You might also like
- Test Bank For Egans Fundamentals of Respiratory Care 11th Edition by KacmarekDocument36 pagesTest Bank For Egans Fundamentals of Respiratory Care 11th Edition by Kacmareknuggetessayistypcu100% (48)
- Test Bank For Egans Fundamentals of Respiratory Care 10th Edition KacmarekDocument10 pagesTest Bank For Egans Fundamentals of Respiratory Care 10th Edition Kacmarekcanebrutalfniy66No ratings yet
- Test Bank For Egans Fundamentals of Respiratory Care 9th Edition Robert L WilkinsDocument9 pagesTest Bank For Egans Fundamentals of Respiratory Care 9th Edition Robert L Wilkinscanebrutalfniy66No ratings yet
- Test Bank For Egans Fundamentals of Respiratory Care 9th Edition Robert L WilkinsDocument9 pagesTest Bank For Egans Fundamentals of Respiratory Care 9th Edition Robert L WilkinsPeggy Gebhart100% (28)
- Test Bank For Egans Fundamentals of Respiratory Care 10th Edition KacmarekDocument36 pagesTest Bank For Egans Fundamentals of Respiratory Care 10th Edition Kacmareknuggetessayistypcu100% (45)
- Test Bank For Egans Fundamentals of Respiratory Care 11th Edition by KacmarekDocument24 pagesTest Bank For Egans Fundamentals of Respiratory Care 11th Edition by KacmarekMichaelHensleyomkra100% (52)
- Kacmarek: Egan's Fundamentals of Respiratory Care, 10th EditionDocument5 pagesKacmarek: Egan's Fundamentals of Respiratory Care, 10th EditionYappie YappieNo ratings yet
- Test Bank For Mosbys Pharmacy Technician 5th Edition Karen Davis Anthony GuerraDocument36 pagesTest Bank For Mosbys Pharmacy Technician 5th Edition Karen Davis Anthony Guerratrigraphlaudably.3i52id100% (42)
- Full Download Test Bank For Foundations of Respiratory Care 2nd Edition Wyka PDF Full ChapterDocument20 pagesFull Download Test Bank For Foundations of Respiratory Care 2nd Edition Wyka PDF Full Chapterhydatidzonal4zm7z100% (11)
- Full Download Test Bank For Mosbys Pharmacy Technician 5th Edition Karen Davis Anthony Guerra PDF Full ChapterDocument36 pagesFull Download Test Bank For Mosbys Pharmacy Technician 5th Edition Karen Davis Anthony Guerra PDF Full Chapternebnebillinoisfp5n100% (20)
- NIV - Past, Present and FutureDocument9 pagesNIV - Past, Present and FutureDejan ŽujovićNo ratings yet
- Mechanical Ventilators Past Present Future (Kackmarek)Document11 pagesMechanical Ventilators Past Present Future (Kackmarek)Loralie Evangeline Perez-MirandaNo ratings yet
- TUGAS Unit I Dan 2 Kedokteran GigiDocument11 pagesTUGAS Unit I Dan 2 Kedokteran GigiWildan MentalisNo ratings yet
- Test Bank For Foundations of Respiratory Care 2nd Edition WykaDocument24 pagesTest Bank For Foundations of Respiratory Care 2nd Edition WykaHarryWilliamscwjbo100% (47)
- Test Bank For Essentials of Sonography and Patient Care 2nd Edition CraigDocument5 pagesTest Bank For Essentials of Sonography and Patient Care 2nd Edition CraigvioletalmaegjNo ratings yet
- Flexible Bronchoscopy - Clin Chest Med 2018Document16 pagesFlexible Bronchoscopy - Clin Chest Med 2018MICHAEL AMARILLO CORREANo ratings yet
- Full Test Bank For Respiratory Care Anatomy and Physiology 3Rd Edition Beachey PDF Docx Full Chapter ChapterDocument36 pagesFull Test Bank For Respiratory Care Anatomy and Physiology 3Rd Edition Beachey PDF Docx Full Chapter Chapterpedagog.blocage.5iwtr100% (9)
- Penicillins and CephalosporinsFrom EverandPenicillins and CephalosporinsRobert B. MorinNo ratings yet
- Noninvasive VentilationDocument38 pagesNoninvasive VentilationPaoly PalmaNo ratings yet
- Early Evolution of NebulizerDocument7 pagesEarly Evolution of NebulizerXubair WajidNo ratings yet
- BAJA MCQsDocument1,201 pagesBAJA MCQsReuben DutiNo ratings yet
- Foundation of Nursing Practice Exam For Oxygenation and NutritionDocument20 pagesFoundation of Nursing Practice Exam For Oxygenation and NutritionJomarie BeltranNo ratings yet
- Lung Development Biological and Clinical Perspectives: Biochemistry and PhysiologyFrom EverandLung Development Biological and Clinical Perspectives: Biochemistry and PhysiologyPhilip FarrellNo ratings yet
- The History of CPRDocument19 pagesThe History of CPRJuan Carlos AlfaroNo ratings yet
- Kinns The Medical Assistant 13th Edition Proctor Test BankDocument35 pagesKinns The Medical Assistant 13th Edition Proctor Test Bankgilbertsantiago6b9w1100% (26)
- Full Download Test Bank For Respiratory Care Anatomy and Physiology 3rd Edition Beachey PDF Full ChapterDocument36 pagesFull Download Test Bank For Respiratory Care Anatomy and Physiology 3rd Edition Beachey PDF Full Chapterpuffaluminize.g6qt100% (17)
- Fiberoptic and Flexible Endoscopic-Aided TechniquesDocument51 pagesFiberoptic and Flexible Endoscopic-Aided TechniquesAgustin CuryNo ratings yet
- Test Bank For Mosbys Pharmacy Technician 5th Edition Karen Davis Anthony GuerraDocument12 pagesTest Bank For Mosbys Pharmacy Technician 5th Edition Karen Davis Anthony GuerrachokydeplorerbxeNo ratings yet
- NCM 103 Final ExamDocument10 pagesNCM 103 Final ExamRichmond LacadenNo ratings yet
- Dwnload Full Kinns The Medical Assistant 13th Edition Proctor Test Bank PDFDocument35 pagesDwnload Full Kinns The Medical Assistant 13th Edition Proctor Test Bank PDFkiniteuphuist.d3axd100% (10)
- Special Methods: Physical Techniques in Biological ResearchFrom EverandSpecial Methods: Physical Techniques in Biological ResearchWilliam L. NastukNo ratings yet
- Full Download Exploring Medical Language A Student Directed Approach 8th Edition Brooks Test BankDocument36 pagesFull Download Exploring Medical Language A Student Directed Approach 8th Edition Brooks Test Bankdamagegunroom.yt79n100% (34)
- Kinns The Medical Assistant 13th Edition Proctor Test BankDocument25 pagesKinns The Medical Assistant 13th Edition Proctor Test BankRuthWilsoncoejg100% (56)
- The British Journal O F SurgeryDocument2 pagesThe British Journal O F SurgerySAILINGAREDDY MKNo ratings yet
- Criminology Board Exam Q - ADocument28 pagesCriminology Board Exam Q - AFelix GatuslaoNo ratings yet
- Polygraphy Reivew QuestionsDocument8 pagesPolygraphy Reivew QuestionsDaphney Claire Pineda63% (8)
- Clinical Procedures For Medical Assistants 8th Edition Bonewit Test BankDocument36 pagesClinical Procedures For Medical Assistants 8th Edition Bonewit Test Bankbedwarfratitemmg4100% (20)
- The Healthcare Professional 2nd Edition Karin C Vanmeter Robert J Hubert Isbn 9780323320924 Isbn 9780323320948 Isbn 9780323320955 Isbn 9780323100281Document7 pagesThe Healthcare Professional 2nd Edition Karin C Vanmeter Robert J Hubert Isbn 9780323320924 Isbn 9780323320948 Isbn 9780323320955 Isbn 9780323100281Tammy Wright100% (37)
- New Protein Foods: Animal Protein SuppliesFrom EverandNew Protein Foods: Animal Protein SuppliesAaron M. AltschulNo ratings yet
- Test Bank For Building A Medical Vocabulary 7th Edition by LeonardDocument24 pagesTest Bank For Building A Medical Vocabulary 7th Edition by LeonardBrianFloydckyt100% (48)
- Respiration ReviewDocument4 pagesRespiration ReviewMarshallMcGoughNo ratings yet
- The Principles and Practice of Human PhysiologyFrom EverandThe Principles and Practice of Human PhysiologyO. G. EdholmNo ratings yet
- Full Download Test Bank For Essentials of Sonography and Patient Care 2nd Edition Craig PDF Full ChapterDocument36 pagesFull Download Test Bank For Essentials of Sonography and Patient Care 2nd Edition Craig PDF Full Chapteranalcitedonary46f2d100% (17)
- Miller 7th Ed Chapter I HistoryDocument35 pagesMiller 7th Ed Chapter I Historyjbahalkeh7570No ratings yet
- New and Updated Methods: Analytical Methods for Pesticides and Plant Growth Regulators, Vol. 10From EverandNew and Updated Methods: Analytical Methods for Pesticides and Plant Growth Regulators, Vol. 10No ratings yet
- Maquina Anestesia PDFDocument14 pagesMaquina Anestesia PDFLider GaleNo ratings yet
- NP1 Oxygenation PDFDocument21 pagesNP1 Oxygenation PDFLot RositNo ratings yet
- 2005 The Inhalation of Drugs, Advantages and ProblemsDocument16 pages2005 The Inhalation of Drugs, Advantages and ProblemsJessica Alejandra Pizarro MoralesNo ratings yet
- Direction: Read The Question Carefully and Choose The Letter of The Correct Answer. Encircle The Letter ofDocument5 pagesDirection: Read The Question Carefully and Choose The Letter of The Correct Answer. Encircle The Letter ofSarah Jane PescadorNo ratings yet
- General Practice Airways Group Reproduction Prohibited: Inhalation Therapy: An Historical ReviewDocument11 pagesGeneral Practice Airways Group Reproduction Prohibited: Inhalation Therapy: An Historical ReviewliadiafaridaNo ratings yet
- hhEF66 HTM PDFDocument354 pageshhEF66 HTM PDFJuan Diego De La Cruz MiñanoNo ratings yet
- Funda 2Document9 pagesFunda 2Alex OlivarNo ratings yet
- MY REVIEWER IN MAPEHDocument13 pagesMY REVIEWER IN MAPEHCarlandrei DeveraNo ratings yet
- Laryngoscopy - Its Past and Future: Canadian Anaesthetists? Society Journal June 2004Document6 pagesLaryngoscopy - Its Past and Future: Canadian Anaesthetists? Society Journal June 2004razihaikalNo ratings yet
- Test Bank For Introduction To Physical Therapy 4th Edition PagliaruloDocument36 pagesTest Bank For Introduction To Physical Therapy 4th Edition Pagliarulophlegmsopranom1vopg100% (55)
- Respiratory - 2 - WsDocument5 pagesRespiratory - 2 - WsRatna PuspitasariNo ratings yet
- Forensic 5 Module 1 DiodosDocument10 pagesForensic 5 Module 1 DiodosGivehart Mira BanlasanNo ratings yet
- Respiratory - 2 - Ws - Grade 8 Penabur - AnswerDocument6 pagesRespiratory - 2 - Ws - Grade 8 Penabur - AnswerRatna PuspitasariNo ratings yet
- Physical Science 1Document25 pagesPhysical Science 1EJ RamosNo ratings yet
- Syllabus PTSV3Document21 pagesSyllabus PTSV3Pablito Quispe RuizNo ratings yet
- 3 Manacsa&Tan 2012 Strong Republic SidetrackedDocument41 pages3 Manacsa&Tan 2012 Strong Republic SidetrackedGil Osila JaradalNo ratings yet
- READMEDocument3 pagesREADMERadu TimisNo ratings yet
- Amazon Invoice Books 4Document1 pageAmazon Invoice Books 4raghuveer9303No ratings yet
- Ce Brochure 20july16Document76 pagesCe Brochure 20july16Yogesh SharmaNo ratings yet
- Fujitsu Lifebook p1120 ManualDocument91 pagesFujitsu Lifebook p1120 Manualمحمد يحىNo ratings yet
- Climate Change Survivor GameDocument22 pagesClimate Change Survivor Game许凉发No ratings yet
- Unit 2 - Chapter 04 - Working With FormsDocument24 pagesUnit 2 - Chapter 04 - Working With FormsSnr Berel ShepherdNo ratings yet
- Consumer Behavior PP Chapter 4Document36 pagesConsumer Behavior PP Chapter 4tuongvyvyNo ratings yet
- Altered Ventilatory Function Assessment at Pamantasan ng CabuyaoDocument27 pagesAltered Ventilatory Function Assessment at Pamantasan ng Cabuyaomirai desuNo ratings yet
- Satisfaction ExtraDocument2 pagesSatisfaction ExtraFazir AzlanNo ratings yet
- ForwardMails PDFDocument7 pagesForwardMails PDFJesús Ramón Romero EusebioNo ratings yet
- NABARD Dairy Farming Project - PDF - Agriculture - Loans PDFDocument7 pagesNABARD Dairy Farming Project - PDF - Agriculture - Loans PDFshiba prasad panjaNo ratings yet
- Is Iso 2692-1992Document24 pagesIs Iso 2692-1992mwasicNo ratings yet
- Forecast Time Series-NotesDocument138 pagesForecast Time Series-NotesflorinNo ratings yet
- Hotel Engineering Facilities: A Case Study of Maintenance PerformanceDocument7 pagesHotel Engineering Facilities: A Case Study of Maintenance PerformanceHoh Pui KeiNo ratings yet
- Frequently Asked Questions About Ailunce HD1: Where Can Find HD1 Software & Firmware?Document5 pagesFrequently Asked Questions About Ailunce HD1: Where Can Find HD1 Software & Firmware?Eric Contra Color0% (1)
- 24.ratios, Rates and Proportions PDFDocument9 pages24.ratios, Rates and Proportions PDFMilsonNo ratings yet
- Addressable Fire Detection and Control Miniplex TranspondersDocument8 pagesAddressable Fire Detection and Control Miniplex TranspondersAfdhal SyahrullahNo ratings yet
- 2.2valves, Alarm - Ul Product IqDocument1 page2.2valves, Alarm - Ul Product Iqbhima irabattiNo ratings yet
- Financial ManagementDocument2 pagesFinancial ManagementSanna KazmiNo ratings yet
- Contemporary Issue in StrategyDocument13 pagesContemporary Issue in Strategypatrick wafulaNo ratings yet
- Ed Brown CatalogDocument44 pagesEd Brown CatalogssnvetNo ratings yet
- Sem Iii Sybcom Finacc Mang AccDocument6 pagesSem Iii Sybcom Finacc Mang AccKishori KumariNo ratings yet
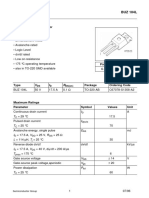
- Sipmos Power Transistor: BUZ 104LDocument10 pagesSipmos Power Transistor: BUZ 104LAlexsander MeloNo ratings yet
- Adms OneAdms One ClassDocument9 pagesAdms OneAdms One ClasssafwatNo ratings yet
- MaheshDocument20 pagesMaheshParthNo ratings yet
- MOW Procurement Management Plan - TemplateDocument7 pagesMOW Procurement Management Plan - TemplateDeepak RajanNo ratings yet
- IT-02 Residential StatusDocument26 pagesIT-02 Residential StatusAkshat GoyalNo ratings yet