You might also like
- Your Electricity Bill at A Glance: Total Due 198.32Document2 pagesYour Electricity Bill at A Glance: Total Due 198.32rodrigo batistaNo ratings yet
- Fold N Slide Hardware BrochureDocument52 pagesFold N Slide Hardware Brochurecavgsi16vNo ratings yet
- Plasma Pen Fibroblast Eyes ContourDocument4 pagesPlasma Pen Fibroblast Eyes Contouralejandro Gonzàlez100% (1)
- University of Tennessee Religious ExemptionDocument3 pagesUniversity of Tennessee Religious ExemptionDonnaNo ratings yet
- Resolution of Pinguecula-Related Dry Eye Disease ADocument4 pagesResolution of Pinguecula-Related Dry Eye Disease ASylvia MtrianiNo ratings yet
- JurnalDocument8 pagesJurnalAnonymous fgRHAEIMrHNo ratings yet
- Miliariapustulosa in Post Craniotomy Patient: IOP Conference Series: Earth and Environmental ScienceDocument6 pagesMiliariapustulosa in Post Craniotomy Patient: IOP Conference Series: Earth and Environmental ScienceHanni HaeraniNo ratings yet
- Current Examination Methods of The Canine Eye: J. Beránek, P.J. VítDocument6 pagesCurrent Examination Methods of The Canine Eye: J. Beránek, P.J. VítOktavia firnandaNo ratings yet
- Corneal Edema Management With Ededay in Post CataractDocument12 pagesCorneal Edema Management With Ededay in Post CataractRamon Andres SrNo ratings yet
- Abstract Book PVSM2021 FinalDocument374 pagesAbstract Book PVSM2021 FinalnitaNo ratings yet
- Medicine: Sumatriptan-Induced Angle-Closure GlaucomaDocument4 pagesMedicine: Sumatriptan-Induced Angle-Closure GlaucomanidaNo ratings yet
- Progress in Retinal and Eye Research: Takashi Kojima, Murat Dogru, Motoko Kawashima, Shigeru Nakamura, Kazuo TsubotaDocument26 pagesProgress in Retinal and Eye Research: Takashi Kojima, Murat Dogru, Motoko Kawashima, Shigeru Nakamura, Kazuo TsubotaNoviani Rosa Sinensis HINo ratings yet
- Faure 2017Document8 pagesFaure 2017zazaza94No ratings yet
- GlaucomaDocument9 pagesGlaucomaREGINE YEO ZHI SHUENNo ratings yet
- Eur J Ophthalmol 2014 3 EJO-D-13-00288 299-308Document10 pagesEur J Ophthalmol 2014 3 EJO-D-13-00288 299-308idokurniawanNo ratings yet
- Evaluation of Umbilical Cord Serum Therapy in Acute Ocular Chemical BurnsDocument6 pagesEvaluation of Umbilical Cord Serum Therapy in Acute Ocular Chemical BurnsDebby Astasya AnnisaNo ratings yet
- Balanced Salt SolutionDocument36 pagesBalanced Salt Solutionnaili nsnNo ratings yet
- JurnalDocument18 pagesJurnalJean UsmanyNo ratings yet
- Trabecular Micro-Bypass Implant (Istent®) in A Case of Bilateral Acute Depigmentation of The IrisDocument4 pagesTrabecular Micro-Bypass Implant (Istent®) in A Case of Bilateral Acute Depigmentation of The IrisTainara BolsoniNo ratings yet
- MainDocument3 pagesMainomidazadmehr1375No ratings yet
- 2017 Ciliary Muscle Electrostimulation To Restore Accommodation in Patients With Early Presbyopia - Preliminary ResultsDocument8 pages2017 Ciliary Muscle Electrostimulation To Restore Accommodation in Patients With Early Presbyopia - Preliminary ResultsAlex KwanNo ratings yet
- TCRM 11 595Document9 pagesTCRM 11 595David LópezNo ratings yet
- Jurnal EED 4Document8 pagesJurnal EED 4Garsa GarnolNo ratings yet
- Orbital Infarction Syndrome Following Hyaluronic Acid Filler RhinoplastyDocument3 pagesOrbital Infarction Syndrome Following Hyaluronic Acid Filler RhinoplastyKerlida SantosNo ratings yet
- Case ReportDocument7 pagesCase ReportJeel GaralaNo ratings yet
- Jurnal MataDocument7 pagesJurnal MataRomi MaharNo ratings yet
- Randomized Clinical Trial of Topical Betaxolol For Persistent Macular Edema After Vitrectomy and Epiretinal Membrane RemovalDocument8 pagesRandomized Clinical Trial of Topical Betaxolol For Persistent Macular Edema After Vitrectomy and Epiretinal Membrane RemovalsiscaNo ratings yet
- Jurnal MataDocument11 pagesJurnal MataNovi RatnaNo ratings yet
- Corneal EdemaDocument9 pagesCorneal Edemazeeshan aliNo ratings yet
- Journal OphtalmologyDocument3 pagesJournal OphtalmologyFaza KeumalasariNo ratings yet
- Journal of Eucornea: K. Zonnevylle, D. Thoma, E. Mulliez, S. Ghekiere, J. Blanckaert, M.D.A. Blanckaert TDocument4 pagesJournal of Eucornea: K. Zonnevylle, D. Thoma, E. Mulliez, S. Ghekiere, J. Blanckaert, M.D.A. Blanckaert TKhalfiaNo ratings yet
- Lesión Química Ocular Asociada Con Desinfectante de Manos Una Mini Revisión Sobre Su Aumento Bajo COVID-19Document4 pagesLesión Química Ocular Asociada Con Desinfectante de Manos Una Mini Revisión Sobre Su Aumento Bajo COVID-19anolejaNo ratings yet
- Regaladofarreras 2014Document5 pagesRegaladofarreras 2014Leonardo AmaralNo ratings yet
- Five Year PROSE Treatment For Aniridic KojimaOct2016PAPDocument5 pagesFive Year PROSE Treatment For Aniridic KojimaOct2016PAP小島隆司No ratings yet
- Boston XODocument5 pagesBoston XOjuan diego RuizNo ratings yet
- Comparison of The Anti-Inflammatory Effects of Fluorometholone 0.1% Combined With Levofloxacin 0.5% and Tobramycin/dexamethasone Eye Drops After Cataract SurgeryDocument5 pagesComparison of The Anti-Inflammatory Effects of Fluorometholone 0.1% Combined With Levofloxacin 0.5% and Tobramycin/dexamethasone Eye Drops After Cataract Surgerybenefits35No ratings yet
- Oftalmologia Del ConejoDocument4 pagesOftalmologia Del ConejoRueca HelenciyaNo ratings yet
- Observations On Time Course Changes of The CherryDocument16 pagesObservations On Time Course Changes of The CherryAndi Tiara S. AdamNo ratings yet
- Bron 2017Document73 pagesBron 2017Anggia BungaNo ratings yet
- Nur Ulfah - Prevalence of Sign and Symptoms of Dry Eye After Refractive SurgeryDocument11 pagesNur Ulfah - Prevalence of Sign and Symptoms of Dry Eye After Refractive Surgerybudi haryadiNo ratings yet
- Eye Care Manajemen PDFDocument6 pagesEye Care Manajemen PDFKiki dwi PratiwiNo ratings yet
- Opth 4 203 PDFDocument7 pagesOpth 4 203 PDFDevanti EkaNo ratings yet
- Follicular Conjunctivitis in Dogs: A Retrospective Study (2007-2022)Document8 pagesFollicular Conjunctivitis in Dogs: A Retrospective Study (2007-2022)Akın SeverNo ratings yet
- Ocular Manifestation of Chlorpromazine Toxicity - ADocument3 pagesOcular Manifestation of Chlorpromazine Toxicity - AkamillaNo ratings yet
- DWDWQDocument10 pagesDWDWQprinceamitNo ratings yet
- JMedLife 05 82 PDFDocument3 pagesJMedLife 05 82 PDFYocha BangunNo ratings yet
- Tubercular Posterior SchleritisDocument6 pagesTubercular Posterior SchleritisInayatul muthmainnahNo ratings yet
- Lembaga KeuanganDocument4 pagesLembaga KeuanganReiny Laura NingrumNo ratings yet
- Tear Film, Contact Lens, and Patient-Related Factors Associated With Contact Lens-Related Dry EyeDocument10 pagesTear Film, Contact Lens, and Patient-Related Factors Associated With Contact Lens-Related Dry EyeAlda Gitu RahmaNo ratings yet
- OphtalmologyDocument7 pagesOphtalmologyZamir OanaNo ratings yet
- A Case of Atrophoderma Vermiculatum Responding ToDocument3 pagesA Case of Atrophoderma Vermiculatum Responding ToToivo ToivonenNo ratings yet
- Contact Lens & Anterior Eye: Keratoconus Presenting With Bilateral Simultaneous Acute Corneal HydropsDocument3 pagesContact Lens & Anterior Eye: Keratoconus Presenting With Bilateral Simultaneous Acute Corneal HydropsPungki Dio AzzawahaniNo ratings yet
- Glaucoma Case ReportDocument9 pagesGlaucoma Case Reportsuci caraswatiNo ratings yet
- b97c PDFDocument3 pagesb97c PDFintan rochmaharindaNo ratings yet
- Entropion 3 PDFDocument5 pagesEntropion 3 PDFdhitadwynNo ratings yet
- A Clinical Study On Visual Outcome and Complications of Penetrating KeratoplastyDocument12 pagesA Clinical Study On Visual Outcome and Complications of Penetrating KeratoplastyIOSRjournalNo ratings yet
- Effectiveness of Steroids Versus Immunomodulators Intreatment of Vernal Kerato-Conjunctivitis. A Study at Armed Forces Institute of OphthalmologyDocument4 pagesEffectiveness of Steroids Versus Immunomodulators Intreatment of Vernal Kerato-Conjunctivitis. A Study at Armed Forces Institute of OphthalmologyJimmy ChuaNo ratings yet
- Uveitic Glaucoma Management With Recurrent Uveitis EpisodeDocument6 pagesUveitic Glaucoma Management With Recurrent Uveitis EpisodeLina Shabrina QoribNo ratings yet
- Eyes That Look Down and Out A Case Series On Isolated Third Nerve PalsyDocument4 pagesEyes That Look Down and Out A Case Series On Isolated Third Nerve PalsyIJAR JOURNALNo ratings yet
- HHS Public Access: Role of Cataract Surgery in The Management of GlaucomaDocument13 pagesHHS Public Access: Role of Cataract Surgery in The Management of GlaucomaayuNo ratings yet
- Sravanthi Vegunta, BS, Dharmendra Patel, MD, and Joanne F. Shen, MDDocument6 pagesSravanthi Vegunta, BS, Dharmendra Patel, MD, and Joanne F. Shen, MDHabib Budiman AgungNo ratings yet
- Thesis Dry EyeDocument7 pagesThesis Dry Eyebsfp46eh100% (2)
- Proactive-And-reactive-practices-cabello Ma. Cristina & Cabillo Patrizia Ianne LDocument11 pagesProactive-And-reactive-practices-cabello Ma. Cristina & Cabillo Patrizia Ianne LcristinaNo ratings yet
- Food Photographs Practical Guidelines II Development and Use of Photographic Atlases For Assessing Food Portion SizeDocument7 pagesFood Photographs Practical Guidelines II Development and Use of Photographic Atlases For Assessing Food Portion SizemmmdeandradeNo ratings yet
- Formula and Functions in MS ExcelDocument9 pagesFormula and Functions in MS ExcelBhavana SangamNo ratings yet
- Kitimat JRP SummaryDocument17 pagesKitimat JRP SummaryNorthwest InstituteNo ratings yet
- TranscriptDocument1 pageTranscriptGursharanjit SinghNo ratings yet
- Finalizing The Accounting ProcessDocument2 pagesFinalizing The Accounting ProcessMilagro Del ValleNo ratings yet
- Tripwire Is An Intrusion Detection SystemDocument28 pagesTripwire Is An Intrusion Detection SystempoornimaNo ratings yet
- Digital ThermometerDocument28 pagesDigital ThermometerRajith SebastianNo ratings yet
- Citing SourcesDocument37 pagesCiting Sourcesasquared29No ratings yet
- 4 AMcKayCatalogDocument10 pages4 AMcKayCatalogManuelNo ratings yet
- Particulate Ow at The Mouth of The Soummam Watershed (Algeria)Document9 pagesParticulate Ow at The Mouth of The Soummam Watershed (Algeria)bougheraraNo ratings yet
- Activity Sheets Q1 - SVADocument5 pagesActivity Sheets Q1 - SVAAlma ReynaldoNo ratings yet
- Lesson 1 Exploring Indian LiteratureDocument5 pagesLesson 1 Exploring Indian LiteratureAthan MensalvasNo ratings yet
- User Manual: Series 7Document44 pagesUser Manual: Series 7Roniel ManjaresNo ratings yet
- HW1Document5 pagesHW1John SpartanNo ratings yet
- The Entheogen Review׃ Vol. 16, No. 1 (2008)Document44 pagesThe Entheogen Review׃ Vol. 16, No. 1 (2008)HoorayFrisbeeHead100% (2)
- Mobile Phone CloningDocument38 pagesMobile Phone CloningDevansh KumarNo ratings yet
- DLP L05 - Challenges in AdolescenceDocument3 pagesDLP L05 - Challenges in AdolescenceSora YamazakiNo ratings yet
- British Food Journal: Article InformationDocument8 pagesBritish Food Journal: Article InformationanisaNo ratings yet
- Construction ProjectsDocument13 pagesConstruction ProjectsMuhammad SafdarNo ratings yet
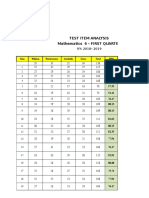
- Test Item Analysis Mathematics 6 - FIRST QUARTER: Item Wisdom Perseverance Gratitude Grace Total MPSDocument6 pagesTest Item Analysis Mathematics 6 - FIRST QUARTER: Item Wisdom Perseverance Gratitude Grace Total MPSQUISA O. LAONo ratings yet
- Digital SAT Skills Insight Tool - MathDocument61 pagesDigital SAT Skills Insight Tool - MathSianitus La Tour D'AuvergneNo ratings yet
- Agitated Thin Film Dryer ClaculationDocument12 pagesAgitated Thin Film Dryer ClaculationakaashNo ratings yet
- Coastal Suite For Tuba SoloDocument7 pagesCoastal Suite For Tuba SoloSusanna Payne-Passmore100% (1)
- Weekly Home Learning Plan - KindergartenDocument3 pagesWeekly Home Learning Plan - KindergartenPrecious ArniNo ratings yet
- RK20 Power Flow SparseDocument33 pagesRK20 Power Flow Sparsejohn smithNo ratings yet
- Councillor Danny Thorpe: Leader, Royal Borough of GreenwichDocument2 pagesCouncillor Danny Thorpe: Leader, Royal Borough of GreenwichDr-Syed Ali TarekNo ratings yet