Professional Documents
Culture Documents
Combine 3 Fitzpatricks Dermatology 9th Edition (PDF - Io)
Uploaded by
IcasiaYuseliOriginal Description:
Original Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Combine 3 Fitzpatricks Dermatology 9th Edition (PDF - Io)
Uploaded by
IcasiaYuseliCopyright:
Available Formats
Fitzpatrick’s
Dermatology
Ninth Edition
EDITORS
SEWON KANG, MD, MPH
MASAYUKI AMAGAI, MD, PhD
ANNA L. BRUCKNER, MD, MSCS
ALEXANDER H. ENK, MD
DAVID J. MARGOLIS, MD, PhD
AMY J. McMICHAEL, MD
JEFFREY S. ORRINGER, MD
VOLUME I
New York Chicago San Francisco Athens London Madrid Mexico City
Milan New Delhi Singapore Sydney Toronto
Kang_DIGM-FM_Vol-I.indd 3 08/12/18 5:31 pm
11
Dermal Connective PART
Tissue Disorders
Chapter 70 :: Anetoderma and Other Atrophic
Disorders of the Skin
:: Catherine Maari & Julie Powell
ANETODERMA suggesting that not only elastolytic overactivity,
but also defective elastic fiber reassembly, may be
involved.6 Immunologic mechanisms may also play a
role, as it can be associated with various systemic con-
AT-A-GLANCE ditions, primarily antiphospholipid antibodies.
■ Circumscribed 1- to 2-cm areas of flaccid skin that
may be elevated, macular, or depressed.
■ Often circumscribed sac-like protrusions. CLINICAL FEATURES
■ Primary or secondary to a preceding dermatosis in
the same location. All types of anetoderma are characterized by a cir-
■ Association with antiphospholipid syndrome. cumscribed loss of normal skin elasticity. The charac-
■ Pathology consists of loss of elastic tissue in the teristic lesions are flaccid circumscribed areas of slack
dermis. skin with the impression of loss of dermal substance
forming depressions, wrinkling, or sac-like protru-
sions (Fig. 70-1). These atrophic, skin-colored, or blue-
white lesions are 5 to 30 mm in diameter. The number
varies from a few to hundreds. The skin surface can
EPIDEMIOLOGY be wrinkled, thinned, and often depigmented, and a
central depression may be seen. Coalescence of smaller
The lesions in anetoderma usually occur in young lesions can give rise to larger herniations. The examin-
adults between the ages of 15 and 30 years and more ing finger sinks without resistance into a distinct pit
often in women than men. Anetoderma is rare, and with sharp borders as if into a hernia ring (buttonhole
the incidence is unknown. Several hundred cases have sign). The protrusion reappears as soon as the pressure
been reported.1-4 from the finger is removed.4
The most common sites for these asymptomatic
lesions are the chest, back, neck, and upper extremi-
ties. They usually develop in young adults, and new
PATHOGENESIS lesions often continue to form for many years as the
older lesions fail to resolve.
The pathogenesis of anetoderma is unknown. The key Primary anetoderma occurs when there is no under-
defect is damage to the dermal elastic fibers. Aneto- lying associated skin disease (ie, it arises on clinically
derma may be considered to be unusual scars, because normal skin). It is historically subdivided into 2 types:
scars also have decreased elastic tissue. The loss of (a) those with preceding inflammatory lesions, mainly
dermal elastin could be the result of an impaired turn- erythema (the Jadassohn-Pellizzari type), and (b)
over of elastin caused by either increased destruction those without preceding inflammatory lesions (the
or decreased synthesis of elastic fibers.4,5 Recently, a Schweninger-Buzzi type). This classification is only of
decrease in fibulin protein expression was described, historical interest, because the 2 types of lesions can
Kang_CH070_p1193-1202.indd 1193 03/12/18 9:26 am
11 TABLE 70-1
Conditions Associated with Secondary
Anetoderma
Infectious
■ Syphilis
■ Lyme disease
■ Leprosy
■ Molluscum contagiosum
Inflammatory
■ Granuloma annulare
■ Discoid lupus erythematosus
■ Sarcoidosis
■ Lichen planus
Part 11
Tumoral
■ Pilomatricomas
■ Juvenile xanthogranuloma
■ Xanthomas
::
■ Involuted infantile hemangiomas
A ■ Cutaneous B-cell lymphoma
Dermal Connective Tissue Disorders
Other Conditionsa
■ Antiphospholipid syndrome
■ Autoimmune thyroiditis
■ HIV
a
Also associated with primary anetoderma.
also has been described in premature infants, possi-
bly related to the use of cutaneous monitoring leads
or adhesives as well as extreme prematurity.7 Both
primary and secondary types of anetoderma may
be associated with an underlying disease, mainly
antiphospholipid syndrome8 autoimmune thyroiditis
and HIV, in which cases the atrophic lesions do not
necessarily develop in areas of skin inflammation.
Although most cases are sporadic, rare cases of famil-
ial anetoderma have been recently described and are
usually not associated with preexisting lesions.9
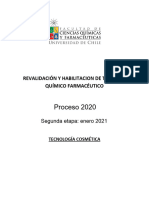
Figure 70-1 Anetoderma. Primary anetoderma. A, Multi-
ple, sharply defined, depressed lesions that look punched
out in the supraclavicular region. B, Soft, sac-like protru-
PATHOLOGY
sions on the back. When depressed, there is the button-
hole phenomenon. This is the same patient as in A. In routinely stained sections, the collagen fibers within
the dermis of affected skin appear normal. Perivascu-
lar lymphocytes, in majority T-helper cells, are often
present in all types of anetoderma and do not correlate
coexist in the same patient; the prognosis and the his- with clinical inflammatory findings.10
topathology are also the same.4 The predominant defect as revealed by elastic tis-
True secondary anetoderma implies that the charac- sue stains is a focal partial or complete loss of elastic
teristic atrophic lesion has appeared in the exact same tissue in the papillary and/or midreticular dermis.
site as a previous specific pathology; the most common There are usually some residual abnormal, irregular,
causes are probably acne and varicella. Numerous and and fragmented elastic fibers (Fig. 70-2). Presumably,
heterogeneous dermatoses have been associated with the weakening of the elastic network leads to flaccidity
secondary anetoderma (Table 70-1), namely infec- and herniation. Direct immunofluorescence sometimes
tious (syphilis, Lyme disease, leprosy, molluscum shows linear or granular deposits of immunoglobulins
contagiosum), inflammatory (granuloma annulare, and complement along the dermal–epidermal junction
discoid lupus, sarcoidosis, lichen planus) and tumoral or around the dermal blood vessels in affected skin.11
(pilomatricomas, juvenile xanthogranuloma, xantho- Electron microscopy demonstrates that the elastic
1194 mas, involuted infantile hemangiomas, cutaneous fibers are fragmented and irregular in shape, occasion-
B-cell lymphoma) to mention only a few. Anetoderma ally engulfed within macrophages.
Kang_CH070_p1193-1202.indd 1194 03/12/18 9:26 am
Papular elastorrhexis is an acquired disorder charac-
terized by white, firm nonfollicular papules measuring
11
1 to 3 mm, evenly scattered on the chest, abdomen, and
back. It usually appears in adolescence or early adult-
hood. The pathology demonstrates focal degeneration
of elastic fibers and normal collagen. There are no asso-
ciated extracutaneous abnormalities. This is believed
by some authors to be a variant of connective tissue
nevi12 or an abortive form of the Buschke-Ollendorff
syndrome,13 whereas others think that these represent
papular acne scars.14 They are differentiated from ane-
toderma by being firm noncompressible lesions.
Middermal elastolysis (MDE) usually consists of
larger areas with diffuse wrinkling without hernia-
Chapter 70 :: Anetoderma and Other Atrophic Disorders of the Skin
tion and with elastolysis limited to the middermis (see
“Middermal Elastolysis” section).
TREATMENT
There is no regularly effective treatment. In secondary
anetoderma, appropriate treatment of the inflamma-
tory underlying condition might prevent new lesions.
Figure 70-2 Anetoderma. Pathology shows decrease of
Various therapeutic modalities have been tried but with
elastic fibers in the papillary and reticular dermis (Weigert
stain). (Used with permission from Victor Kokta, MD.) no improvement of existing atrophic lesions, includ-
ing intralesional injections of triamcinolone, and sys-
temic administration of aspirin, dapsone, phenytoin,
penicillin G (benzylpenicillin), and vitamin E. Some
authors have reported improvement with hydroxy-
DIFFERENTIAL DIAGNOSIS chloroquine. In patients with limited lesions that are
cosmetically objectionable, surgical excision may be
Anetoderma must be differentiated from other disor- useful. Ablative and nonablative fractionated lasers
ders of elastic tissue as well as atrophies of the connec- have shown some improvement in limited cases.15,16
tive tissue (Table 70-2). The use of soft-tissue fillers is inconclusive.
Keloids form nodules that are much firmer on pal-
pation. A history of trauma is often elicited, and the
pathology is very distinct.
Glucocorticoid-induced atrophy occurs most com-
OTHER ATROPHIC
monly over the triceps or buttocks at sites where injec-
tions are usually given. Clinically, the lesions resemble
DISORDERS OF THE SKIN
atrophoderma. History is obviously most helpful in
making the diagnosis. On histopathology, polarization
MIDDERMAL ELASTOLYSIS
may show the steroid crystals in the dermis.
Nevus lipomatosus superficialis of Hoffman and MDE is a rare acquired disorder of elastic tissue. It is
Zurhelle presents as a clustered group of soft, skin- characterized by patches and plaques of diffuse, fine,
colored to yellow nodules usually on the lower trunk wrinkled skin, most often located on the trunk, neck,
and buttocks and present since birth. Histology shows and arms. In 1977, Shelley and Wood reported the first
ectopic mature lipocytes located in the dermis. case of “wrinkles due to idiopathic loss of middermal
elastic tissue.”17 Since then, approximately 100 cases
have been reported. The vast majority of patients are
white women between the ages of 30 and 50 years.17-19
TABLE 70-2
Differential Diagnosis of Primary Anetoderma PATHOGENESIS
ELEVATED DEPRESSED The pathogenesis of this acquired elastic tissue degen-
Secondary anetoderma Secondary anetoderma eration is still unknown. Ultraviolet exposure has
Acne scars Glucocorticoid-induced atrophy been postulated to be a major contributing factor in
Keloids Acne scars the degeneration of elastic fibers,20 including natural
Nevus lipomatosus superficialis sunlight and narrowband ultraviolet B phototherapy.21
Papular elastorrhexis Other possible mechanisms include defects in the syn-
Connective tissue nevi 1195
thesis of elastic fibers, autoimmunity against elastic
Kang_CH070_p1193-1202.indd 1195 03/12/18 9:26 am
11 fibers, and damage to elastic fibers through the release
of elastase by inflammatory cells or fibroblasts. Of
PATHOLOGY
interest, MDE has been reported in a case of immune Histopathology shows a normal epidermis and, occa-
reconstitution inflammatory syndrome.22 Some data sionally, a mild perivascular infiltrate in the dermis.
suggest that inflammatory processes and an imbalance The characteristic features are seen on elastic tissue
between matrix metalloproteinases and tissue inhibi- stains (such as Verhoeff-van Gieson or Weigert) and
tor of metalloproteinases are probably involved in the reveal a selective band-like loss of elastic fibers in the
pathogenesis of MDE, in addition to CD34+ dendritic middermis (see Fig. 70-3B). Macrophagic elastophago-
fibroblasts.23 A decrease of lysyl oxidase-like 2 expres- cytosis can occasionally be seen. There is preservation
sion potentially has an effect on elastin renewal.24 A of normal elastic tissue in the superficial papillary der-
recent study has shown that dermal fibulin-4 and mis above, in the reticular dermis below, and along
fibulin-5 are significantly diminished in MDE compared adjacent hair follicles. Electron microscopy studies
with controls. This data indicates that the pathogenesis have shown phagocytosis by macrophages of both
is not only secondary to an elastolytic overactivity, but normal and degenerated elastic fiber tissue.26
Part 11
also altered reassembly of elastic fibers.6
DIFFERENTIAL DIAGNOSIS
CLINICAL FEATURES MDE must be differentiated from the other common
::
MDE is characterized by asymptomatic, well-demar- disorders of elastic tissue.
Dermal Connective Tissue Disorders
cated, or diffuse areas of fine wrinkling (type I), Solar elastosis differs by its onset in an older age
usually in a symmetric distribution (Fig. 70-3A). Dis- group, location in only sun-exposed areas, yellowish
crete perifollicular papules can be seen in some cases color, and coarser wrinkling, as well as by hyperpla-
(type II), leaving the hair follicle itself as an indented sia and abnormalities of elastic fibers and basophilic
center. More rarely, a reticular pattern (type III) with degeneration of the collagen in the papillary dermis.
erythematous patches and telangiectasia can be seen. Anetoderma is characterized clinically by smaller
Lesions are typically found on the trunk, neck, and soft macules and papules instead of diffuse wrinkling,
upper extremities. They are chronic and give the skin and histologically by elastolysis that can occur in any
a prematurely aged appearance. There is usually no layer of the dermis.
history of a preceding inflammatory dermatosis, but Perifollicular elastolysis27 differs by a selective and
some patients report mild-to-moderate erythema and almost complete loss of elastic fibers surrounding hair
more rarely urticarial lesions or granuloma annulare. follicles compared with preservation of elastic fibers
There is usually no associated systemic involvement. around follicles in MDE. Elastase-producing Staphylo-
Although the diagnosis of MDE is mainly based coccus epidermidis was found in the hair follicles and is
on clinical and histopathologic features, noninvasive the presumed etiology of this condition.
diagnostic techniques (optical coherence microscopy Postinflammatory elastolysis and cutis laxa were
or high-frequency ultrasound) may be helpful.25 originally described in young girls of African descent.
A B
Figure 70-3 Middermal elastolysis. A, Well-circumscribed area of fine wrinkling on the neck of a middle-aged woman.
(Used with permission from Richard Dubuc, MD.) B, Histology of middermal elastolysis. Note selective loss of elastic fibers
1196 in the middermis. Normal elastic tissue is preserved in the superficial papillary dermis and in the reticular dermis (Weigert
stain). (Used with permission from Danielle Bouffard, MD.)
Kang_CH070_p1193-1202.indd 1196 03/12/18 9:26 am
An inflammatory phase, consisting of indurated
plaques or urticaria, malaise, and fever, preceded the
as the development of pelvic relaxation and clinical
prolapse.33
11
diffuse wrinkling, atrophy, and severe disfigurement. The striae associated with systemic corticosteroid
Insect bites may be the trigger for the initial inflamma- therapy and Cushing syndrome can be larger and
tory lesions.28 more widely distributed.
TREATMENT PATHOLOGY
There is no known effective treatment for MDE. Sun- Histologic findings show a decrease in dermal thick-
screens, colchicine, chloroquine, vitamin E, and topical ness and in collagen in the upper dermis. The collagen
retinoic acid have been tried without good success.17-19 bundles are thinned and lie parallel to the epidermis,
Topical soybean extract and eicosapentaenoic acid but they are also arranged transversely to the direction
may prove to be interesting options.18 of the striae. Alterations in elastic fibers are variable,
but dermal elastin can be fragmented, and specific
Chapter 70 :: Anetoderma and Other Atrophic Disorders of the Skin
elastin staining can demonstrate a marked reduction
STRIAE in visible elastin content compared with adjacent nor-
mal dermis.34 There is absence of both hair follicles and
other appendages.
Chapters 105 and 137 provide additional discussion of
striae.
Striae are very common and usually develop
between the ages of 5 and 50 years.29 They occur about
DIFFERENTIAL DIAGNOSIS
twice as frequently in women as in men. They com- The diagnosis of striae distensae is usually straightfor-
monly develop during puberty, with an overall inci- ward, but the differential diagnosis does include linear
dence of 25% to 35%,30 or during pregnancy, with an focal elastosis (elastotic striae) that was first described
incidence of up to 90%.31 by Burket and colleagues in 1989.35 Linear focal elasto-
sis is characterized by rows of yellow palpable striae-
like bands on the lower back. Unlike striae, the lesions
PATHOGENESIS are raised and yellow rather than depressed and white.
The factors leading to the development of striae have Elderly men are most commonly affected, although
not been fully elucidated. Striae distensae are the cases in teenagers have been described. Linear focal
results of breaks in the connective tissue, resulting in elastosis is probably not an uncommon condition. His-
dermal atrophy. Many factors, including hormones tologically, there is a focal increase in the number of
(particularly corticosteroids), mechanical stress, and elongated or fragmented elastic fibers and a thickened
genetic predisposition, appear to play a role. dermis. It is postulated that linear focal elastosis may
represent an excessive regenerative process of elastic
fibers and could be thought of as a keloidal repair of
CLINICAL FEATURES striae distensae.36
Striae are usually multiple, symmetric, well-defined
linear atrophic lesions that follow the lines of cleavage.
Initially, striae appear as red-to-violaceous elevated
TREATMENT37
lines (striae rubra). Over time, the color gradually Striae distensae have no medical consequences, but
fades, and the lesions become atrophic, with the skin they are frequently distressing to those affected. As
surface exhibiting a fine, white, wrinkled appearance stretch marks tend to regress spontaneously to some
(striae alba). The striae can measure several centime- degree over time, the usefulness of treatments that have
ters in length and a few millimeters to a few centime- been tried without case controls is difficult to assess.
ters in width. Topical treatments that have shown some improve-
During puberty, striae appear in areas where there is ment of early stage striae are tretinoin 0.1% cream,38
a rapid increase in size. In girls, the most common sites a combination of 0.05% tretinoin/20% glycolic acid,
are the breasts, thighs, hips, and buttocks, whereas or 10% l-ascorbic acid/20% glycolic acid.39 Several
in boys, they are seen on the shoulders, lumbosacral lasers40 have been used in treating striae: the 585-nm
region, and thighs. Other less-common sites include pulsed-dye laser has been demonstrated to be of some
the abdomen, upper arms, neck, and axillae. efficacy in improving the appearance of striae rubra
Striae distensae are a common finding on the abdo- but has no effect on striae alba. Preliminary data have
men, and less so on the breasts and thighs, of preg- shown improvement of striae alba with fractionated
nant women, especially during the last trimester. They microneedle radiofrequency in combination with frac-
are more common in younger primigravidas than in tional carbon dioxide laser.41 Microneedling and com-
older pregnant women, and are associated with larger bination treatment with radiofrequency and pulsed
weight gain and/or with babies of higher birth weight. magnetic fields also appear promising.42,43 The long-
Striae gravidarum can be associated with a higher term future of treatment strategies is encouraging with 1197
risk of lacerations during vaginal delivery,32 as well the advance in laser technologies.
Kang_CH070_p1193-1202.indd 1197 03/12/18 9:26 am
11 IDIOPATHIC
ATROPHODERMA OF PASINI
AND PIERINI
Idiopathic atrophoderma of Pasini and Pierini is a
form of dermal atrophy that presents as 1 or several
sharply demarcated depressed patches with no out-
pouching, usually on the back of adolescents or young
adults.44 Whether atrophoderma is a nonsclerotic, pri-
marily atrophic variant of morphea or a separate dis-
tinct entity is still debated.45
Part 11
EPIDEMIOLOGY AND
PATHOGENESIS
::
This disorder is more frequently encountered in
Dermal Connective Tissue Disorders
women than in men, with a ratio of 6:1. It usually
starts insidiously in young individuals in the second Figure 70-4 Atrophoderma of Pasini and Pierini. Brownish
or third decades of life. Congenital cases have been depressed lesions on the lower back.
reported.46
Its relationship to morphea is favored by its strik-
ing clinical and histologic similarities to the atrophy are present, they can have the appearance of Swiss
seen at sites of regressing plaques of morphea. Anti- cheese. They are even more apparent when pres-
bodies to Borrelia burgdorferi have been reported.47 ent on the back because the dermis is thicker in this
Typical lesions of morphea, lichen sclerosus, and area. The skin surrounding the patches is normal in
atrophoderma have been observed to occur simul- appearance, and there is no erythema or lilac ring as
taneously in the same patient, but in different in morphea.
areas, supporting the view that these conditions are The course of this benign disease is progressive,
related.48 In a series of 139 patients, 24 (17%) had and lesions can continue to appear for decades before
white induration in the central portions of their atro- reaching a standstill. Transformation to generalized
phic lesions, and 30 (22%) had superficial plaques morphea has not been observed.
of morphea coexisting in areas outside of their atro-
phic foci.49 However, to some, the different course
and outcome of atrophoderma of Pierini and Pasini
PATHOLOGY
as compared with morphea justifies preservation of The histologic picture is generally not diagnostic.47,49
a distinct name. The epidermis is usually normal. Collagen bundles
in the middermis and reticular dermis show varying
degrees of homogenization and clumping. Dermal
CLINICAL FEATURES thickness is eventually reduced when compared with
adjacent normal skin. Some irregular clumping and loss
The lesions are well-demarcated depressed patches,
of elastic fibers were described in earlier case reports,
usually occurring on the trunk, especially on the back
but in most series, no abnormality was seen with elas-
and lumbosacral region, followed in frequency by the
tic tissue stains; consequently, this is not of diagnostic
chest, arms, and abdomen.47,49 The distribution is often
value. The appendages are usually preserved. If sclero-
symmetric and bilateral.
dermatous changes appear in preexisting patches, the
The lesions are single or multiple and usually round
histology reveals varying degrees of collagen sclerosis
or ovoid, ranging in size from a few centimeters to
resembling morphea. A recent study using multipho-
patches covering large areas of the trunk (Fig. 70-4).
ton microscopy suggests that the atrophic appearance
They are usually asymptomatic and lack inflamma-
of atrophoderma lesions reflect changes in the organi-
tion. When lesions coalesce, they can form large, irreg-
zation of collagen and elastic fibers and not variation
ular, brown patches but can be hypopigmented.49 The
in their content.50
surface of the skin is normal in appearance, and there
is no skin induration or sclerosis.
The borders or edges of these lesions are sharply
defined, and they are usually described as abrupt,
DIFFERENTIAL DIAGNOSIS
“cliff-drop” borders ranging from 1 to 8 mm in depth, The differential diagnosis is to be made with active
although they can have a gradual slant.46 These lesions of morphea that usually present as indurated,
1198 depressed patches are characteristic and give the often hyperpigmented plaques with a characteristic
impression of inverted plateaus, or, if multiple lesions peripheral lilac rim.
Kang_CH070_p1193-1202.indd 1198 03/12/18 9:26 am
TREATMENT 11
No treatment has proven effective. Penicillin and dox-
ycycline have been used with poor results. Dramatic
response to oral hydroxychloroquine was reported in
1 patient.51 Q-switched alexandrite laser can maybe
help decrease hyperpigmentation.52
FOLLICULAR
ATROPHODERMA
Follicular atrophoderma refers to dimple-like depres-
sions at the follicular orifices. It can occur as an iso-
Chapter 70 :: Anetoderma and Other Atrophic Disorders of the Skin
lated defect of limited extent, in association with a
variety of disorders in which hair follicles are plugged
with keratin, or with rare genodermatoses.53, 54
Distinctive ice-pick depressions around hair follicles
can be seen most commonly on the cheeks and on the
back of the hands or feet. These pitted scars can pres-
ent at birth or early in life. A family history may be Figure 70-5 Atrophoderma vermiculatum. Multiple, small,
present. Follicular atrophoderma occurs in the condi- pitted scars on the cheek of a young girl.
tions described in the following sections.
over the malar area and progresses to involve the eye-
brows, scalp, and extremities, with scarring alopecia.
ATROPHODERMA This condition is inherited in an X-linked recessive
fashion in some patients. Ulerythema ophryogenes (or
VERMICULATUM keratosis pilaris atrophicans faciei) differs from atro-
phoderma vermiculatum by affecting primarily the
Atrophoderma vermiculatum is a term that applies lateral portion of the eyebrows (ophryogenes) with
when the lesions are found exclusively on the cheeks.55 erythema, follicular papules, and alopecia (Fig. 70-6).
It is a condition that can either occur sporadically, The underlying pathologic defect in these disorders
be inherited as an autosomal dominant disorder, be appears to be abnormal follicular hyperkeratinization
part of a group of related diseases including kerato- of the upper third of the hair shaft leading to obstruc-
sis pilaris atrophicans, or be associated with various tion of the growing hair and production of chronic
syndromes. inflammation. The end result of this process is scarring
Multiple inflammatory symmetric papules on the below that level. Histopathology is usually not very
cheeks, presumably centered around hair follicles,
may precede the atrophic lesions. These papules then
go on to develop pitted, atrophic, and depressed scars
in a reticulated or honeycomb pattern (Fig. 70-5). These
lesions can extend to the forehead and preauricular
regions. This condition usually has its onset in child-
hood or, less often, around puberty. Men and women
seem to be affected equally. It usually has a slow pro-
gressive course.
KERATOSIS PILARIS
ATROPHICANS
Keratosis pilaris atrophicans55,56 can include atropho-
derma vermiculatum but also a group of closely related
disorders that includes keratosis follicularis spinulosa
decalvans and ulerythema ophryogenes. These condi-
tions are characterized by keratotic follicular papules,
variable degrees of inflammation, and secondary atro-
phic scarring. Keratosis follicularis spinulosa decal- Figure 70-6 Ulerythema ophryogenes. Erythematous fol- 1199
vans begins in infancy with keratotic follicular papules licular papules and scarring alopecia of the eyebrow.
Kang_CH070_p1193-1202.indd 1199 03/12/18 9:26 am
11 helpful and shows dilated follicles, sometimes asso-
ciated with plugging, inflammation, and sclerosis of
it is usually lethal in hemizygous males. The under-
lying molecular defect consists of mutations in the
dermal collagen. emopamil-binding protein gene at Xp11.23-p11.22.62
The clinical manifestations include an ichthyosiform
scaling erythroderma patterned along the lines of
Blaschko that usually resolves during the first year
ASSOCIATED SYNDROMES of life and is replaced by bands of follicular atropho-
derma. Hyperpigmentation, cataracts, scarring alope-
The various syndromes that include atrophoderma cia, saddle-nose deformity, asymmetric limb reduction
vermiculatum are Rombo syndrome (milia, telangiec- defects, and stippled calcifications of the epiphyses
tasias, basal cell carcinomas, hypotrichosis, acral cya- can be seen. Ichthyosis with keratotic follicular plugs
nosis, and, rarely, trichoepitheliomas), Nicolau-Balus containing dystrophic calcification in newborns are
syndrome (syringomas and milia), Tuzun syndrome distinctive histopathologic features.63
(scrotal tongue), Loeys-Dietz syndrome,57 and finally
Part 11
the Braun-Falco-Marghescu syndrome (palmoplantar
hyperkeratosis and keratosis pilaris). OTHER ATROPHIES OF THE
CONNECTIVE TISSUE
::
THERAPY Many systemic conditions (scleroderma [see Chap. 63],
Dermal Connective Tissue Disorders
lupus erythematosus [see Chap. 61], dermatomyositis
[see Chap. 62]), and genodermatoses (poikiloderma
These disorders are mainly a cosmetic but vexing prob- congenitale, dyskeratosis congenita, Cockayne syn-
lem. Various topical treatments, including emollients, drome, Hallermann-Streiff syndrome) have skin atro-
corticosteroids, tretinoin, and keratolytics, have shown phy as an associated finding and are described in other
no consistent benefit. Systemic isotretinoin has been chapters.
shown to stop progression and to induce remission
in some cases.55 Dermabrasion as well as carbon diox-
ide and 585-nm pulsed-dye lasers are other options to
improve the appearance of the atrophic scars.58 REFERENCES
1. Jadassohn J. Uber eine eigenartige form von “atrophica
maculosa cutis”. Arch Derm Syphilol. 1892;24:342-358.
BAZEX-DUPRÉ-CHRISTOL 2. Schweninger E, Buzzi F. Multiple benign tumor-like new
growths of the skin. In: Internationaler Atlas Sellltener
SYNDROME (OMIM 301845) Hautkrankheiten, plate 15. Leipzig, Germany: L Voss;
1891.
Bazex-Dupré-Christol syndrome is characterized by 3. Venencie PY, Winkelmann RK, Moore BA. Anetoderma:
follicular atrophoderma, milia, multiple basal cell car- clinical findings, associations, and long-term follow-
up evaluations. Arch Dermatol. 1984;120:1032-1039.
cinomas, hypotrichosis, and localized hypohidrosis.59
4. Kineston DP, Xia Y, Turiansky GW. Anetoderma: a
The follicular atrophoderma described as multiple case report and review of the literature. Cutis. 2008;
ice-pick marks or patulous follicles can be found most 81:501-506.
commonly on the dorsa of the hands. It is inherited in 5. Venencie PY, Bonnefoy A, Gogly B, et al. Increased
an X-linked dominant fashion, and the gene has been expression of gelatinases A and B by skin explants
linked to Xq24-q27.60 Additional reported findings from patients with anetoderma. Br J Dermatol.
include facial hyperpigmentation, hair shaft dystrophy, 1997;137:517-525.
and multiple trichoepitheliomas. This syndrome might 6. Gambichler T, Reininghaus L, Skrygan M, et al. Fibu-
be better considered as an ectodermal dysplasia.61 lin protein expression in mid-dermal elastolysis and
anetoderma: a study of 23 cases. Acta Derm Venereol.
2016;96:708-710.
7. Gougeon E, Beer F, Gay S, et al. Anetoderma of prema-
CONRADI-HÜNERMANN- turity: an iatrogenic consequence of neonatal inten-
sive care. Arch Dermatol. 2010;146:565-567.
HAPPLE SYNDROME 8. Hodak E, David M. Primary anetoderma and antiphos-
pholipid antibodies—review of the literature. Clin Rev
(X-LINKED DOMINANT Allergy Immunol. 2007;32:162-166.
9. Patrizi A, Neri I, Virdi A, et al. Familial anetoderma: a
CHONDRODYSPLASIA report of two families. Eur J Dermatol. 2011;21:680-685.
10. Venecie PY, Wilkelmann RK. Histopathologic findings
PUNCTATA, CDPX2, in anetoderma. Arch Dermatol. 1984;120:1040-1044.
OMIM 302960) 11. Bergman R, Friedman-Birnbaum R, Hazaz B, et al. An
immunofluorescence study of primary anetoderma.
Clin Exp Dermatol. 1990;15:124-130.
1200 Conradi-Hünermann-Happle syndrome is an X-linked 12. Sears J, Stone M, Argenyi Z. Papular elastorrhexis:
dominant disorder that occurs only in girls because a variant of connective tissue nevus: case reports
Kang_CH070_p1193-1202.indd 1200 03/12/18 9:26 am
and review of the literature. J Am Acad Dermatol.
1988;19:409-414.
34. Arem A, Ward Kisher C. Analysis of striae. Plast Reconstr
Surg. 1980;65:22-29.
11
13. Schirren H, Schirren C, Stolz W, et al. Papular elastor- 35. Burket JM, Zelickson AS, Padilla RS. Linear focal elas-
rhexis: a variant of dermatofibrosis lenticularis dissem- tosis (elastotic striae). J Am Acad Dermatol. 1989;
inata (Buschke-Ollendorff syndrome). Dermatology. 20:633-636.
1994;189:368-372. 36. Hashimoto K. Linear focal elastosis: keloidal repair of
14. Wilson B, Dent C, Cooper P. Papular acne scars; a com- striae distensae. J Am Acad Dermatol. 1998;39:309-313.
mon cutaneous finding. Arch Dermatol. 1990;126: 37. Al-Himdani S, Ud-Din S, Gilmore S, et al. Striae dis-
797-800. tensae: a comprehensive review and evidence-based
15. Wang K, Ross NA, Saedi N. Anetoderma treated with evaluation of prophylaxis and treatment. Br J Dermatol.
combined 595-nm pulsed-dye laser and 1550-nm 2014;170:527-547.
non-ablative fractionated laser. J Cosmet Laser Ther. 38. Kang S. Topical tretinoin therapy for management of
2016;18:38-40. early striae. J Am Acad Dermatol. 1998;39:S90-S92.
16. Cho S, Jung JY, Lee JH. Treatment of anetoderma 39. Ash K, Lord J, Zukowski M, et al. Comparison of topical
occurring after resolution of Stevens-Johnson syn- therapy for striae alba (20% glycolic acid/0.05% treti-
drome using an ablative 10,600-nm carbon dioxide noin versus 20% glycolic acid/10% L-ascorbic acid).
Chapter 70 :: Anetoderma and Other Atrophic Disorders of the Skin
fractional laser. Dermatol Surg. 2012;38:677-679. Dermatol Surg. 1998;24:849-856.
17. Shelley WB, Wood MG. Wrinkles due to idiopathic 40. Aldahan AS, Shah VV, Mlacker S, et al. Laser and light
loss of mid-dermal elastic tissue. Br J Dermatol. 1977; treatments for striae distensae: a comprehensive
97:441-445. review of the literature. Am J Clin Dermatol. 2016;
18. Hardin J, Dupuis E, Haber RM. Mid-dermal elastolysis: 17:239-256.
a female-centric disease; case report and updated 41. Fatemi Naeini F, Behfar S, Abtahi-Naeini B, et al. Prom-
review of the literature. Int J Women’s Dermatol. ising option for treatment of striae alba: fractionated
2015;1:126-130. microneedle radiofrequency in combination with
19. Gambichler T. Mid-dermal elastolysis revisited. Arch fractional carbon dioxide laser. Dermatol Res Pract.
Dermatol Res. 2010;302:85-93. 2016;2016:2896345.
20. Snider RL, Lang PG, Maize JC. The clinical spectrum 42. Ramaut L, Hoeksema H, Pirayesh A, et al. Micronee-
of mid-dermal elastolysis and the role of UV light dling: where do we stand now? A systematic review
in its pathogenesis. J Am Acad Dermatol. 1993;28: of the literature. J Plast Reconstr Aesthet Surg.
938-942. 2018;71:1-14.
21. Vatve M, Morton R, Bilsland D. A case of mid-dermal 43. Dover JS, Rothaus K, Gold MH. Evaluation of safety and
elastolysis after narrowband ultraviolet B photother- patient subjective efficacy of using radiofrequency
apy. Clin Exp Dermatol. 2009;34:263-264. and pulsed magnetic fields for the treatment of striae
22. Cota C, Latini A, Lora V, et al. Mid-dermal elastolysis as (stretch marks). J Clin Aesthet Dermatol. 2014;7:30-33.
a manifestation of immune reconstitution inflamma- 44. Canizares O, Sachs PM, Jaimovich L, et al. Idiopathic
tory syndrome in an HIV-infected patient. J Am Acad atrophoderma of Pasini and Pierini. Arch Dermatol.
Dermatol. 2014;71:e134-e135. 1958;77:42-60.
23. Gambichler T, Breuckmann F, Kreuter A, et al. Immuno- 45. Jablonska S, Blaszczyk M. Is superficial morphea
histochemical investigation of mid-dermal elastolysis. synonymous with atrophoderma Pierini-Pasini? J Am
Clin Exp Dermatol. 2004;29:192-195. Acad Dermatol. 2004;50:979-980.
24. Gambichler T, Skyrgan M. Decreased lysyl oxidase-like 46. Kang CY, Lam J. Congenital idiopathic atrophoderma
2 expression in mid-dermal elastolysis. Arch Dermatol of Pierini and Pasini. Int J Dermatol. 2015;54:e44-e46.
Res. 2013;305:359-363. 47. Buechner SA, Rufli T. Atrophoderma of Pasini and Pier-
25. Scola N, Goulimus A, Gambichler T. Non-invasive ini: clinical and histopathologic findings and antibod-
imaging of mid-dermal elastolysis. Clin Exp Dermatol. ies to Borrelia burgdorferi in thirty-four patients. J Am
2011;36:155-160. Acad Dermatol. 1994;30:441-446.
26. Harmon CB, Su WP, Gagne EJ, et al. Ultrastructural 48. Amano H, Nagai Y, Ishikawa O. Multiple morphea
evaluation of mid-dermal elastolysis. J Cutan Pathol. coexistent with atrophoderma of Pierini-Pasini (APP):
1994;21:233-238. APP could be abortive morphea. J Eur Acad Dermatol
27. Varadi DP, Saqueton AC. Perifollicular elastolysis. Br J Venereol. 2007;21:1254-1256.
Dermatol. 1970;83:143. 49. Saleh Z, Abbas O, Dahdah MJ, et al. Atrophoderma
28. Verhagen AR, Woederman MJ. Post-inflammatory elas- of Pierini and Pasini: a clinical and histopathological
tolysis and cutis laxa. Br J Dermatol. 1975;92:183-190. study. J Cutan Pathol. 2008;35:1108-1114.
29. Garcia-Hidalgo L, Orozco-Topete R, Gonzalez-Barranco 50. Vieira-Damiani G, Lage D, Christofoletti Daldon PÉ,
J, et al. Dermatoses in 156 obese adults. Obes Res. et al. Idiopathic atrophoderma of Pasini and Pierini: a
1999;7:299-302. case study of collagen and elastin texture by multipho-
30. Ammar NM, Rao B, Schwartz RA, et al. Adolescent ton microscopy. J Am Acad Dermatol. 2017;77:930-937.
striae. Cutis. 2000;65:69-70. 51. Carter JD, Valeriano J, Vasey FB. Hydroxychloroquine
31. Farahnik B, Park K, Kroumpouzos G, et al. Striae gravi- as treatment for atrophoderma of Pierini and Pasini.
darum: risk factors, prevention and management. Int J Int J Dermatol. 2006;45:1255-1256.
Womens Dermatol. 2017;3:77-85. 52. Arpey CJ, Patel DS, Stone MS, et al. Treatment of atro-
32. Wahman AJ, Finan MA, Emerson SC. Striae gravi- phoderma of Pierini and Pasini-associated hyperpig-
darum as a predictor of vaginal lacerations at delivery. mentation with the Q-switched alexandrite laser: a
South Med J. 2000;93:873-876. clinical, histologic, and ultrastructural appraisal. Lasers
33. Salter SA, Batra RS, Rohrer TE, et al. Striae and pel- Surg Med. 2000;27:206-212.
vic relaxation: two disorders of connective tissue 53. Miescher G. Atypische Chondrodystrophie, Typus
with a strong association. J Invest Dermatol. 2006; morquino kombiniert mit follikularer atrophodermie. 1201
126:1745-1748. Dermatologica. 1944;89:38-51.
Kang_CH070_p1193-1202.indd 1201 03/12/18 9:26 am
11 54. Curth HO. The genetics of follicular atrophoderma.
Arch Dermatol. 1978;114:1479-1483.
61. Castori M, Castiglia D, Passarelli F, et al. Bazex-
Dupré-Christol syndrome: an ectodermal dysplasia
55. Luria RB, Conologue T. Atrophoderma vermiculatum: with skin appendage neoplasms. Eur J Med Genet.
a case report and review of the literature on keratosis 2009:52:250-255.
pilaris atrophicans. Cutis. 2009;83:83-86. 62. Canueto J, Giros M, Ciria S, et al. Clinical, molecular and
56. Callaway SR, Lesher JL. Keratosis pilaris atrophicans: biochemical characterization of nine Spanish fami-
case series and review. Pediatr Dermatol. 2004;21:14-17. lies with Conradi-Hünermann-Happle syndrome: new
57. van Dijk FS, Brittain H, Boerma R, et al. Atrophoderma insights into X-linked dominant chondrodysplasia
vermiculatum: a cutaneous feature of Loeys-Dietz punctata with a comprehensive review of the literature.
syndrome. JAMA Dermatol. 2015;151:675-677. Br J Dermatol. 2012;166:830-838.
58. Handrick C, Alster T. Laser treatment of atrophoderma 63. Hoang MP, Carder KR, Pandya AG, et al. Ichthyosis and
vermiculata. J Am Acad Dermatol. 2001;44:693-695. keratotic follicular plugs containing dystrophic calci-
59. Torrelo A, Sprecher E, Medeiro IG, et al. What syn- fication in newborns: distinctive histopathologic fea-
drome is this? Basex-Dupré-Christol syndrome. Pediatr tures of X-linked dominant chondrodysplasia punctata
Dermatol. 2006;23:286-290. (Conradi-Hünermann-Happle syndrome). Am J Derma-
60. Parren LJ, Abuzahra F, Wagenvoort T, et al. Linkage topathol. 2004;26:53-58.
Part 11
refinement of Bazex-Dupré-Christol syndrome to
an 11·4-Mb interval on chromosome Xq25-27.1. Br J
Dermatol. 2011;165:201-203.
::
Dermal Connective Tissue Disorders
1202
Kang_CH070_p1193-1202.indd 1202 03/12/18 9:26 am
You might also like
- How To Cut Your Own or Anybody Else's Hair - Bob BentDocument118 pagesHow To Cut Your Own or Anybody Else's Hair - Bob BentChihYang Hsieh100% (12)
- 10 Patho Skin PathologyDocument27 pages10 Patho Skin PathologyMartin Tan100% (1)
- Core Curriculum WOCNSDocument1,212 pagesCore Curriculum WOCNSJerry MaguireNo ratings yet
- Face CleansingDocument2 pagesFace Cleansingbhargav patelNo ratings yet
- 0 Basic Principles of DermatologyDocument42 pages0 Basic Principles of Dermatologymusatii100% (1)
- Revised Curriculum For Fellowship in Anti Ageing &Document24 pagesRevised Curriculum For Fellowship in Anti Ageing &drraj23121No ratings yet
- Skin DiseasesDocument11 pagesSkin DiseasesPipoy Amy100% (1)
- Hair CareDocument112 pagesHair CarestudentNo ratings yet
- The Integumentary SystemDocument33 pagesThe Integumentary SystemMica BernardoNo ratings yet
- Aging Skin Fore 06Document12 pagesAging Skin Fore 06Felp ScholzNo ratings yet
- SDL IntegumentaryDocument4 pagesSDL IntegumentaryMonique Eloise GualizaNo ratings yet
- Obagi Price ListDocument3 pagesObagi Price ListANDELYNNo ratings yet
- NPIAP Staging PosterDocument2 pagesNPIAP Staging PosterDr. Hüseyin ŞAHİNNo ratings yet
- All About Hair: Presented By: R, E. O. GaasDocument25 pagesAll About Hair: Presented By: R, E. O. GaasPrincess Joy Morales100% (1)
- Skin Integrity & Wound CareDocument108 pagesSkin Integrity & Wound CareRon Ar IcaNo ratings yet
- Steven Johnson SyndromeDocument24 pagesSteven Johnson SyndromeNatalia MagdalenaNo ratings yet
- Pressure Injury Documentation and Assessment: A Guide To State-Of-The-Art Staging and Recording of PisDocument7 pagesPressure Injury Documentation and Assessment: A Guide To State-Of-The-Art Staging and Recording of PisAlexis TrivinoNo ratings yet
- Skin: Unique Anatomy: The IowerDocument3 pagesSkin: Unique Anatomy: The IowerAnonymous kdBDppigENo ratings yet
- HAPP-PICO Tissue Pathology Journal ResearchDocument4 pagesHAPP-PICO Tissue Pathology Journal ResearchArlynn MartinezNo ratings yet
- Dermatopathology For The Surgical Pathologist A Pattern-Based Approach To The Diagnosis of Inflammatory Skin Disorders Part IDocument21 pagesDermatopathology For The Surgical Pathologist A Pattern-Based Approach To The Diagnosis of Inflammatory Skin Disorders Part IkarigargiuloNo ratings yet
- Giant Skin TagDocument2 pagesGiant Skin Tagshf.mxlikNo ratings yet
- Painful Tumors of The Skin – From ENGLAND To LEND AN EGG To BLEND TAN EGG.Document4 pagesPainful Tumors of The Skin – From ENGLAND To LEND AN EGG To BLEND TAN EGG.KuldeepSinghBanaNo ratings yet
- Case Report: Primary AnetodermaDocument3 pagesCase Report: Primary AnetodermaAizat KamalNo ratings yet
- P7.2. Soft Tissue TraumaDocument12 pagesP7.2. Soft Tissue TraumaCharles HuayraNo ratings yet
- Skin Anatomy and Flap Physiology: P. S. MDDocument15 pagesSkin Anatomy and Flap Physiology: P. S. MDAncaVerdesNo ratings yet
- Medterm IntegumentaryDocument10 pagesMedterm IntegumentaryVince BalloriNo ratings yet
- 2017 - Tecnología CosméticaDocument54 pages2017 - Tecnología CosméticaCésar Rosado Avila ToñoNo ratings yet
- Tecnologí A Cosmé Tica 2020Document56 pagesTecnologí A Cosmé Tica 2020HAIDY FRANCONo ratings yet
- Dermatology For Plastic Surgeon I - Skin Care and Benign Dermatologic ConditionsDocument10 pagesDermatology For Plastic Surgeon I - Skin Care and Benign Dermatologic ConditionsNabil MaulanaNo ratings yet
- MyopatiDocument19 pagesMyopatiIndra kusuma mardiaNo ratings yet
- Safari - Feb 21, 2024 at 11:56 AMDocument1 pageSafari - Feb 21, 2024 at 11:56 AMsyansyncNo ratings yet
- UNP-CN Do Not Reproduce: Learning Pocket DescriptionDocument37 pagesUNP-CN Do Not Reproduce: Learning Pocket DescriptionJanelle Cabida SupnadNo ratings yet
- 5.12 Venous UlcersDocument4 pages5.12 Venous UlcersCollen LihakaNo ratings yet
- A Review of Skin and The Effects of Aging On Skin Structure and Function - Skin Turnover TimeDocument10 pagesA Review of Skin and The Effects of Aging On Skin Structure and Function - Skin Turnover TimeEUNPYO LEENo ratings yet
- Anatomy, Skin (Integument) - StatPearls - NCBI BookshelfDocument4 pagesAnatomy, Skin (Integument) - StatPearls - NCBI Bookshelfputri aisheNo ratings yet
- Document - 119 - 322how To Download Dermatology For Advanced Practice Clinicians 1St Edition Ebook PDF Ebook PDF Docx Kindle Full ChapterDocument36 pagesDocument - 119 - 322how To Download Dermatology For Advanced Practice Clinicians 1St Edition Ebook PDF Ebook PDF Docx Kindle Full Chapterdoug.wiggins940100% (25)
- APP - The International Society of Dermatology APPDocument3 pagesAPP - The International Society of Dermatology APPAndrés WunderwaldNo ratings yet
- Pathology CH 24 (Robbins Edition 2017 891-910)Document20 pagesPathology CH 24 (Robbins Edition 2017 891-910)putri aisheNo ratings yet
- Basic Physiology of The SkinDocument4 pagesBasic Physiology of The SkinRegina SinagaNo ratings yet
- Recognition and Interpretation of Skin 1Document6 pagesRecognition and Interpretation of Skin 1Veterinarios de ArgentinaNo ratings yet
- Tissue Integrity Outline Spring 2023Document25 pagesTissue Integrity Outline Spring 2023morganstorey0No ratings yet
- Dr. Kurniati - Eliminating Dead Skin Cell Face and Body 0kt 2022Document27 pagesDr. Kurniati - Eliminating Dead Skin Cell Face and Body 0kt 2022wiwinNo ratings yet
- 08.16.16 Skin Histo Pathol (Nanney) HandoutDocument14 pages08.16.16 Skin Histo Pathol (Nanney) HandoutDan WuiytNo ratings yet
- Laporan Pendahuluan Asuhan Keperawatan Skin Loss A. PengertianDocument9 pagesLaporan Pendahuluan Asuhan Keperawatan Skin Loss A. PengertianPrasetyo official.01No ratings yet
- Anatomi, Eflouresensi KulitDocument67 pagesAnatomi, Eflouresensi KulitWhydia Wedha SutedjaNo ratings yet
- B T (B) E F M AL R: Otulinum Oxin Otox TO Nhance Acial Acroesthetics: Iterature EviewDocument8 pagesB T (B) E F M AL R: Otulinum Oxin Otox TO Nhance Acial Acroesthetics: Iterature EviewAnderson AraujoNo ratings yet
- Boli de PieleDocument44 pagesBoli de PieleAndreea CiaușuNo ratings yet
- Dr. Igwe DISEASE OF THE SKIN - Doc-1Document11 pagesDr. Igwe DISEASE OF THE SKIN - Doc-1Jake MillerNo ratings yet
- Anti Decubitus Air Pump For Air Mattress SystemDocument7 pagesAnti Decubitus Air Pump For Air Mattress SystemInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Anatomy of Wound Repair: Key Practice PointsDocument5 pagesAnatomy of Wound Repair: Key Practice PointsFofiuNo ratings yet
- Wound HealingDocument32 pagesWound Healingtepat rshsNo ratings yet
- A Case of Urticaria PigmentosaDocument3 pagesA Case of Urticaria PigmentosaRaisa SugoroNo ratings yet
- Unit # 06 Skin Management Insta Husain.z.kmuDocument43 pagesUnit # 06 Skin Management Insta Husain.z.kmuAamir IqbalNo ratings yet
- Terminologi Lesi KulitDocument4 pagesTerminologi Lesi KulitMariyatul QibthiyyahNo ratings yet
- Sindroma KompartemenDocument8 pagesSindroma KompartemennurulNo ratings yet
- AnalizáisDocument28 pagesAnalizáisJuan David LopezNo ratings yet
- Integumentary System: Burns and Wounds Clinical Case Study: Degree Burn Depth in Dermal Layers Description ImageDocument6 pagesIntegumentary System: Burns and Wounds Clinical Case Study: Degree Burn Depth in Dermal Layers Description ImageGabrielitoNo ratings yet
- Clinical Review On Sensitive Skin History Epidemiology Pathogenesis and Management 2155 9554 1000453Document6 pagesClinical Review On Sensitive Skin History Epidemiology Pathogenesis and Management 2155 9554 1000453Ratih AriyaniNo ratings yet
- Toxic Epidermal Necrolysis: A Paradigm of Critical IllnessDocument10 pagesToxic Epidermal Necrolysis: A Paradigm of Critical IllnessViolett LiebeNo ratings yet
- 03 SitumDocument5 pages03 SitumTrần Huyền TrânNo ratings yet
- Common Cutaneous Disorders in ElderlyDocument6 pagesCommon Cutaneous Disorders in Elderlyirvinaldi9No ratings yet
- Group 1Document34 pagesGroup 1Justin MallariNo ratings yet
- An Overview On Transdermal Patch Past, Present and Future PerspectiveDocument17 pagesAn Overview On Transdermal Patch Past, Present and Future PerspectiveSantanu PalNo ratings yet
- Modul 1 (No: 1-3) Anggota KelompokDocument33 pagesModul 1 (No: 1-3) Anggota KelompokfrostedsurgeonNo ratings yet
- Fisiologi Proses Penyembuhan LukaDocument7 pagesFisiologi Proses Penyembuhan LukaMarniNo ratings yet
- Skin Local: PlastiesDocument14 pagesSkin Local: PlastiesAnonymous kdBDppigENo ratings yet
- Ijd 12629Document8 pagesIjd 12629Hamza RafiqNo ratings yet
- Student Council Organization Rules and Regulations: ST ND RD TH TH THDocument2 pagesStudent Council Organization Rules and Regulations: ST ND RD TH TH THGabrelle OgayonNo ratings yet
- La Verre Male Grooming - The Ultimate Guide To Hair Styling 1Document38 pagesLa Verre Male Grooming - The Ultimate Guide To Hair Styling 1Charlie WeirNo ratings yet
- Fringe by Nikhil Chawla Price List JAN 2023 PDFDocument4 pagesFringe by Nikhil Chawla Price List JAN 2023 PDFAtiksh ChawlaNo ratings yet
- Countries CrosswordDocument5 pagesCountries Crossworddafnis dafnisNo ratings yet
- Degree of Burns: CharacteristicsDocument2 pagesDegree of Burns: CharacteristicsAnu TripathiNo ratings yet
- SkinDocument38 pagesSkinrodelagapito100% (1)
- Skin Diseases and Conditions Among Students of A Medical College in Southern IndiaDocument9 pagesSkin Diseases and Conditions Among Students of A Medical College in Southern IndiaMuhammad Khairuna SyahPutraNo ratings yet
- AlopeciaDocument12 pagesAlopeciasonamNo ratings yet
- FB Posts CommentsDocument41 pagesFB Posts Commentsizhar babaNo ratings yet
- Clinical and Dermoscopic Features of Lichen Planus Pigmentosus in 37 Patients With Frontal Fibrosing AlopeciaDocument9 pagesClinical and Dermoscopic Features of Lichen Planus Pigmentosus in 37 Patients With Frontal Fibrosing AlopeciaMir LaieeqNo ratings yet
- June July Reuze LDocument4 pagesJune July Reuze LAnonymous qpIquN2No ratings yet
- Management of Client With Integumentary DisordersDocument97 pagesManagement of Client With Integumentary Disordersduday76100% (1)
- Yang2015 Pili TortiDocument3 pagesYang2015 Pili TortiErnawati HidayatNo ratings yet
- Describing People: AppearanceDocument1 pageDescribing People: AppearanceMilű MonteroNo ratings yet
- Health Promotion of Older Adult - PPT HandoutsDocument24 pagesHealth Promotion of Older Adult - PPT HandoutsShankar GanigNo ratings yet
- Love Toolkit Worksheets FinalDocument16 pagesLove Toolkit Worksheets FinalYeisi HernándezNo ratings yet
- Nu Skin Enterprises Philippines, LLCDocument18 pagesNu Skin Enterprises Philippines, LLCJoel Collado AdalinNo ratings yet
- Harga Emina NewDocument4 pagesHarga Emina NewZidni IlmaNo ratings yet
- Actividad 1 Modulo 2Document11 pagesActividad 1 Modulo 2Claudia carsonNo ratings yet
- Dermpath Cheat SheetDocument2 pagesDermpath Cheat SheetBob LoblawNo ratings yet
- Hair ProductsDocument16 pagesHair ProductsAicha HrnNo ratings yet
- Luka Thermal / Combustio / BurnDocument51 pagesLuka Thermal / Combustio / BurnPraty Dina MulyaNo ratings yet