You might also like
- Topnotch Ent Supplement Handout Updated April 2016pdf PDFDocument15 pagesTopnotch Ent Supplement Handout Updated April 2016pdf PDFKenneth NuñezNo ratings yet
- Slots 2019 Periodontal Herpesvirus Morbidity and TreatmentDocument11 pagesSlots 2019 Periodontal Herpesvirus Morbidity and Treatmentmaria ocampoNo ratings yet
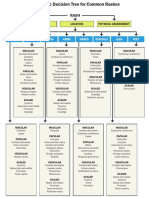
- WK 5 Rash Decision TreeDocument1 pageWK 5 Rash Decision TreeBetsy Brown ByersmithNo ratings yet
- Oral Manifestations of Viral Infections: CPD ArticleDocument4 pagesOral Manifestations of Viral Infections: CPD ArticleAlvionita AnggrainyNo ratings yet
- Oral Viral Infections Diagnosis and Management PDFDocument13 pagesOral Viral Infections Diagnosis and Management PDFWesley RodriguesNo ratings yet
- Integumen Viral InfectionDocument34 pagesIntegumen Viral InfectionNissa KeyssaNo ratings yet
- Oral Viral Infections Diagnosis and ManagementDocument13 pagesOral Viral Infections Diagnosis and ManagementhunarsandhuNo ratings yet
- Infections of The Oral MucosaDocument154 pagesInfections of The Oral MucosarizwanNo ratings yet
- Show Infetious Diseases IDocument18 pagesShow Infetious Diseases Iريام الموسويNo ratings yet
- Viral Infections: Presented By: Fatimah Zahraa Ahmed Supervised By: DR - RafilDocument31 pagesViral Infections: Presented By: Fatimah Zahraa Ahmed Supervised By: DR - Rafilfatimah zahraaNo ratings yet
- Herpes Simplex Type-1 Virus Infection (2003)Document16 pagesHerpes Simplex Type-1 Virus Infection (2003)Aron RonalNo ratings yet
- Oro-Facial Herpes Zoster: A Case Report With A Detailed Review of LiteratureDocument8 pagesOro-Facial Herpes Zoster: A Case Report With A Detailed Review of LiteratureTunggul BagusNo ratings yet
- Ulcerations of The Oral Cavity Infection Causing Oral UlcerationDocument17 pagesUlcerations of The Oral Cavity Infection Causing Oral UlcerationSebastian QuinteroNo ratings yet
- Herpes Zoster (Shingles) : Muhammad Abdullah Dept. of Dermatology DHQ Hospital FaisalabadDocument26 pagesHerpes Zoster (Shingles) : Muhammad Abdullah Dept. of Dermatology DHQ Hospital FaisalabadwaleedNo ratings yet
- Jurna Herpes Labialis 3Document3 pagesJurna Herpes Labialis 3Tifani Cita DewiNo ratings yet
- نور الهدى?Document16 pagesنور الهدى?nooraalhuda99No ratings yet
- Herpes Zoster Infection of Maxillary and Mandibular BranchpoDocument4 pagesHerpes Zoster Infection of Maxillary and Mandibular BranchpovikriNo ratings yet
- Oral Complications of Herpes Zoster Infection-Report of 3 CasesDocument4 pagesOral Complications of Herpes Zoster Infection-Report of 3 CasesAhmad HaikalNo ratings yet
- Primary Herpetic GingivostomatitisDocument5 pagesPrimary Herpetic GingivostomatitisGaleri Kreasi SepatukuNo ratings yet
- Ulcers and Vesicles2Document24 pagesUlcers and Vesicles2Kelly MayerNo ratings yet
- Jurnal Herpes PDFDocument9 pagesJurnal Herpes PDFIstianah EsNo ratings yet
- 4 Benign Infectious LesionsDocument5 pages4 Benign Infectious LesionsalbaablyNo ratings yet
- Herpes Zoster Ophthalmicus-Diagnosis and ManagementDocument6 pagesHerpes Zoster Ophthalmicus-Diagnosis and ManagementseptyneNo ratings yet
- SOFIA SALSABILA Rangkuman On ProgressDocument10 pagesSOFIA SALSABILA Rangkuman On ProgressSofia SalsabilaNo ratings yet
- Ulcerative Vesicular Bullous Lesions 1Document32 pagesUlcerative Vesicular Bullous Lesions 1Mustafa AliNo ratings yet
- M13 - Dermatology - Chapter 6Document9 pagesM13 - Dermatology - Chapter 6Idham BaharudinNo ratings yet
- Sur Mucosal Lesions-207Document207 pagesSur Mucosal Lesions-207megahedhazeemNo ratings yet
- Herpes Simplex VirusesDocument17 pagesHerpes Simplex VirusesДенніс МонгатеNo ratings yet
- LalalaDocument4 pagesLalalanoreka azizahNo ratings yet
- Oral PathologyDocument18 pagesOral Pathologyمنتظر منشد دعاشNo ratings yet
- Internal Medicine - DermatologyDocument125 pagesInternal Medicine - DermatologySoleil DaddouNo ratings yet
- Varicella/Herpes Zoster: Communicable Disease Management ProtocolDocument5 pagesVaricella/Herpes Zoster: Communicable Disease Management Protocolyuliyanto.efendiNo ratings yet
- Viral Skin Infections: Verrucae ValgarusDocument14 pagesViral Skin Infections: Verrucae Valgarusمسلم هاشم منافNo ratings yet
- Lesi Multipel Akut (Infeksi Virus & Bakteri)Document19 pagesLesi Multipel Akut (Infeksi Virus & Bakteri)Icha AnviniNo ratings yet
- Topnotch ENT Supplement Handout - UPDATED April 2017Document15 pagesTopnotch ENT Supplement Handout - UPDATED April 2017Andrassy Twinkle AlineaNo ratings yet
- Verruca Vulgaris in A Non-Immunocompromised Patient: Case ReportDocument4 pagesVerruca Vulgaris in A Non-Immunocompromised Patient: Case ReportBryan Eliezer SitumorangNo ratings yet
- Herpes Zoster Ophthalmicus Review and Prevention: Andrew R. Davis, and John SheppardDocument6 pagesHerpes Zoster Ophthalmicus Review and Prevention: Andrew R. Davis, and John SheppardVincentius Michael WilliantoNo ratings yet
- Oral Diseases Associated With Human Herpes Viruses: Aetiology, Clinical Features, Diagnosis and ManagementDocument9 pagesOral Diseases Associated With Human Herpes Viruses: Aetiology, Clinical Features, Diagnosis and ManagementArif RifaiNo ratings yet
- Rosen's Emergency Medicine Concepts and Clinical PracticeDocument15 pagesRosen's Emergency Medicine Concepts and Clinical PracticeMusdal RahmatNo ratings yet
- 3 Focal Infection of Periodontal Origin 2019Document3 pages3 Focal Infection of Periodontal Origin 2019fhiraNo ratings yet
- Orofacial Viral Infections An UpdateDocument6 pagesOrofacial Viral Infections An UpdateAli RazaNo ratings yet
- Management of Acute Primary Herpetic Gingivo-Stomatitis in ChildrenDocument3 pagesManagement of Acute Primary Herpetic Gingivo-Stomatitis in ChildrenNindy PutriNo ratings yet
- Herpes SimplexDocument27 pagesHerpes SimplexHania KhanNo ratings yet
- Viral KeratitisDocument30 pagesViral KeratitisIbrahim HayatiNo ratings yet
- Herpes Zoster - StatPearls - NCBI BookshelfDocument6 pagesHerpes Zoster - StatPearls - NCBI BookshelfDhany karubuyNo ratings yet
- 33HSVRamaDocument5 pages33HSVRamaPriskilla RachmiyantiNo ratings yet
- Otolaryngologic Manifestations of HIV Infection: ReviewsDocument6 pagesOtolaryngologic Manifestations of HIV Infection: ReviewsSo NicNo ratings yet
- Ulcerative Vesicular Bullous Lesions 2Document30 pagesUlcerative Vesicular Bullous Lesions 2Mustafa AliNo ratings yet
- Clinical ManifesDocument7 pagesClinical ManifesAbd Halim Gazali HNo ratings yet
- Herpes ZosterDocument15 pagesHerpes ZosterNadia Desanti RachmatikaNo ratings yet
- Chickenpox: Varicella-Virus InfectionsDocument5 pagesChickenpox: Varicella-Virus InfectionsAjay Pal NattNo ratings yet
- Common Viral Infections in The Oral Cavity: 1. Acute Herpetic Gingivostomatitis DNA VirusDocument6 pagesCommon Viral Infections in The Oral Cavity: 1. Acute Herpetic Gingivostomatitis DNA VirusChristineMartinNo ratings yet
- Efektivitas Vaksin VaricellaDocument21 pagesEfektivitas Vaksin VaricellaSul FadlyNo ratings yet
- 12 Cutaneous ManifestationsDocument11 pages12 Cutaneous ManifestationsFirda AureliaNo ratings yet
- Herpesvirida E& Adenoviridae: By: MJ Briones Bsn-IiDocument93 pagesHerpesvirida E& Adenoviridae: By: MJ Briones Bsn-IiMj BrionesNo ratings yet
- Microbial Diseases of The Skin and EyesDocument29 pagesMicrobial Diseases of The Skin and EyesqueennieNo ratings yet
- Nassef2015 PDFDocument6 pagesNassef2015 PDFBilel DhaouadiNo ratings yet
- Viral InfectionsDocument103 pagesViral InfectionsAkash Anilkumar MaliniNo ratings yet
- Ch04oral MedicineDocument35 pagesCh04oral MedicineNaleena JosephNo ratings yet
- Clinically Relevant Mycoses: A Practical ApproachFrom EverandClinically Relevant Mycoses: A Practical ApproachElisabeth PresterlNo ratings yet
- JForensicSciMed2139-5480686 151326 PDFDocument5 pagesJForensicSciMed2139-5480686 151326 PDFNur Adha AtjoNo ratings yet
- J9 How Little We Know Herpes ZosterDocument4 pagesJ9 How Little We Know Herpes ZosterNur Adha AtjoNo ratings yet
- J6 Patrrn of Oral Cavity LesionDocument5 pagesJ6 Patrrn of Oral Cavity LesionNur Adha AtjoNo ratings yet
- J4 A Savoury Case Report of Drugs Induced Erytema MultiformeDocument4 pagesJ4 A Savoury Case Report of Drugs Induced Erytema MultiformeNur Adha AtjoNo ratings yet
- Neuralgia TrigeminalDocument5 pagesNeuralgia TrigeminalcantikarevieraNo ratings yet
- Essential Drugs 2013Document378 pagesEssential Drugs 2013Chedeng KumaNo ratings yet
- Transient Delayed Facial Nerve Palsy After Inferior Alveolar Nerve Block AnesthesiaDocument6 pagesTransient Delayed Facial Nerve Palsy After Inferior Alveolar Nerve Block AnesthesiaWilson WijayaNo ratings yet
- Varicella ZosterDocument62 pagesVaricella ZosterEzekiel ArtetaNo ratings yet
- Infectious DermatologyDocument206 pagesInfectious DermatologyAaron Christian Earl VillosoNo ratings yet
- Basic Complex HomeopathyDocument681 pagesBasic Complex Homeopathytanasedaniela100% (1)
- Oral Path 2 - Lecture 2 DFBDocument7 pagesOral Path 2 - Lecture 2 DFBJana Louise DesamitoNo ratings yet
- Nursing Council of Kenya: Course Summary Report Eunice Paul 109603Document1 pageNursing Council of Kenya: Course Summary Report Eunice Paul 109603Eunice Mueni paulNo ratings yet
- Atlas and Synopsis of Clinical DermatologyDocument1,146 pagesAtlas and Synopsis of Clinical DermatologyAnda Madalina Zaharia100% (6)
- Dermatology Lectures JRRMMCDocument10 pagesDermatology Lectures JRRMMCGi Em100% (1)
- Shu ACT 2Document4 pagesShu ACT 2John Daniel CapituloNo ratings yet
- ChickenpoxDocument5 pagesChickenpoxShan MunozNo ratings yet
- Acyclovir Drug Study WWW RNpedia ComDocument3 pagesAcyclovir Drug Study WWW RNpedia ComJanaica JuanNo ratings yet
- Meningitis in Children, Diagnosis and Treatment in Emergency PDFDocument11 pagesMeningitis in Children, Diagnosis and Treatment in Emergency PDFPaul Palmer Mamani FNo ratings yet
- Buzz Word Cheat Sheet (Derm)Document5 pagesBuzz Word Cheat Sheet (Derm)emilyjvaldez99No ratings yet
- Evaluating The Febrile Patient With A RashDocument8 pagesEvaluating The Febrile Patient With A RashhawkssensNo ratings yet
- Assessing The BreastfeedingDocument25 pagesAssessing The BreastfeedinghiwaNo ratings yet
- Kenalog-40 en PiDocument11 pagesKenalog-40 en PiTariqNo ratings yet
- Nursing Pathophysiology Study Guide Last Test (Test 5)Document53 pagesNursing Pathophysiology Study Guide Last Test (Test 5)rainbowunicorn25100% (1)
- Antiviral Therapy PDFDocument438 pagesAntiviral Therapy PDFYOUCEF DHIA ELHAK KOUAOUCINo ratings yet
- Dermatology 2010 2011Document28 pagesDermatology 2010 2011Qasim HaleimiNo ratings yet
- WHO Med Guide 3 EdnDocument58 pagesWHO Med Guide 3 Ednmsk5in100% (1)
- Herpesvirus Infections in ChildrenDocument23 pagesHerpesvirus Infections in ChildrenShafiq NezatNo ratings yet
- August 9, 2013 Strathmore TimesDocument32 pagesAugust 9, 2013 Strathmore TimesStrathmore TimesNo ratings yet
- Trigeminal Autonomic CephalgiasDocument15 pagesTrigeminal Autonomic Cephalgiasheni taridaNo ratings yet
- Eye Pain and DischargeDocument53 pagesEye Pain and DischargeJitendra ChaudharyNo ratings yet
- Written Part AlfavitikaDocument24 pagesWritten Part AlfavitikaShanna MitchellNo ratings yet
- Pathophysiology - Chicken Pox Paper PDFDocument6 pagesPathophysiology - Chicken Pox Paper PDFRhiannon MartinNo ratings yet