You might also like
- TheLowCortisolLifestyle PDFDocument51 pagesTheLowCortisolLifestyle PDFthomas100% (2)
- A Systematic Approach To The Hip-Spine Relationship and Its Applications To Total Hip Arthroplasty - Eftekhary Et Al. 2019Document9 pagesA Systematic Approach To The Hip-Spine Relationship and Its Applications To Total Hip Arthroplasty - Eftekhary Et Al. 2019Mohammad KaramNo ratings yet
- Using The Brain (Not The Nose) To SmellDocument5 pagesUsing The Brain (Not The Nose) To SmellMorneNo ratings yet
- ENT EEE by Dr. Manisha Budhiraja 5th Edition - UnlockedDocument448 pagesENT EEE by Dr. Manisha Budhiraja 5th Edition - UnlockedArbin PanjaNo ratings yet
- Association Between Posture Voice Dysphonia ReviewDocument12 pagesAssociation Between Posture Voice Dysphonia ReviewChristaire AfariNo ratings yet
- A Review On Cosmetic Preparation of HairDocument8 pagesA Review On Cosmetic Preparation of HairEditor IJTSRDNo ratings yet
- Chapter 11: Parenteral Administration: Intradermal, Subcutaneous, and Intramuscular Routes Test BankDocument7 pagesChapter 11: Parenteral Administration: Intradermal, Subcutaneous, and Intramuscular Routes Test BankLuna TunaNo ratings yet
- META-Health Decoding Your Bodys Intelligence by Fisslinger, Johannes, RDocument196 pagesMETA-Health Decoding Your Bodys Intelligence by Fisslinger, Johannes, RTheo_96100% (2)
- Occlusal Vertical Dimension Treatment Planning Decisions and Management ConsiderationsDocument16 pagesOcclusal Vertical Dimension Treatment Planning Decisions and Management ConsiderationsHector Flores Soto100% (4)
- Tam1726834776305969 - RLS 4Document16 pagesTam1726834776305969 - RLS 4Rahul GNo ratings yet
- Non-Bone Graft Associated Regenerative Periodontal TherapyDocument80 pagesNon-Bone Graft Associated Regenerative Periodontal TherapyGorremuchu Srinivas0% (1)
- Hyoid Bone Position in Different Facial Skeletal PatternsDocument6 pagesHyoid Bone Position in Different Facial Skeletal PatternsVíctor Adolfo Ravelo SalinasNo ratings yet
- The Role of Intercondylar Distance in The Posterior Teeth ArrangementDocument5 pagesThe Role of Intercondylar Distance in The Posterior Teeth ArrangementBharath KondaveetiNo ratings yet
- Therapeutic Effects of Functional Orthodontic Appliances On Cervical Spine Posture: A Retrospective Cephalometric StudyDocument9 pagesTherapeutic Effects of Functional Orthodontic Appliances On Cervical Spine Posture: A Retrospective Cephalometric StudyJuliana ÁlvarezNo ratings yet
- Rocabado 1983Document7 pagesRocabado 1983Jessica PardoNo ratings yet
- Change of Hyoid Bone Position in Patients TreatedDocument18 pagesChange of Hyoid Bone Position in Patients TreatedYesenia PaisNo ratings yet
- Brachycephalic Dolichocephalic and Mesocephalic IsDocument6 pagesBrachycephalic Dolichocephalic and Mesocephalic IsDian PuspitaningtyasNo ratings yet
- Articulo Reading Report 1Document12 pagesArticulo Reading Report 1Caro RodriguezNo ratings yet
- Tooth Position in Wind Instrument Players: Dentofacial Cephalometric AnalysisDocument22 pagesTooth Position in Wind Instrument Players: Dentofacial Cephalometric AnalysisMauricio FemeniaNo ratings yet
- 0003-3219 (2004) 074 0361 Cotcba 2 0 Co 2Document6 pages0003-3219 (2004) 074 0361 Cotcba 2 0 Co 2Aly OsmanNo ratings yet
- Bjorl: Lambs' Temporal Bone Anatomy Under Didactic AspectsDocument7 pagesBjorl: Lambs' Temporal Bone Anatomy Under Didactic AspectsFairus ZainNo ratings yet
- Otolaryngol - Head Neck Surg - 2023 - Thuler - Transverse Maxillary Deficiency Predicts Increased Upper AirwayDocument10 pagesOtolaryngol - Head Neck Surg - 2023 - Thuler - Transverse Maxillary Deficiency Predicts Increased Upper AirwayMarco Saavedra BurgosNo ratings yet
- Vocal Fold Insuf Ficiency: Medialization Laryngoplasty Vs Calcium Hydroxylapatite Microspheres (Radiesse Voice)Document6 pagesVocal Fold Insuf Ficiency: Medialization Laryngoplasty Vs Calcium Hydroxylapatite Microspheres (Radiesse Voice)Dr. Hilder HernandezNo ratings yet
- Chin-Throat Anatomy: Normal Relations and Changes Following Orthognathic Surgery and Growth ModificationDocument7 pagesChin-Throat Anatomy: Normal Relations and Changes Following Orthognathic Surgery and Growth Modificationmehdi chahrourNo ratings yet
- Proposal of Measurement of Vertical Larynx Position at RestDocument5 pagesProposal of Measurement of Vertical Larynx Position at RestianekinNo ratings yet
- Examination of The Relationship Between Mandibular Position and Body PostureDocument14 pagesExamination of The Relationship Between Mandibular Position and Body PostureKiss KatalinNo ratings yet
- Comparison of Natural Head Position in Different Anteroposterior MalocclusionsDocument12 pagesComparison of Natural Head Position in Different Anteroposterior MalocclusionsRebin AliNo ratings yet
- Ferreira 2020Document10 pagesFerreira 2020Dela MedinaNo ratings yet
- Liu 2019Document7 pagesLiu 2019Aulia Siti NuraininNo ratings yet
- The Relationships Between Craniofacial Structure and Frontal Sinus Morphology: Evaluation With Conventional Anthropometry and CT-Based VolumetryDocument11 pagesThe Relationships Between Craniofacial Structure and Frontal Sinus Morphology: Evaluation With Conventional Anthropometry and CT-Based VolumetryfebriNo ratings yet
- Characteristics of Cervical Position Sense in Subjects With Forward Head PostureDocument3 pagesCharacteristics of Cervical Position Sense in Subjects With Forward Head PostureA AZIZNo ratings yet
- Relationships of Sagittal Skeletal Discrepancy, Natural Head Position, and Craniocervical Posture in Young Chinese ChildrenDocument7 pagesRelationships of Sagittal Skeletal Discrepancy, Natural Head Position, and Craniocervical Posture in Young Chinese ChildrenTanya HernandezNo ratings yet
- SefaloDocument6 pagesSefaloadisty maharaniNo ratings yet
- Reliability of Natural Head Position in Orthodontic Diagnosis: A Cephalometric StudyDocument4 pagesReliability of Natural Head Position in Orthodontic Diagnosis: A Cephalometric StudyAlvaro ChacónNo ratings yet
- Ce (Vsu) F (GH) Pf1 (Vsugh) Pfa (GH) Pf2 (Vsugh)Document5 pagesCe (Vsu) F (GH) Pf1 (Vsugh) Pfa (GH) Pf2 (Vsugh)miskica miskicaNo ratings yet
- Medscimonit 22 1637Document9 pagesMedscimonit 22 1637miskica miskicaNo ratings yet
- Comparative Study of Intermaxillary Relationships of Manual and Swallowing MethodsDocument7 pagesComparative Study of Intermaxillary Relationships of Manual and Swallowing MethodsdenisseNo ratings yet
- Reliability of Natural Head Position in Orthodontic Diagnosis: A Cephalometric StudyDocument4 pagesReliability of Natural Head Position in Orthodontic Diagnosis: A Cephalometric StudyAndrea Cárdenas SandovalNo ratings yet
- OPL & Hyoid BoneDocument7 pagesOPL & Hyoid BoneKanchit SuwanswadNo ratings yet
- Synopsis FormatDocument6 pagesSynopsis FormatAshok KumarNo ratings yet
- Revision Oclusion Dental y PosturaDocument6 pagesRevision Oclusion Dental y PosturaAlberto Jesús CamposNo ratings yet
- Morphometric Study of External Ear of MeDocument6 pagesMorphometric Study of External Ear of Meritee.shresthaNo ratings yet
- Bjorl: Cephalometric Evaluation of The Oropharyngeal Space in Children With Atypical DeglutitionDocument6 pagesBjorl: Cephalometric Evaluation of The Oropharyngeal Space in Children With Atypical DeglutitionJudith Alexandra Castro GaeteNo ratings yet
- ATT00183Document7 pagesATT00183Daniel VelezNo ratings yet
- Development of Prosthodontic Craniofacial StandardsDocument1 pageDevelopment of Prosthodontic Craniofacial StandardskerolossalahNo ratings yet
- Respiratory Swallow Pattern Following Total LaryngectomyDocument7 pagesRespiratory Swallow Pattern Following Total Laryngectomykhadidja BOUTOUILNo ratings yet
- Archives of Oral Biology: ArticleinfoDocument8 pagesArchives of Oral Biology: ArticleinfoMarwan El HelouNo ratings yet
- A Review of The Clinical Significance of The Occlusal Plane Variation and Head PostureDocument74 pagesA Review of The Clinical Significance of The Occlusal Plane Variation and Head PostureFaheemuddin MuhammadNo ratings yet
- Lenguaje y PaleoneurologiaDocument5 pagesLenguaje y PaleoneurologiasantiagoNo ratings yet
- Dimension VerticalDocument17 pagesDimension Verticalger moralesNo ratings yet
- Physiotherapeutic Treatment For Temporomandibular Disorders (TMD)Document6 pagesPhysiotherapeutic Treatment For Temporomandibular Disorders (TMD)israr_pt8880No ratings yet
- Evaluation of Mandibular First Molars' Axial Inclination and Alveolar Morphology in Different Facial Patterns: A CBCT StudyDocument10 pagesEvaluation of Mandibular First Molars' Axial Inclination and Alveolar Morphology in Different Facial Patterns: A CBCT StudyPututu PatataNo ratings yet
- Comparison of Airway Dimensions in Skeletal Class I PDFDocument8 pagesComparison of Airway Dimensions in Skeletal Class I PDFSoe San KyawNo ratings yet
- A Comparison of The Head and Cervical Posture Between The Self-Balanced Position and The Frankfurt MethodDocument8 pagesA Comparison of The Head and Cervical Posture Between The Self-Balanced Position and The Frankfurt MethodEvaristo Lillo VenegasNo ratings yet
- Susarla 2020Document8 pagesSusarla 2020MarcelaGutiérrezCarranzaNo ratings yet
- Mandibular Rest Position: A Reliable Position Influenced by Head Support and Body PostureDocument9 pagesMandibular Rest Position: A Reliable Position Influenced by Head Support and Body PostureKiss KatalinNo ratings yet
- Evaluation of Hyoid in Subject With Open BiteDocument11 pagesEvaluation of Hyoid in Subject With Open BiteSTEFANNY MERELONo ratings yet
- Natural Position of The Head Review of Two DimensionalDocument8 pagesNatural Position of The Head Review of Two DimensionalkerolossalahNo ratings yet
- Head Posture and Dental Wear Evaluation of Bruxist Children With Primary TeethDocument8 pagesHead Posture and Dental Wear Evaluation of Bruxist Children With Primary TeethEl GalenoNo ratings yet
- 21343-Article Text-67222-1-10-20181013Document6 pages21343-Article Text-67222-1-10-20181013Indah SuryadewiNo ratings yet
- Cervical Column Posture and Airway Dimensions in Clinical... 2013Document8 pagesCervical Column Posture and Airway Dimensions in Clinical... 2013Carlos Alberto Carranza LópezNo ratings yet
- Jkaoms 41 224Document8 pagesJkaoms 41 224SelvaNo ratings yet
- Cephalometric Evaluation of The Oropharyngeal Space in Children With Atypical DeglutitionDocument6 pagesCephalometric Evaluation of The Oropharyngeal Space in Children With Atypical DeglutitionGabriela MuñozNo ratings yet
- Aatika 5 PDFDocument8 pagesAatika 5 PDFAbhishek GuptaNo ratings yet
- A Cephalometric Study To Evaluate The Variations IDocument6 pagesA Cephalometric Study To Evaluate The Variations IjayashreeNo ratings yet
- Mouth Breathing and Facial Morphological PatternDocument6 pagesMouth Breathing and Facial Morphological PatternAlejandro RuizNo ratings yet
- MC NamaraDocument21 pagesMC NamaraGregoria choque floresNo ratings yet
- Clinical Result 61701Document1 pageClinical Result 61701Muhammad UzairNo ratings yet
- 01 Photo RecordsDocument1 page01 Photo RecordsMuhammad UzairNo ratings yet
- BiomechanicsDocument3 pagesBiomechanicsMuhammad UzairNo ratings yet
- Flapless CorticotomyDocument2 pagesFlapless CorticotomyMuhammad UzairNo ratings yet
- AnchorageDocument1 pageAnchorageMuhammad UzairNo ratings yet
- Eupatorium Leonardii - Brittonia 2012Document8 pagesEupatorium Leonardii - Brittonia 2012Richelle FigueroaNo ratings yet
- Beltran-Garcia2021 Article NitrogenFertilizationAndStressDocument12 pagesBeltran-Garcia2021 Article NitrogenFertilizationAndStressLALUKISNo ratings yet
- Class 12 Biology Chapter 14 NotesDocument23 pagesClass 12 Biology Chapter 14 NotesSyed Atta Ur RahmanNo ratings yet
- Comprehensive Antibiotic Resistance DatabaseDocument3 pagesComprehensive Antibiotic Resistance Databasemcdonald212No ratings yet
- JohnsonsDocument25 pagesJohnsonsshoba0880No ratings yet
- AP Biology Unit 7: Genetics Cheat Sheet: by ViaDocument1 pageAP Biology Unit 7: Genetics Cheat Sheet: by ViaJ15No ratings yet
- Nicart, Jeric-Vincent C. - Genetics LaboratoryDocument3 pagesNicart, Jeric-Vincent C. - Genetics Laboratoryebenicart0No ratings yet
- Evaluation of Antibacterial Activity of Leaf and Root Extracts of Sansevieria Zeylanica On UTI Among Students in University of Benin, Edo StateDocument8 pagesEvaluation of Antibacterial Activity of Leaf and Root Extracts of Sansevieria Zeylanica On UTI Among Students in University of Benin, Edo StateTunde EgunjobiNo ratings yet
- Worksheet Breathing and Exchange of GasesDocument2 pagesWorksheet Breathing and Exchange of GasesAakif RazaNo ratings yet
- Molecular-Docking Study of Malaria DrugDocument14 pagesMolecular-Docking Study of Malaria DrugJubairNo ratings yet
- The National Museum: Aljohn M. Fajilagmago G12 - DeweyDocument6 pagesThe National Museum: Aljohn M. Fajilagmago G12 - Deweypreciousaragon042gmailcomNo ratings yet
- Ejhg 201324Document7 pagesEjhg 201324sssssNo ratings yet
- The Earth's OceansDocument31 pagesThe Earth's Oceansglenn plazaNo ratings yet
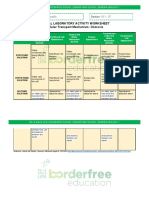
- Virtual Laboratory Worksheet-Cellular Transport MechanismDocument2 pagesVirtual Laboratory Worksheet-Cellular Transport MechanismKeizzhia Alleonah T. CastilloNo ratings yet
- Sample 10528Document16 pagesSample 10528Arham HaiderNo ratings yet
- IDOSER Efeito e Classificação Das Doses-1Document25 pagesIDOSER Efeito e Classificação Das Doses-1shimdiegoNo ratings yet
- Calendula 8Document7 pagesCalendula 8Zeila OmarNo ratings yet
- Art Integrated Project: Topic-GeneticsDocument10 pagesArt Integrated Project: Topic-GeneticsShifa SiddiquiNo ratings yet
- Organa Brands Dream TeamDocument3 pagesOrgana Brands Dream TeamMichael_Lee_RobertsNo ratings yet
- Gauk 1 Picture1 PDFDocument1 pageGauk 1 Picture1 PDFIshak Ika KovacNo ratings yet
- Researcher Lives Underwater MAXDocument4 pagesResearcher Lives Underwater MAXBrendaNo ratings yet
- Azoospermia ThesisDocument8 pagesAzoospermia ThesisBuyCustomPapersOnlineUK100% (2)