You might also like
- Critical Care for Potential Liver Transplant CandidatesFrom EverandCritical Care for Potential Liver Transplant CandidatesDmitri BezinoverNo ratings yet
- The Fontan Procedure Contemporary Techniques Have Improved Long-Term OutcomesDocument8 pagesThe Fontan Procedure Contemporary Techniques Have Improved Long-Term OutcomesEko SiswantoNo ratings yet
- Thoracic Endoscopy: Advances in Interventional PulmonologyFrom EverandThoracic Endoscopy: Advances in Interventional PulmonologyMichael J. SimoffNo ratings yet
- Manejo FontanDocument11 pagesManejo FontanAngélica ContrerasNo ratings yet
- Annual Update in Intensive Care and Emergency Medicine 2020From EverandAnnual Update in Intensive Care and Emergency Medicine 2020No ratings yet
- Kverneland 2018Document13 pagesKverneland 2018Eko SiswantoNo ratings yet
- Perioperative Two-Dimensional Transesophageal Echocardiography: A Practical HandbookFrom EverandPerioperative Two-Dimensional Transesophageal Echocardiography: A Practical HandbookNo ratings yet
- 朱家权氯沙坦猪模型Document10 pages朱家权氯沙坦猪模型shentujin1997No ratings yet
- Pi Is 0003497521008249Document8 pagesPi Is 0003497521008249Santoso 9JimmyNo ratings yet
- The Fontan Circulation Contin EducDocument5 pagesThe Fontan Circulation Contin EducAishu BNo ratings yet
- J Neucom 2012 03 034Document8 pagesJ Neucom 2012 03 034masanta11No ratings yet
- Patent Ductus Arteriosus Stenting For Palliation of Severe Pulmonary Arterial Hypertension in ChildhoodDocument5 pagesPatent Ductus Arteriosus Stenting For Palliation of Severe Pulmonary Arterial Hypertension in ChildhoodEffendi TanNo ratings yet
- A 40 YearsDocument9 pagesA 40 YearsDra Mariana Huerta CampaNo ratings yet
- Fontan Operation: DR Hussain BuxDocument62 pagesFontan Operation: DR Hussain BuxMujeeb Ur RehmanNo ratings yet
- Kim2012Document5 pagesKim2012Stefanie MelisaNo ratings yet
- HM3 in FontonDocument2 pagesHM3 in FontonselvakumarNo ratings yet
- Article 8Document4 pagesArticle 8Kamal SaleemNo ratings yet
- Tam 1999Document6 pagesTam 1999Eko SiswantoNo ratings yet
- Transhepatic Access: Alternative Approach For Right Heart Catheterization and Pulmonary AngiographyDocument3 pagesTranshepatic Access: Alternative Approach For Right Heart Catheterization and Pulmonary AngiographyDavids MarinNo ratings yet
- Early and Intermediate-Term Results of The Extracardiac Conduit Total Cavopulmonary Connection For Functional Single-Ventricle HeartsDocument7 pagesEarly and Intermediate-Term Results of The Extracardiac Conduit Total Cavopulmonary Connection For Functional Single-Ventricle HeartstedejoNo ratings yet
- The Fontan Procedure: Anatomy, Complications, and Manifestations of FailureDocument12 pagesThe Fontan Procedure: Anatomy, Complications, and Manifestations of FailureEko SiswantoNo ratings yet
- Anaesthetic Management of Posterior Mediastinal Mass in A Child. Case ReportDocument3 pagesAnaesthetic Management of Posterior Mediastinal Mass in A Child. Case ReporttcsariNo ratings yet
- 40-Year Follow-Up After The 2015Document11 pages40-Year Follow-Up After The 2015rujiraNo ratings yet
- Long-Term Fate of The Truncal ValveDocument15 pagesLong-Term Fate of The Truncal Valvehuynhtruongthinh1998No ratings yet
- FCVM 08 775578Document9 pagesFCVM 08 775578wiyay34652ceoshubcomNo ratings yet
- Cryptogenic Stroke and Patent Foramen Ovale: Review Topic of The WeekDocument8 pagesCryptogenic Stroke and Patent Foramen Ovale: Review Topic of The WeekferrevNo ratings yet
- Accidente Cerebrovascular Criptogénico Yforamen Oval Permea 2018Document9 pagesAccidente Cerebrovascular Criptogénico Yforamen Oval Permea 2018federico saldariniNo ratings yet
- Ventricular Assist Device For Fontan - Who, When and WhyDocument6 pagesVentricular Assist Device For Fontan - Who, When and WhyPatricia Martínez piano flamencoNo ratings yet
- Surgical Treatment of Partial Anomalous Pulmonary Venous Connection To The Superior Vena CavaDocument5 pagesSurgical Treatment of Partial Anomalous Pulmonary Venous Connection To The Superior Vena CavaJose YoveraNo ratings yet
- Ezs 535Document6 pagesEzs 535Eko SiswantoNo ratings yet
- Poterucha 2015Document13 pagesPoterucha 2015Comanescu MirelaNo ratings yet
- Diagnostic AlgorithmDocument7 pagesDiagnostic AlgorithmindahNo ratings yet
- Venous Stent Recovery Migrated To Right Pulmonary Artery: Case Report, Clinical Review and UpdateDocument4 pagesVenous Stent Recovery Migrated To Right Pulmonary Artery: Case Report, Clinical Review and UpdateRomeo GuevaraNo ratings yet
- Percutaneous Transluminal Balloon Valvuloplasty For Pulmonary Valve StenosisDocument7 pagesPercutaneous Transluminal Balloon Valvuloplasty For Pulmonary Valve Stenosisandrew timanta brahmanaNo ratings yet
- Ecocardiografia Monitoreo Hemodinamico en Critico..Document12 pagesEcocardiografia Monitoreo Hemodinamico en Critico..cositaamorNo ratings yet
- 2018 - Article Erdocan 8p.pdf - CopieDocument6 pages2018 - Article Erdocan 8p.pdf - CopieThomas HussonNo ratings yet
- Carotid StentDocument9 pagesCarotid StentCut FadmalaNo ratings yet
- Extracardiac Fontan With Direct Inferior Vena Cava To Main Pulmonary Artery Connection Without Cardiopulmonary BypassDocument4 pagesExtracardiac Fontan With Direct Inferior Vena Cava To Main Pulmonary Artery Connection Without Cardiopulmonary BypassEko SiswantoNo ratings yet
- Early and Late Results of The Modified Fontan Operation For Heterotaxy SyndromeDocument5 pagesEarly and Late Results of The Modified Fontan Operation For Heterotaxy SyndromeJacob Trisusilo SaleanNo ratings yet
- De Neuville 2000Document5 pagesDe Neuville 2000Anonymous WPiPld6npNo ratings yet
- Apm 12 151 PDFDocument4 pagesApm 12 151 PDFFityan Aulia RahmanNo ratings yet
- Bleeding On Dual Antiplatelet Therapy: Real-Life ChallengesDocument9 pagesBleeding On Dual Antiplatelet Therapy: Real-Life ChallengesTri Ari dityaNo ratings yet
- Association of Lymphatic Abnormalities With Early Complications After Fontan OperationDocument9 pagesAssociation of Lymphatic Abnormalities With Early Complications After Fontan OperationCarlos CostaNo ratings yet
- USC Moe FINAL - SV PhysiologyDocument5 pagesUSC Moe FINAL - SV PhysiologyindahNo ratings yet
- 朱家权1Document9 pages朱家权1shentujin1997No ratings yet
- CTEPH and Klippel Trenaunay SyndromeDocument6 pagesCTEPH and Klippel Trenaunay SyndromeAndreiSefNo ratings yet
- 2-Year Outcomes After Transcatheter Mitral Valve ReplacementDocument8 pages2-Year Outcomes After Transcatheter Mitral Valve Replacementphi taiNo ratings yet
- Heinemann 2001Document7 pagesHeinemann 2001Binod KumarNo ratings yet
- Outcome Analysis of Ventriculoperitoneal Shunt Procedures in Hydrocephalus Due To Tubercular Meningitis and Non-Infective CasesDocument6 pagesOutcome Analysis of Ventriculoperitoneal Shunt Procedures in Hydrocephalus Due To Tubercular Meningitis and Non-Infective CasesNurul AzizahNo ratings yet
- Nee TH Ling 2019Document18 pagesNee TH Ling 2019diogofc123No ratings yet
- Chronic Type B "Residual" After Type A: What I Would Do?Document5 pagesChronic Type B "Residual" After Type A: What I Would Do?Essam KhalafNo ratings yet
- Transcatheter Coil Embolotherapy: A Safe and Evective Option For Major Colonic HaemorrhageDocument7 pagesTranscatheter Coil Embolotherapy: A Safe and Evective Option For Major Colonic Haemorrhagemuhammad gagas sasongkoNo ratings yet
- Perioperative Management of AdrenalectomyDocument13 pagesPerioperative Management of AdrenalectomyTJ LapuzNo ratings yet
- Otolaryngology - Head and Neck Surgery: Hemorrhage Following Tonsillectomy and Adenoidectomy in 15,218 PatientsDocument7 pagesOtolaryngology - Head and Neck Surgery: Hemorrhage Following Tonsillectomy and Adenoidectomy in 15,218 PatientsreztrymaulidaNo ratings yet
- 2022 Article 1790Document7 pages2022 Article 1790juajimenez55No ratings yet
- Pi Is 0003497500014818Document7 pagesPi Is 0003497500014818GKNo ratings yet
- Dowling 1990Document5 pagesDowling 1990Gaetano Di GiovanniNo ratings yet
- Bosentan Treatment For Pulmonary Arterial Hypertension Due To Patent Ductus Arteriosus and Down's Syndrome in An InfantDocument2 pagesBosentan Treatment For Pulmonary Arterial Hypertension Due To Patent Ductus Arteriosus and Down's Syndrome in An InfantOctavianus KevinNo ratings yet
- Costello HeartlungmachineDocument10 pagesCostello HeartlungmachineAnand GvphNo ratings yet
- Psychopathological Risks Associated With Adherence To Treatment of Patients With High Blood PressureDocument13 pagesPsychopathological Risks Associated With Adherence To Treatment of Patients With High Blood PressureInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Long-Term Abstinence Following Holotropic Breathwork As Adjunctive Treatment of Substance Use Disorders and Related Psychiatric ComorbidityDocument7 pagesLong-Term Abstinence Following Holotropic Breathwork As Adjunctive Treatment of Substance Use Disorders and Related Psychiatric ComorbiditymghuesoNo ratings yet
- Different Types of AsthmaDocument16 pagesDifferent Types of AsthmaAmira Saidin0% (1)
- Pelod ScoreDocument7 pagesPelod ScoreAgus SarjonoNo ratings yet
- Reduction of Depression and Anxiety by 4 Weeks Hericium Erinaceus IntakeDocument7 pagesReduction of Depression and Anxiety by 4 Weeks Hericium Erinaceus IntakeBob CornellNo ratings yet
- Ocular Hypotony - A Comprehensive ReviewDocument20 pagesOcular Hypotony - A Comprehensive ReviewJavier Infantes MolinaNo ratings yet
- Fluid Volume ExcessDocument2 pagesFluid Volume ExcessRodel Yacas100% (5)
- Parasite CleanseDocument17 pagesParasite CleanseHisExcellencyNo ratings yet
- 046 - 1554 - Ni Kadek Seri Mahayanti - GalleyDocument4 pages046 - 1554 - Ni Kadek Seri Mahayanti - Galleysibon M amrilNo ratings yet
- Jawaharlal Nehru Medical College Belgaum Admission - Fees - Seats - ExamsDocument10 pagesJawaharlal Nehru Medical College Belgaum Admission - Fees - Seats - ExamsRakeshKumar1987No ratings yet
- Cerebro NeonatalDocument8 pagesCerebro NeonatalRodri EspinNo ratings yet
- Continuous Renal Replacement Therapy Education PackDocument18 pagesContinuous Renal Replacement Therapy Education PacktsongtonsgNo ratings yet
- HEALTH ASSESSMENT - BatteryDocument20 pagesHEALTH ASSESSMENT - BatteryJoana Grace Cortez100% (1)
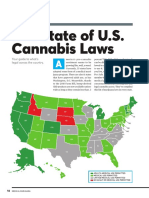
- The State of U.S. Cannabis Laws, AbridgedDocument6 pagesThe State of U.S. Cannabis Laws, AbridgedPaul Marini100% (1)
- N-Acetylcysteine To Combat COVID-19: An Evidence Review - PubMedDocument2 pagesN-Acetylcysteine To Combat COVID-19: An Evidence Review - PubMedDavid ShapiroNo ratings yet
- Wyogyhna A. Quidilla, RNDocument2 pagesWyogyhna A. Quidilla, RNMc DalayapNo ratings yet
- A Model To Predict Short-Term Death or Readmission After Intensive Care Unit DischargeDocument10 pagesA Model To Predict Short-Term Death or Readmission After Intensive Care Unit DischargeInnani Wildania HusnaNo ratings yet
- Ramsay Hunt Syndrome: Infectious DiseasesDocument3 pagesRamsay Hunt Syndrome: Infectious DiseasesAldy BimaNo ratings yet
- TATA Medicare Premier 871b2dee42Document8 pagesTATA Medicare Premier 871b2dee42ramana reddy KotaNo ratings yet
- 05 Digital Vag Exam Revised Feb 06Document2 pages05 Digital Vag Exam Revised Feb 06Musa yohanaNo ratings yet
- XI. Chronic Kidney Disease PDFDocument45 pagesXI. Chronic Kidney Disease PDFnaro ayosNo ratings yet
- Clinical Practice Guidelines On Hepatitis Delta VirusDocument28 pagesClinical Practice Guidelines On Hepatitis Delta VirusRadu IonescuNo ratings yet
- HaiHua CD 9X User ManualDocument13 pagesHaiHua CD 9X User ManualEdson Cordeaca100% (1)
- The KDIGO AKI Guidelines: From 2011-2019Document38 pagesThe KDIGO AKI Guidelines: From 2011-2019Andreas Agung KurniawanNo ratings yet
- BIO PROJECT For Class 12 On Drug AddictionDocument17 pagesBIO PROJECT For Class 12 On Drug Addictiongaurav nehraNo ratings yet
- Namrata Final PaperDocument22 pagesNamrata Final PaperAngel TechNo ratings yet
- Arterial Line and Central LineDocument32 pagesArterial Line and Central LineOrachorn AimarreeratNo ratings yet
- Fractional CO2Document4 pagesFractional CO2Rahul PillaiNo ratings yet
- 2023 ABC of Major Trauma Rescue, Resuscitation With Imaging, andDocument493 pages2023 ABC of Major Trauma Rescue, Resuscitation With Imaging, andVanessa MendozaNo ratings yet
- Acute Renal Failure: John FeehallyDocument107 pagesAcute Renal Failure: John Feehallygede wira mahaditaNo ratings yet
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (404)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 4.5 out of 5 stars4.5/5 (83)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (36)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDFrom EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDRating: 5 out of 5 stars5/5 (4)
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)From EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Rating: 3 out of 5 stars3/5 (1)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- The Twentysomething Treatment: A Revolutionary Remedy for an Uncertain AgeFrom EverandThe Twentysomething Treatment: A Revolutionary Remedy for an Uncertain AgeRating: 4.5 out of 5 stars4.5/5 (2)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 4 out of 5 stars4/5 (5)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeRating: 2 out of 5 stars2/5 (1)
- Manipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesFrom EverandManipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesRating: 4.5 out of 5 stars4.5/5 (1412)
- I Shouldn't Feel This Way: Name What’s Hard, Tame Your Guilt, and Transform Self-Sabotage into Brave ActionFrom EverandI Shouldn't Feel This Way: Name What’s Hard, Tame Your Guilt, and Transform Self-Sabotage into Brave ActionNo ratings yet
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- Critical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsFrom EverandCritical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsRating: 4.5 out of 5 stars4.5/5 (39)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (44)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (170)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (46)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (254)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsFrom EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo ratings yet
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- Self-Care for Autistic People: 100+ Ways to Recharge, De-Stress, and Unmask!From EverandSelf-Care for Autistic People: 100+ Ways to Recharge, De-Stress, and Unmask!Rating: 5 out of 5 stars5/5 (1)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (267)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 4 out of 5 stars4/5 (6)
- Summary: Thinking, Fast and Slow: by Daniel Kahneman: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: Thinking, Fast and Slow: by Daniel Kahneman: Key Takeaways, Summary & Analysis IncludedRating: 4 out of 5 stars4/5 (61)