You might also like
- Pregnancy Tests Explained (2Nd Edition): Current Trends of Antenatal TestsFrom EverandPregnancy Tests Explained (2Nd Edition): Current Trends of Antenatal TestsNo ratings yet
- Basics of Fetal EchocardiographyDocument58 pagesBasics of Fetal Echocardiographyrk vNo ratings yet
- Imaging of Gynecological Disorders in Infants and ChildrenFrom EverandImaging of Gynecological Disorders in Infants and ChildrenGurdeep S. MannNo ratings yet
- First-Trimester Maternal Ophthalmic Artery Doppler Analysis For Prediction of Pre-EclampsiaDocument8 pagesFirst-Trimester Maternal Ophthalmic Artery Doppler Analysis For Prediction of Pre-EclampsiaTopan AzzuriniNo ratings yet
- Vol9 Issue1 06Document4 pagesVol9 Issue1 06annisaNo ratings yet
- Cancer in Frozen Embryo TransferDocument21 pagesCancer in Frozen Embryo Transferadnoctum18No ratings yet
- FullPIERS Paper-LancetDocument39 pagesFullPIERS Paper-LancetRyan SadonoNo ratings yet
- Second-Generation Antipsychotics and Pregnancy ComplicationsDocument9 pagesSecond-Generation Antipsychotics and Pregnancy ComplicationsDian Oktaria SafitriNo ratings yet
- Protocol Poojitha CompletedDocument15 pagesProtocol Poojitha CompletedPranav SNo ratings yet
- Ijerph 16 00315Document16 pagesIjerph 16 00315nurlatifahNo ratings yet
- Risk Factors of Pre-Eclampsia/Eclampsia and Its Adverse Outcomes in Low-And Middle-Income Countries: A WHO Secondary AnalysisDocument9 pagesRisk Factors of Pre-Eclampsia/Eclampsia and Its Adverse Outcomes in Low-And Middle-Income Countries: A WHO Secondary AnalysisPutri Nilam SariNo ratings yet
- Ijerph 16 00315Document16 pagesIjerph 16 00315nilamsaryNo ratings yet
- Zhang 2019Document9 pagesZhang 2019Maria José MendiolaNo ratings yet
- Nakimuli2016 Article TheBurdenOfMaternalMorbidityAnDocument8 pagesNakimuli2016 Article TheBurdenOfMaternalMorbidityAnPriscilla AdetiNo ratings yet
- Congenital Diaphragmatic Hernia (CDH) Information For Health ProfessionalsDocument5 pagesCongenital Diaphragmatic Hernia (CDH) Information For Health ProfessionalsMangku Liong GuanNo ratings yet
- Fetal Heart Defects and Measures of Cerebral Size: Objectives Study DesignDocument8 pagesFetal Heart Defects and Measures of Cerebral Size: Objectives Study DesignAdrian KhomanNo ratings yet
- Articol 1Document7 pagesArticol 1nistor97No ratings yet
- Fetal DistressDocument48 pagesFetal DistressMeangafo GraciaNo ratings yet
- GUias de Practica Clinica de Ecografias de 2do TrimestreDocument11 pagesGUias de Practica Clinica de Ecografias de 2do TrimestreRodrigo BenitezNo ratings yet
- AMJ-05-522 American JournalDocument12 pagesAMJ-05-522 American JournalIman NurulNo ratings yet
- Hypertensive Disorders of Pregnancy and AssociatedDocument10 pagesHypertensive Disorders of Pregnancy and AssociatedMedrechEditorialNo ratings yet
- Knowledge Level and Determinants of Neonatal Jaundice A Cross-Sectional Study in The Effutu Municipality of GhanaDocument10 pagesKnowledge Level and Determinants of Neonatal Jaundice A Cross-Sectional Study in The Effutu Municipality of GhananicloverNo ratings yet
- Profile and Outcome of Congenital Heart Disease in Buea South West Region of Cameroon A Cross Sectional StudyDocument6 pagesProfile and Outcome of Congenital Heart Disease in Buea South West Region of Cameroon A Cross Sectional StudyAthenaeum Scientific PublishersNo ratings yet
- 2016 Neonates FinalDocument91 pages2016 Neonates FinalherryNo ratings yet
- Intrapartum Fetal Heart Rate Monitoring - Overview - UpToDateDocument62 pagesIntrapartum Fetal Heart Rate Monitoring - Overview - UpToDateROzi BarriosNo ratings yet
- Prenatal Diagnosis - Principles of Diagnostic Procedures and Genetic CounselingDocument6 pagesPrenatal Diagnosis - Principles of Diagnostic Procedures and Genetic CounselingvineelainjetyNo ratings yet
- The World Health Organization Fetal Growth ChartsDocument36 pagesThe World Health Organization Fetal Growth ChartsAndri SistikaNo ratings yet
- 2004, Vol.31, Issues 1, Ultrasound in ObstetricsDocument213 pages2004, Vol.31, Issues 1, Ultrasound in ObstetricsFebrinata MahadikaNo ratings yet
- Sof MarkersDocument21 pagesSof MarkersHari NairNo ratings yet
- R. Irvian1Document5 pagesR. Irvian1Ermawati RohanaNo ratings yet
- Risk Factor For Sever Postpartum Hemorrhage A Case Control StudyDocument9 pagesRisk Factor For Sever Postpartum Hemorrhage A Case Control StudyAhmad SyaukatNo ratings yet
- RHL - WHO Recommendation On Routine Assessment of Fetal Well-Being On Labour Admission - 2018-06-26Document9 pagesRHL - WHO Recommendation On Routine Assessment of Fetal Well-Being On Labour Admission - 2018-06-26Andyana SabtisanNo ratings yet
- Prenatal Screening SOGCDocument13 pagesPrenatal Screening SOGCBrendaNo ratings yet
- Guidelines For Fetal EchocardiographyDocument21 pagesGuidelines For Fetal EchocardiographyEbenNo ratings yet
- Diagnosis and Management of Thyroid Disease During Pregnancy and Postpartum - ATADocument61 pagesDiagnosis and Management of Thyroid Disease During Pregnancy and Postpartum - ATAtabhsinghiNo ratings yet
- Guidelines of The American Thyroid Association PREGNANCY PDFDocument47 pagesGuidelines of The American Thyroid Association PREGNANCY PDFIqra AnugerahNo ratings yet
- Guidelines For The Interpretation of The Neonatal ElectrocardiogramDocument16 pagesGuidelines For The Interpretation of The Neonatal ElectrocardiogramccNo ratings yet
- Eroswr GWGRDocument12 pagesEroswr GWGRPrasetio Kristianto BudionoNo ratings yet
- Neonatal and Obstetric Risk Assessment (NORA) Pregnancy Cohort Study in SingaporeDocument7 pagesNeonatal and Obstetric Risk Assessment (NORA) Pregnancy Cohort Study in SingaporePremier PublishersNo ratings yet
- Maternal Outcome After Complete Uterine RuptureDocument20 pagesMaternal Outcome After Complete Uterine RuptureDitaAndiniNo ratings yet
- Pre Marital Testing GuidelineDocument82 pagesPre Marital Testing GuidelineWidelmark FarrelNo ratings yet
- BMJ f6398Document13 pagesBMJ f6398Luis Gerardo Pérez CastroNo ratings yet
- Feto-Maternal Outcomes in Hypertensive Disorders of Pregnancy in A Tertiary Care Hospital: A Retrospective StudyDocument7 pagesFeto-Maternal Outcomes in Hypertensive Disorders of Pregnancy in A Tertiary Care Hospital: A Retrospective StudyIJAR JOURNALNo ratings yet
- Alcohol Consumption and Binge Drinking in Early Pregnancy. A Cross-Sectional Study With Data From The Copenhagen Pregnancy CohortDocument10 pagesAlcohol Consumption and Binge Drinking in Early Pregnancy. A Cross-Sectional Study With Data From The Copenhagen Pregnancy CohortdyantikazhafiraNo ratings yet
- Berntsen Articulo 1Document22 pagesBerntsen Articulo 1angelNo ratings yet
- Journal ClubDocument45 pagesJournal ClubdrnonoNo ratings yet
- 2nd Journal - Andre Parmonangan Panjaitan - 013Document7 pages2nd Journal - Andre Parmonangan Panjaitan - 013Andre Parmonangan PanjaitanNo ratings yet
- A Retrospective Review of Newborn Screening For Congenital Hypothyroidism and Newborn Thyroid Disease at A Major Medical CenterDocument8 pagesA Retrospective Review of Newborn Screening For Congenital Hypothyroidism and Newborn Thyroid Disease at A Major Medical CenterJohn Paul Driz ViloriaNo ratings yet
- Maternal and Perinatal Complications of Severe Preeclampsia in Three Referral Hospitals in Yaoundé, CameroonDocument8 pagesMaternal and Perinatal Complications of Severe Preeclampsia in Three Referral Hospitals in Yaoundé, CameroonIke Istofani KNo ratings yet
- 9 JurnalDocument83 pages9 JurnalWanda AndiniNo ratings yet
- European Journal of Obstetrics & Gynecology and Reproductive BiologyDocument5 pagesEuropean Journal of Obstetrics & Gynecology and Reproductive BiologyGustina Maryanti MooyNo ratings yet
- 2022 - McIntyre - Global Prevalence CPDocument13 pages2022 - McIntyre - Global Prevalence CPFriendlymeNo ratings yet
- Heavy Prenatal Alcohol Exposure and Obstetric and Birth2023Document8 pagesHeavy Prenatal Alcohol Exposure and Obstetric and Birth2023pau.reccNo ratings yet
- Evidence-Based Guidelines For The Management of Abnormally Invasive Placenta Recommendations From The International PDFDocument16 pagesEvidence-Based Guidelines For The Management of Abnormally Invasive Placenta Recommendations From The International PDFErika GuerreroNo ratings yet
- 33873-Article Text-121761-1-10-20170831Document6 pages33873-Article Text-121761-1-10-20170831AnggaNo ratings yet
- IUFDDocument12 pagesIUFDPitut T. PuspitasariNo ratings yet
- BMJ Open 2011 Roberts PrevalenceDocument11 pagesBMJ Open 2011 Roberts PrevalenceSiqbal Karta AsmanaNo ratings yet
- Ijgo 12692Document10 pagesIjgo 12692Putri Sari DewiNo ratings yet
- 2020 State Wide Program To Reduce Preterm Birth WADocument18 pages2020 State Wide Program To Reduce Preterm Birth WAmadhuNo ratings yet
- Jamacardiology Tyrmi 2023 Oi 230025 1688580076.42703Document10 pagesJamacardiology Tyrmi 2023 Oi 230025 1688580076.42703Vidya SaraswatiNo ratings yet
- Front PageDocument5 pagesFront PageAnas AloyodanNo ratings yet
- Modules in Grade 12: Quarter 1 - Week 3 Academic Track - StemDocument23 pagesModules in Grade 12: Quarter 1 - Week 3 Academic Track - StemZenarose MirandaNo ratings yet
- Automatic Summarization of Youtube Video Transcription Text Using Term Frequency-Inverse Document FrequencyDocument9 pagesAutomatic Summarization of Youtube Video Transcription Text Using Term Frequency-Inverse Document FrequencyKarunya ChavanNo ratings yet
- Your Initial Task. Find Out What's in Me!Document6 pagesYour Initial Task. Find Out What's in Me!Earl MontecastroNo ratings yet
- STEP English (1-18) All Worksheets 2020Document134 pagesSTEP English (1-18) All Worksheets 2020Shema ZulfiqarNo ratings yet
- Essay On Education in IndiaDocument6 pagesEssay On Education in IndiaSümît DãsNo ratings yet
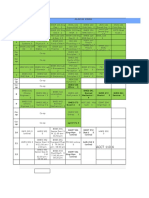
- BSMS Drexel ScheduleDocument4 pagesBSMS Drexel ScheduleAmy ZhiNo ratings yet
- Factura/Invoice: Et 1, Cernavoda, ConstantaDocument1 pageFactura/Invoice: Et 1, Cernavoda, ConstantaMadalina TibaNo ratings yet
- Kali Kaula A Manual of Tantric Magick HardbackDocument3 pagesKali Kaula A Manual of Tantric Magick Hardbackalintuta20% (1)
- Sachet MarketingDocument7 pagesSachet MarketingTom JohnNo ratings yet
- Offer and Acceptance:: Lapse of An OfferDocument12 pagesOffer and Acceptance:: Lapse of An OfferPriya AroraNo ratings yet
- Oslo Mihai Neacsu, IcpeDocument12 pagesOslo Mihai Neacsu, IcpeMihaiNeacsuNo ratings yet
- The Revenge of The SerpentDocument2 pagesThe Revenge of The SerpentMiyamoto MusashiNo ratings yet
- Ronald Allan Talisay CV 2017 - 1Document6 pagesRonald Allan Talisay CV 2017 - 1Ronald AllanNo ratings yet
- 2011 07 IDIP Unit A Past PaperDocument4 pages2011 07 IDIP Unit A Past Paperfh71No ratings yet
- Scribd Sap SD Pricing in Depth Configuration GuideDocument136 pagesScribd Sap SD Pricing in Depth Configuration GuideRavi SubramanianNo ratings yet
- BS 6089 - 2010 - Assessment of Insitu Compressive TestDocument40 pagesBS 6089 - 2010 - Assessment of Insitu Compressive TestMike Chan100% (2)
- Affordable HousingDocument12 pagesAffordable HousingTenzin KesangNo ratings yet
- Devesh ResumeDocument4 pagesDevesh ResumeNitinNo ratings yet
- PF2 S02-10 in Burning DawnDocument31 pagesPF2 S02-10 in Burning Dawnxajos85812No ratings yet
- MIS 310 - Syllabus 1.0Document12 pagesMIS 310 - Syllabus 1.0jackNo ratings yet
- The Igloo PartyDocument11 pagesThe Igloo PartyRaghav MalhotraNo ratings yet
- Industrial Development and Regulation ActDocument9 pagesIndustrial Development and Regulation ActNaveen DsouzaNo ratings yet
- Cut Pieces: From Flat Plates, Strips and Coil Stock. A. Shearing B. Bend Allowance C. Forming Dies D. Spring BackDocument100 pagesCut Pieces: From Flat Plates, Strips and Coil Stock. A. Shearing B. Bend Allowance C. Forming Dies D. Spring BackJade DigNo ratings yet
- Part 8 - Bibliography and ReferencesDocument31 pagesPart 8 - Bibliography and Referencessibhat mequanintNo ratings yet
- Solved Problems: Single Degree Free VibrationDocument14 pagesSolved Problems: Single Degree Free Vibrationprem adhikariNo ratings yet
- Taxation (Malawi) : Tuesday 4 June 2013Document10 pagesTaxation (Malawi) : Tuesday 4 June 2013angaNo ratings yet
- Service Manual: Diva Avr200 Surround Sound ReceiverDocument61 pagesService Manual: Diva Avr200 Surround Sound Receiver王军No ratings yet
- 1 Illinois Criminal Defense Motions - 9.14 2022-12-26 21 - 34 - 10 2Document4 pages1 Illinois Criminal Defense Motions - 9.14 2022-12-26 21 - 34 - 10 2Brandon SchrammNo ratings yet
- The Pros and Cons of GlobalizationDocument7 pagesThe Pros and Cons of Globalizationmaverick auburnNo ratings yet