You might also like
- 68th AACC Annual Scientific Meeting Abstract eBookFrom Everand68th AACC Annual Scientific Meeting Abstract eBookNo ratings yet
- De Novo Mutations in YWHAG Cause Early Onset EpilepsyDocument11 pagesDe Novo Mutations in YWHAG Cause Early Onset EpilepsyGiselle Costa Daniel HonoratoNo ratings yet
- A Structured Assessment of Motor Function and Behavior in Patients With Kleefstra SyndromeDocument9 pagesA Structured Assessment of Motor Function and Behavior in Patients With Kleefstra SyndromeLEONARDO DO AMARAL PANCIERANo ratings yet
- MR Findings in Leigh Syndrome With COX Deficiency and SURF-1 MutationsDocument6 pagesMR Findings in Leigh Syndrome With COX Deficiency and SURF-1 MutationsDrsandy SandyNo ratings yet
- Riley 2009Document9 pagesRiley 2009Fahrunnisa NurdinNo ratings yet
- New Genes Causing Hereditary Parkinson 'S Disease or ParkinsonismDocument11 pagesNew Genes Causing Hereditary Parkinson 'S Disease or ParkinsonismAngélicaNo ratings yet
- FTPDocument325 pagesFTPKim Chwin KhyeNo ratings yet
- NFNS Molecular EvidenceDocument4 pagesNFNS Molecular EvidenceAldunIdhunNo ratings yet
- Gim 201618Document8 pagesGim 201618Ioana PoterasNo ratings yet
- Duplication at Xq13.3-q21.1 With Syndromic Intellectual Disability, A Probable Role For The ATRX GeneDocument6 pagesDuplication at Xq13.3-q21.1 With Syndromic Intellectual Disability, A Probable Role For The ATRX GeneEyyup UctepeNo ratings yet
- Cariotipo X Fragil y 47, XXX PDFDocument6 pagesCariotipo X Fragil y 47, XXX PDFLìzeth RamìrezNo ratings yet
- SchizophreniaDocument6 pagesSchizophreniaМ.К. МариNo ratings yet
- HHS Public Access: XRCC1 Mutation Is Associated With PARP1 Hyperactivation andDocument25 pagesHHS Public Access: XRCC1 Mutation Is Associated With PARP1 Hyperactivation andThaís MesequeNo ratings yet
- Role For Hedgehog Signaling in Cranial-Suture Development and ObesityDocument9 pagesRole For Hedgehog Signaling in Cranial-Suture Development and ObesityDanny Alvarez FocacciNo ratings yet
- GENE VARIATIONS ASSOCIATED WITH OCDDocument6 pagesGENE VARIATIONS ASSOCIATED WITH OCDRavennaNo ratings yet
- Marinesco-Sjo Gren Syndrome - 2013Document5 pagesMarinesco-Sjo Gren Syndrome - 2013Irfan RazaNo ratings yet
- Journal of Child Neurology 2Document7 pagesJournal of Child Neurology 2NEUROLAB ESCALÓNNo ratings yet
- Ejhg 201324Document7 pagesEjhg 201324sssssNo ratings yet
- Letter To The Editor: Autism and GeneticsDocument2 pagesLetter To The Editor: Autism and GeneticsHarshit AmbeshNo ratings yet
- Migraña Con Aura: Una Mirada Molecular A Un Problema HereditarioDocument7 pagesMigraña Con Aura: Una Mirada Molecular A Un Problema Hereditariojucrf1218No ratings yet
- 2008 - StefanssonDocument6 pages2008 - StefanssonCarlosNo ratings yet
- Epilepsia EpicongressDocument245 pagesEpilepsia EpicongressВасилий КоптеловNo ratings yet
- Gen SchizopDocument11 pagesGen SchizopDewiakyuNo ratings yet
- Multi-Disciplinary Study of Smith-Magenis SyndromeDocument8 pagesMulti-Disciplinary Study of Smith-Magenis SyndromeAraNo ratings yet
- Burégio-Frota Et Al 2010Document5 pagesBurégio-Frota Et Al 2010dida_bispoNo ratings yet
- tmp1329 TMPDocument11 pagestmp1329 TMPFrontiersNo ratings yet
- 1428 FullDocument6 pages1428 FullErik ArturNo ratings yet
- ARB and PregnancySSDocument2 pagesARB and PregnancySSakhmadNo ratings yet
- Jiménez-PSEN1 2008Document4 pagesJiménez-PSEN1 2008Carles de Diego BoguñáNo ratings yet
- Genotype-Phenotype Correlation, and Phenotypic HeterogeneityDocument9 pagesGenotype-Phenotype Correlation, and Phenotypic Heterogeneitykorokoro12No ratings yet
- hubADdgnserotoninarchneur 61 8 1249Document5 pageshubADdgnserotoninarchneur 61 8 1249Fitri anaNo ratings yet
- Genetics and AlzheimersDocument15 pagesGenetics and AlzheimersSex & Gender Women's Health CollaborativeNo ratings yet
- Wang 1995 Sonographic Lenticulostriate Vasculopathy in InfantsDocument11 pagesWang 1995 Sonographic Lenticulostriate Vasculopathy in InfantsModou NianeNo ratings yet
- 2011 BakirciogluDocument13 pages2011 BakirciogluMestrado EducacaoNo ratings yet
- Molecular analysis shows no linkage between migraine with aura and chromosome 4 locus in Chilean familiesDocument7 pagesMolecular analysis shows no linkage between migraine with aura and chromosome 4 locus in Chilean familiesDannnis PNo ratings yet
- 8.kuechler Et Al 2015Document13 pages8.kuechler Et Al 2015MiaNo ratings yet
- 8.kuechler Et Al 2015Document13 pages8.kuechler Et Al 2015MiaNo ratings yet
- Journal Noonan SyndromeDocument7 pagesJournal Noonan SyndromeSheilla GiustiNo ratings yet
- Limb Mammary Syndrome: A New Genetic Disorder With Mammary Hypoplasia, Ectrodactyly, and Other Hand/Foot Anomalies Maps To Human Chromosome 3q27Document9 pagesLimb Mammary Syndrome: A New Genetic Disorder With Mammary Hypoplasia, Ectrodactyly, and Other Hand/Foot Anomalies Maps To Human Chromosome 3q27Jane LiuNo ratings yet
- Nob 30093Document7 pagesNob 30093Bilel Le ChevalierNo ratings yet
- Genome-Wide Association Study Implicates NDST3 in Schizophrenia and Bipolar DisorderDocument10 pagesGenome-Wide Association Study Implicates NDST3 in Schizophrenia and Bipolar Disordera aNo ratings yet
- Letter: Mutations in UBQLN2 Cause Dominant X-Linked Juvenile and Adult-Onset ALS and ALS/dementiaDocument7 pagesLetter: Mutations in UBQLN2 Cause Dominant X-Linked Juvenile and Adult-Onset ALS and ALS/dementiaGarzo ZardofskyNo ratings yet
- Epileptic Encephalopathies SYNGAP1Document7 pagesEpileptic Encephalopathies SYNGAP1Saya OtonashiNo ratings yet
- Epigenetic Diagnostics For Neuropsychiatric DisordersDocument3 pagesEpigenetic Diagnostics For Neuropsychiatric DisordersafpiovesanNo ratings yet
- Aicardi-Goutie'res Syndrome: Neuroradiologic Findings and Follow-UpDocument6 pagesAicardi-Goutie'res Syndrome: Neuroradiologic Findings and Follow-UpclaypotgoldNo ratings yet
- Gim 200269 ADocument5 pagesGim 200269 AfakeempireNo ratings yet
- Zehra Agha, Zafar Iqbal, Maleeha Azam, Maimoona Siddique, Marjolein H. Willemsen, Tjitske Kleefstra, Christiane Zweier, Nicole de Leeuw, Raheel Qamar, Hans Van BokhovenDocument6 pagesZehra Agha, Zafar Iqbal, Maleeha Azam, Maimoona Siddique, Marjolein H. Willemsen, Tjitske Kleefstra, Christiane Zweier, Nicole de Leeuw, Raheel Qamar, Hans Van BokhovenAli HaiderNo ratings yet
- Science 1997Document3 pagesScience 1997demmie1989No ratings yet
- Genetic and Constitutional Factors Are Major Contributors ToDocument9 pagesGenetic and Constitutional Factors Are Major Contributors ToFernandoCardonaNo ratings yet
- First HPSE2 Missense Mutation in Urofacial SyndromeDocument5 pagesFirst HPSE2 Missense Mutation in Urofacial SyndromeAmir Akram MasihNo ratings yet
- Ref 47 hasil291096-862829963C2173Aaid-ajmg173B2-0Document5 pagesRef 47 hasil291096-862829963C2173Aaid-ajmg173B2-0Fitri anaNo ratings yet
- Michael C O'DonovanDocument3 pagesMichael C O'DonovanFahrunnisa NurdinNo ratings yet
- Srinivasan 2016Document16 pagesSrinivasan 2016Zeljko TomljanovicNo ratings yet
- TMP 756 DDocument24 pagesTMP 756 DnithiananthiNo ratings yet
- Microduplication of xp22.31Document4 pagesMicroduplication of xp22.31Roberth SanchezNo ratings yet
- Clinical, Biological and Genetic Analysis of Anorchia in 26 BoysDocument5 pagesClinical, Biological and Genetic Analysis of Anorchia in 26 Boysarda_ccerNo ratings yet
- Juvenile Neuronal Ceroid Lipofuscinosis: Clinical Course and Genetic Studies in Spanish PatientsDocument11 pagesJuvenile Neuronal Ceroid Lipofuscinosis: Clinical Course and Genetic Studies in Spanish PatientsMaferNo ratings yet
- Angelman syndrome and Rett syndrome genetic linkDocument6 pagesAngelman syndrome and Rett syndrome genetic linkAkmal NugrahaNo ratings yet
- A de Novo FOXP1 Truncating Mutation in A Patient Originally Diagnosed As C SyndromeDocument6 pagesA de Novo FOXP1 Truncating Mutation in A Patient Originally Diagnosed As C SyndromebcdavilaNo ratings yet
- 4.kharbanda Et Al 2017Document6 pages4.kharbanda Et Al 2017MiaNo ratings yet
- 2016 - Analysis of Y-Chromosome STRs in Chile Confirms An Extensive Introgression of European Male Lineages in Urban PopulationsDocument5 pages2016 - Analysis of Y-Chromosome STRs in Chile Confirms An Extensive Introgression of European Male Lineages in Urban PopulationsDaniela TroncosoNo ratings yet
- Ejemplo Analisis Modal EspectralDocument46 pagesEjemplo Analisis Modal EspectralJORGE DE LA CRUZ GUTIERREZNo ratings yet
- 2019 Haplogroup GDocument948 pages2019 Haplogroup GKlaus MarklNo ratings yet
- Human Heredity Principles and Issues 11th Edition Cummings Solutions ManualDocument10 pagesHuman Heredity Principles and Issues 11th Edition Cummings Solutions Manualstacyperezbrstzpmgif100% (32)
- Anthropology Paper 1 Topic Wise Upsc Questions (1985-2018) Syllabus Previous Year QuestionsDocument31 pagesAnthropology Paper 1 Topic Wise Upsc Questions (1985-2018) Syllabus Previous Year QuestionsAnkitOhriNo ratings yet
- HItchhiker's ThumbDocument3 pagesHItchhiker's ThumbJuan Dela CruzNo ratings yet
- Mangas.-Bidireccional - REVBDocument10 pagesMangas.-Bidireccional - REVBDanilo Camac FloresNo ratings yet
- The Origin of The Pashtuns PathansDocument4 pagesThe Origin of The Pashtuns PathansTuri AhmedNo ratings yet
- 2019 Haplogroup FDocument17 pages2019 Haplogroup FKlaus MarklNo ratings yet
- Branches of Genetics: Classical to PsychiatricDocument3 pagesBranches of Genetics: Classical to Psychiatrickevin maravillaNo ratings yet
- Adolf Hitler S DNA Shows North African and Ashkenazi Jew AncestryDocument2 pagesAdolf Hitler S DNA Shows North African and Ashkenazi Jew AncestryNarcisa Rudnic100% (1)
- FactorsDocument22 pagesFactorsKim OpenaNo ratings yet
- Test Bank For Human Heredity Principles and Issues 11th EditionDocument36 pagesTest Bank For Human Heredity Principles and Issues 11th Editionoutborn.piste5ols3q100% (46)
- DPT AngkerDocument10 pagesDPT Angkeranton seleNo ratings yet
- Jadwal dan Rute Kereta Api Gapeka 2019Document12 pagesJadwal dan Rute Kereta Api Gapeka 2019Anggerago Pjl Pitoe Siji100% (1)
- Hla DR TypingDocument5 pagesHla DR TypingJackie De VriesNo ratings yet
- SssDocument2 pagesSssE narender nayakNo ratings yet
- Anthropology Pyq 1985 - 2022-17-57Document41 pagesAnthropology Pyq 1985 - 2022-17-57Sada PatilNo ratings yet
- 2019 Haplogroup TDocument35 pages2019 Haplogroup TKlaus MarklNo ratings yet
- Aay6826 Antonio SMDocument117 pagesAay6826 Antonio SMRichard BlandiniNo ratings yet
- Human Genetics Concepts and Applications 11th Edition Ricki Lewis Test BankDocument9 pagesHuman Genetics Concepts and Applications 11th Edition Ricki Lewis Test BankMichaelMorgandzkam100% (29)
- Syndactyly 1Document13 pagesSyndactyly 1AminullahNo ratings yet
- MSC Genetics Ref BooksDocument21 pagesMSC Genetics Ref Bookssk912220% (1)
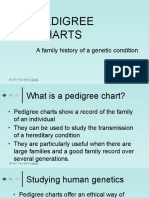
- Making A Pedigree ChartDocument15 pagesMaking A Pedigree ChartTylerNo ratings yet
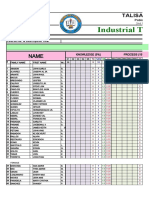
- SAY CITY COLLEGE TECHNOLOGY STUDENTS' PERFORMANCEDocument22 pagesSAY CITY COLLEGE TECHNOLOGY STUDENTS' PERFORMANCEAlther DabonNo ratings yet
- Arbins - R1B Haplogroup - KlyosovDocument19 pagesArbins - R1B Haplogroup - KlyosovRodrigo ArenasNo ratings yet
- Genome - A-mtDNA Haplogroup Analysis ReportDocument10 pagesGenome - A-mtDNA Haplogroup Analysis ReportsbzgtNo ratings yet
- 2Nd Year BS-MLT Course ContentsDocument13 pages2Nd Year BS-MLT Course ContentsAbdul RehmanNo ratings yet
- Full Download Human Genetics Concepts and Applications 12th Edition Lewis Test BankDocument6 pagesFull Download Human Genetics Concepts and Applications 12th Edition Lewis Test Bankwalmmidgetoin38o100% (41)
- Industrial Technology Program: Talisay City CollegeDocument22 pagesIndustrial Technology Program: Talisay City CollegeAlther DabonNo ratings yet