinoembryonic Antigen IMarcellia AngelinaNo ratings yet
- Carcinoembryonic Antigen: Characterization and Clinical ApplicationsDocument31 pagesCarcinoembryonic Antigen: Characterization and Clinical ApplicationsSugeng JitowiyonoNo ratings yet
- Creatine Phosphokinase Levels in Oral Cancer Patients: Issn 0974-3618 (Print) 0974-360X (Online)Document4 pagesCreatine Phosphokinase Levels in Oral Cancer Patients: Issn 0974-3618 (Print) 0974-360X (Online)Deepak KumarNo ratings yet
- Articulo 2Document11 pagesArticulo 2Andrea NeriaNo ratings yet
- Pharmacological Research: SciencedirectDocument10 pagesPharmacological Research: SciencedirectKeyla MaydeeNo ratings yet
- 2023 Article 529Document22 pages2023 Article 529amirNo ratings yet
- Elevated Level of Serum Carcinoembryonic Antigen (CEA) and Search For A Malignancy: A Case ReportDocument4 pagesElevated Level of Serum Carcinoembryonic Antigen (CEA) and Search For A Malignancy: A Case ReportDhen Mas PrimanaNo ratings yet
- 1 s2.0 S1743919115013953 MainDocument11 pages1 s2.0 S1743919115013953 MainMita AdrianiNo ratings yet
- CA A Cancer J Clinicians - March April 1988 - Virji - Tumor Markers in Cancer Diagnosis and PrognosisDocument23 pagesCA A Cancer J Clinicians - March April 1988 - Virji - Tumor Markers in Cancer Diagnosis and PrognosisIssahaku AbdallahNo ratings yet
- NLR & CEA As Prognostic FactorDocument8 pagesNLR & CEA As Prognostic FactorEly Sakti SihotangNo ratings yet
- Pharmacology Res Perspec - 2021 - Das - CCN5 Activation by Free or Encapsulated EGCG Is Required To RenderDocument14 pagesPharmacology Res Perspec - 2021 - Das - CCN5 Activation by Free or Encapsulated EGCG Is Required To RenderAaron CiudadNo ratings yet
- Biomarkers For The Diagnosis of Cholangiocarcinoma A Systematic Review 2018Document10 pagesBiomarkers For The Diagnosis of Cholangiocarcinoma A Systematic Review 2018Anna MariaNo ratings yet
- DNA Aptamer Evolved by Cell-SELEX For Recognition ofDocument10 pagesDNA Aptamer Evolved by Cell-SELEX For Recognition ofFernanda LDNo ratings yet
- Zeng 2013Document7 pagesZeng 2013angela_karenina_1No ratings yet
- Fonc 11 664848Document10 pagesFonc 11 664848m8f5mwpzwyNo ratings yet
- Grady Reading1Document15 pagesGrady Reading1hh1790No ratings yet
- Cybulska 2019Document8 pagesCybulska 2019ZULMA MADELINE LIBNY GUTARRA TICANo ratings yet
- PL 00011733Document9 pagesPL 00011733Monica CabaNo ratings yet
- Liao 2014Document13 pagesLiao 2014Jenivia LulileloNo ratings yet
- CA A Cancer J Clinicians - March April 1988 - Virji - Tumor Markers in Cancer Diagnosis and PrognosisDocument23 pagesCA A Cancer J Clinicians - March April 1988 - Virji - Tumor Markers in Cancer Diagnosis and Prognosistem gastonNo ratings yet
- Artcle 2 PDFDocument11 pagesArtcle 2 PDFAnirban PaulNo ratings yet
- Asima-Bisha 2012Document8 pagesAsima-Bisha 2012Bisha UzirNo ratings yet
- DLK1 As A Potential Target Against Cancer Stem/Progenitor Cells of Hepatocellular CarcinomaDocument10 pagesDLK1 As A Potential Target Against Cancer Stem/Progenitor Cells of Hepatocellular CarcinomaHadrien DemagnyNo ratings yet
- Ijcep 0011785Document6 pagesIjcep 0011785TanveerNo ratings yet
- 2005 - Xin - CCSP2 Novel CandidateDocument8 pages2005 - Xin - CCSP2 Novel CandidateedmaryvictoriaNo ratings yet
- Asia-Pac J CLNCL Oncology - 2023 - Bonazzi - C Reactive Protein Is A Prognostic Biomarker in Pancreatic DuctalDocument10 pagesAsia-Pac J CLNCL Oncology - 2023 - Bonazzi - C Reactive Protein Is A Prognostic Biomarker in Pancreatic DuctalHamsa veniNo ratings yet
- Cancer de MamaDocument12 pagesCancer de MamaDavid Galiano LatorreNo ratings yet
- Thno 54961r2 3Document45 pagesThno 54961r2 3Eduardo JuarezNo ratings yet
- Cancers 13 02067Document15 pagesCancers 13 02067Flaviu Ionuț FaurNo ratings yet
- s10120 016 0652 YnvidotknvtgDocument8 pagess10120 016 0652 YnvidotknvtgJavi Jimenez VelascoNo ratings yet
- CCN1 Sensitizes Esophageal Cancer Cells To TRAIL Me - 2017 - Experimental Cell RDocument7 pagesCCN1 Sensitizes Esophageal Cancer Cells To TRAIL Me - 2017 - Experimental Cell RFlorin AchimNo ratings yet
- Lectin Diagnostic CancerDocument22 pagesLectin Diagnostic CancerChrysthian Didier BernardesNo ratings yet
- Tumor MarkerDocument5 pagesTumor MarkerIndah95No ratings yet
- Cancers: Oncomine™ Comprehensive Assay v3 vs. Oncomine™ Comprehensive Assay PlusDocument19 pagesCancers: Oncomine™ Comprehensive Assay v3 vs. Oncomine™ Comprehensive Assay PlusquarkstarscribdNo ratings yet
- Cytogenetic Profile Predicts Prognosis of Patients With Clear Cell Renal Cell CarcinomaDocument8 pagesCytogenetic Profile Predicts Prognosis of Patients With Clear Cell Renal Cell CarcinomaRivan 21No ratings yet
- Circulating Endothelial Cells and Other Angiogenesis Factors in Pancreatic Carcinoma Patients Receiving Gemcitabine ChemotherapyDocument10 pagesCirculating Endothelial Cells and Other Angiogenesis Factors in Pancreatic Carcinoma Patients Receiving Gemcitabine ChemotherapyftwNo ratings yet
- Intra-Lesional Injection of The Novel PKC Activator EBC-46 Rapidly Ablates Tumors in Mouse ModelsDocument12 pagesIntra-Lesional Injection of The Novel PKC Activator EBC-46 Rapidly Ablates Tumors in Mouse ModelscarlammartinsNo ratings yet
- Aquaporin 1 Is A Prognostic Marker and Inhibits Tumour Progression Through Downregulation of Snail Expression in Intrahepatic CholangiocarcinomaDocument8 pagesAquaporin 1 Is A Prognostic Marker and Inhibits Tumour Progression Through Downregulation of Snail Expression in Intrahepatic CholangiocarcinomaΡαφαήλ ΠαπανάγνοςNo ratings yet
- Acta31 01-04 26 TDocument10 pagesActa31 01-04 26 TTanveerNo ratings yet
- Barsanti-Innes The Oncologist - 2016Document8 pagesBarsanti-Innes The Oncologist - 2016Liz BethNo ratings yet
- OncolyticDocument14 pagesOncolytichasna muhadzibNo ratings yet
- Stadializare HCCDocument12 pagesStadializare HCCIanosi BogdanNo ratings yet
- Poliposis Adenomatosa FamiliarDocument14 pagesPoliposis Adenomatosa FamiliarRicardo Uzcategui ArreguiNo ratings yet
- Jco 19 00337Document13 pagesJco 19 00337alberto cabelloNo ratings yet
- Squamous Cellular Carcinoma Antigen Serum Determination As A Biomarker of Barrett Esophagus and Esophageal CancerDocument6 pagesSquamous Cellular Carcinoma Antigen Serum Determination As A Biomarker of Barrett Esophagus and Esophageal CancervictorNo ratings yet
- Evaluation of An Inflammation-Based Prognostic Score in Patients With Inoperable Gastro-Oesophageal CancerDocument5 pagesEvaluation of An Inflammation-Based Prognostic Score in Patients With Inoperable Gastro-Oesophageal CancerdianaNo ratings yet
- Cancer de PancreasDocument12 pagesCancer de PancreasRuben RoaNo ratings yet
- Carcinoma of Unknown Primary Origin: Gauri R. VaradhacharyDocument7 pagesCarcinoma of Unknown Primary Origin: Gauri R. VaradhacharyHeather PorterNo ratings yet
- Multi-Targeted Therapy Resistance Via Drug - Induced Secretome FucosylationDocument42 pagesMulti-Targeted Therapy Resistance Via Drug - Induced Secretome Fucosylationaditya subchanNo ratings yet
- Articulo de HistologiaDocument6 pagesArticulo de HistologiaalexbowwNo ratings yet
- Molecular Profiling in Muscle-Invasive Bladder Cancer: More Than The Sum of Its PartsDocument11 pagesMolecular Profiling in Muscle-Invasive Bladder Cancer: More Than The Sum of Its PartsJoel ChávezdrumsNo ratings yet
- Establishing A Human Renal Cell Carcinoma Tumorgraft Platform For Preclinical Drug TestingDocument12 pagesEstablishing A Human Renal Cell Carcinoma Tumorgraft Platform For Preclinical Drug TestingArvin ZakerNo ratings yet
- 1 - Colorectal CancerDocument11 pages1 - Colorectal CancerNatnicha foongfaNo ratings yet
- 1 s2.0 S2590156723000695 MainDocument16 pages1 s2.0 S2590156723000695 Mainmonu kashyapNo ratings yet
- JANG - Extracellular Vesicle (EV) - Polyphenol Nanoaggregates For microRNA-based Cancer DiagnosisDocument10 pagesJANG - Extracellular Vesicle (EV) - Polyphenol Nanoaggregates For microRNA-based Cancer DiagnosisenaNo ratings yet
- The Examiner of Alternative MedicineDocument4 pagesThe Examiner of Alternative MedicineLee Ming HinNo ratings yet
- 03-Unravelling The Proteomic Landscape of Extracellular Vesicles in Prostate Cancer by Density-BaDocument25 pages03-Unravelling The Proteomic Landscape of Extracellular Vesicles in Prostate Cancer by Density-BaInggita Adinda PutriNo ratings yet
- Fast Facts: Cholangiocarcinoma: Diagnostic and therapeutic advances are improving outcomesFrom EverandFast Facts: Cholangiocarcinoma: Diagnostic and therapeutic advances are improving outcomesNo ratings yet
- STATUS KESEHATANDocument1 pageSTATUS KESEHATANSugeng JitowiyonoNo ratings yet
- Patterns of Adoption of RoboticDocument21 pagesPatterns of Adoption of RoboticSugeng JitowiyonoNo ratings yet
- Bibliometric Analysis of Journals, Authors, and Topics Related To Halal Tourism Listed in The Database Scopus by Indonesian AuthorsDocument16 pagesBibliometric Analysis of Journals, Authors, and Topics Related To Halal Tourism Listed in The Database Scopus by Indonesian AuthorsSugeng JitowiyonoNo ratings yet
- Validitas Isi: Tahap Awal Pengembangan KuesionerDocument11 pagesValiditas Isi: Tahap Awal Pengembangan KuesionerSuryanti ChenNo ratings yet
- A Scopus Based Bibliometric Evaluation of Saudi Medical JournalDocument11 pagesA Scopus Based Bibliometric Evaluation of Saudi Medical JournalSugeng JitowiyonoNo ratings yet
- 2014 Development of A Tool For DefiningDocument13 pages2014 Development of A Tool For DefiningSugeng JitowiyonoNo ratings yet
- Gender Inequality in Health Among Elderly People in A Combined Framework of Socioeconomic Position Family Characteristics and Social SupportDocument23 pagesGender Inequality in Health Among Elderly People in A Combined Framework of Socioeconomic Position Family Characteristics and Social SupportSugeng JitowiyonoNo ratings yet
- 1 s2.0 S0167494316300498 MainDocument7 pages1 s2.0 S0167494316300498 MainSugeng JitowiyonoNo ratings yet
- 1 s2.0 S0167494319301530 MainDocument9 pages1 s2.0 S0167494319301530 MainSugeng JitowiyonoNo ratings yet
- Abbreviated Comprehensive Geriatric Assessment (aCGA)Document6 pagesAbbreviated Comprehensive Geriatric Assessment (aCGA)Sugeng JitowiyonoNo ratings yet
- Developing A Comprehensive Cancer Specific GeriatricDocument4 pagesDeveloping A Comprehensive Cancer Specific GeriatricSugeng JitowiyonoNo ratings yet
- Multifactorial Screening For Fall Risk In.5Document10 pagesMultifactorial Screening For Fall Risk In.5Sugeng JitowiyonoNo ratings yet
- Rapid Geriatric AssessmentDocument5 pagesRapid Geriatric AssessmentSugeng JitowiyonoNo ratings yet
- Comprehensive Geriatric Assessment in The Older AdultDocument10 pagesComprehensive Geriatric Assessment in The Older AdultSugeng JitowiyonoNo ratings yet
- Brief Assessments and Screening ForDocument13 pagesBrief Assessments and Screening ForSugeng JitowiyonoNo ratings yet
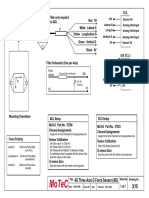
- Filter and wiring schematic for 3-axis ADL G-force sensorDocument1 pageFilter and wiring schematic for 3-axis ADL G-force sensorJuan Ramón Pérez LorenzoNo ratings yet
- Tapping Volcanic Energy for Human UseDocument9 pagesTapping Volcanic Energy for Human UseThartson Oliveros MagdadaroNo ratings yet
- Ecosystem Components and InteractionsDocument31 pagesEcosystem Components and InteractionsBirraa TajuNo ratings yet
- Project: M/S Cae-Gondia at Nagpur Cable Schedule For Proposed ProjectDocument26 pagesProject: M/S Cae-Gondia at Nagpur Cable Schedule For Proposed ProjectMurali MohanNo ratings yet
- Innogy Invitation For Seminar PCODocument6 pagesInnogy Invitation For Seminar PCOTivorshio MacabodbodNo ratings yet
- Recommended Abma & Asme Boiler Water Limits Drum Operating Pressure (Psig) SteamDocument9 pagesRecommended Abma & Asme Boiler Water Limits Drum Operating Pressure (Psig) Steammaoc4vnNo ratings yet
- Low Noise Pseudomorphic HEMT Technical DataDocument4 pagesLow Noise Pseudomorphic HEMT Technical Datahendpraz88No ratings yet
- Help to Buy ISA GuideDocument4 pagesHelp to Buy ISA GuidefsdesdsNo ratings yet
- 4-Ingredient Vegan Easy Brownies - Minimalist Baker RecipesDocument2 pages4-Ingredient Vegan Easy Brownies - Minimalist Baker RecipespeteNo ratings yet
- THE LIVING MATRIX: A MODEL FOR THE PRIMARTY RESPIRATORY MECHANISMDocument69 pagesTHE LIVING MATRIX: A MODEL FOR THE PRIMARTY RESPIRATORY MECHANISMRukaphuongNo ratings yet
- Bonanza A36 ChecklistDocument10 pagesBonanza A36 Checklistalbucur100% (4)
- Edc Power Plant FacilitiesDocument32 pagesEdc Power Plant FacilitiesMichael TayactacNo ratings yet
- Sarah Fahy CV College PDFDocument4 pagesSarah Fahy CV College PDFapi-487352339No ratings yet
- The Electrooculogram (EOG)Document34 pagesThe Electrooculogram (EOG)Prasidha PrabhuNo ratings yet
- Silver Rain Svetlana Perevalova PDFDocument9 pagesSilver Rain Svetlana Perevalova PDFAndrea Koumarian100% (1)
- Blood Bank Case Study 5bDocument2 pagesBlood Bank Case Study 5bbalqis jaberNo ratings yet
- 2 Way 3 Way Piping DiagramDocument1 page2 Way 3 Way Piping DiagrammarrukhjNo ratings yet
- NFPA 97 - 2003 Standard Glossary of Terms Relating To Chimneys, Vents, and Heat-Producing AppliancesDocument34 pagesNFPA 97 - 2003 Standard Glossary of Terms Relating To Chimneys, Vents, and Heat-Producing Appliancesonepunchman yaoNo ratings yet
- Moisture Sorption Isotherms Characteristics of Food ProductsDocument10 pagesMoisture Sorption Isotherms Characteristics of Food ProductsMustapha Bello50% (2)
- PEDH ReviewerDocument10 pagesPEDH ReviewerMaki Orejola de LeonNo ratings yet
- Animals Pets Board GameDocument1 pageAnimals Pets Board GameOlga ZasNo ratings yet
- Flame Amplifier HoneywellDocument8 pagesFlame Amplifier Honeywellgavo vargoNo ratings yet
- Basic Principles of Growth DevelopmentDocument19 pagesBasic Principles of Growth DevelopmentMikz Chua100% (1)
- (PP 67-14) Quantifying Cracks in Asphalt Pavement Surfaces From Collected Images Utilizing Automated MethodsDocument7 pages(PP 67-14) Quantifying Cracks in Asphalt Pavement Surfaces From Collected Images Utilizing Automated MethodsAveNo ratings yet
- Volcanic Eruption Types and ProcessDocument18 pagesVolcanic Eruption Types and ProcessRosemarie Joy TanioNo ratings yet
- Jurnal Dermatitis AtopikDocument20 pagesJurnal Dermatitis AtopikchintyaNo ratings yet
- Riel Comun Fstguide2Document2 pagesRiel Comun Fstguide2Rosita TejedaNo ratings yet
- Hyperfunctional Voice DisordersDocument11 pagesHyperfunctional Voice DisordersJam PNo ratings yet
- Basic Science JSS 1 2NDDocument29 pagesBasic Science JSS 1 2NDAdeoye Olufunke100% (2)
- Wrap Book A4Document27 pagesWrap Book A4doscribe100% (1)