You might also like
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5813)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Handbook of Placental Pathology, 2ndDocument343 pagesHandbook of Placental Pathology, 2ndpeuter100% (1)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Imumz Pitch DeckDocument20 pagesImumz Pitch DeckSanjay KumarNo ratings yet
- Framework For Maternal and Child Health NursingDocument26 pagesFramework For Maternal and Child Health NursingLeo Santos Magno75% (4)
- Legal Considerations of Maternal and Child PracticeDocument22 pagesLegal Considerations of Maternal and Child PracticeChari RivoNo ratings yet
- Dance Terms With Foreign Origin and Filipino Dance Terms Used in Filipino DancesDocument3 pagesDance Terms With Foreign Origin and Filipino Dance Terms Used in Filipino DancesHarvey Matbagan100% (1)
- Intimate Partner Violence Among Pregnant Women in Kenya: Forms, Perpetrators and AssociationsDocument25 pagesIntimate Partner Violence Among Pregnant Women in Kenya: Forms, Perpetrators and AssociationsNove Claire Labawan EnteNo ratings yet
- Science: Quarter 3 - Module 2Document16 pagesScience: Quarter 3 - Module 2Fernadez Rodison100% (3)
- Science: Quarter 3 - Module 2: Feedback Mechanisms Involved in The Regulating Processes of Menstrual CycleDocument26 pagesScience: Quarter 3 - Module 2: Feedback Mechanisms Involved in The Regulating Processes of Menstrual CycleViktor InocNo ratings yet
- Lesson Plan - ProstaglandinsDocument5 pagesLesson Plan - ProstaglandinsDelphy VargheseNo ratings yet
- Other Indication For CSDocument1 pageOther Indication For CSHarvey MatbaganNo ratings yet
- Study of Sociodemographic Profile, Maternal, Fetal Outcome in Preeclamptic and Eclamptic Women A Prospective StudyDocument6 pagesStudy of Sociodemographic Profile, Maternal, Fetal Outcome in Preeclamptic and Eclamptic Women A Prospective StudyHarvey MatbaganNo ratings yet
- High Rate of Early Onset Preeclampsia in MauritiusDocument4 pagesHigh Rate of Early Onset Preeclampsia in MauritiusHarvey MatbaganNo ratings yet
- 7 Properties of Curves: ObjectivesDocument42 pages7 Properties of Curves: ObjectivesHarvey MatbaganNo ratings yet
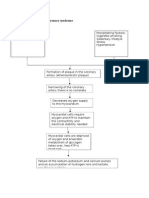
- Pathophysiology of Acute Coronary SyndromeDocument2 pagesPathophysiology of Acute Coronary SyndromeHarvey MatbaganNo ratings yet
- Loving and Caring Father Opening Prayer:: Luke 15: 11-32Document2 pagesLoving and Caring Father Opening Prayer:: Luke 15: 11-32Harvey MatbaganNo ratings yet
- R1Mc Internal Medicine Clerkship Rotation: Date Topics/Lectures Clerk Presenter ActivitiesDocument3 pagesR1Mc Internal Medicine Clerkship Rotation: Date Topics/Lectures Clerk Presenter ActivitiesHarvey MatbaganNo ratings yet
- (Type The Document Subtitle) : (Pick The Date) (Type The Company Name) Ka DomatDocument2 pages(Type The Document Subtitle) : (Pick The Date) (Type The Company Name) Ka DomatHarvey MatbaganNo ratings yet
- Modality of Learning Style: Unimodal MultimodalDocument1 pageModality of Learning Style: Unimodal MultimodalHarvey MatbaganNo ratings yet
- Generic Name: Classification: Muscular: Fine: SalbutamolDocument4 pagesGeneric Name: Classification: Muscular: Fine: SalbutamolHarvey MatbaganNo ratings yet
- NURS 1566 Clinical Form 3: Clinical Medications WorksheetsDocument1 pageNURS 1566 Clinical Form 3: Clinical Medications WorksheetsHarvey MatbaganNo ratings yet
- NURS 1566 Clinical Form 3: Clinical Medications WorksheetsDocument1 pageNURS 1566 Clinical Form 3: Clinical Medications WorksheetsHarvey MatbaganNo ratings yet
- Research QuestionsDocument1 pageResearch QuestionsHarvey MatbaganNo ratings yet
- Pathophysiology of Peyronie's DiseaseDocument7 pagesPathophysiology of Peyronie's DiseaseHarvey MatbaganNo ratings yet
- 100 Ways Not Ill-SHEEHANDocument0 pages100 Ways Not Ill-SHEEHANHarvey MatbaganNo ratings yet
- Format of The Family Nursing Care PlanDocument3 pagesFormat of The Family Nursing Care PlanHarvey MatbaganNo ratings yet
- FeverDocument7 pagesFeverHarvey MatbaganNo ratings yet
- NCPDocument6 pagesNCPHarvey MatbaganNo ratings yet
- Final Manu Sex EdDocument29 pagesFinal Manu Sex Eddee jayNo ratings yet
- Case Presentation-Severe Acute MalnutritionDocument29 pagesCase Presentation-Severe Acute Malnutritionroutc076No ratings yet
- Population Explosion-: Family Welfare ProgrammmeDocument15 pagesPopulation Explosion-: Family Welfare ProgrammmeAiyanNo ratings yet
- Day 1 UWORLD NOTESDocument6 pagesDay 1 UWORLD NOTESJohn DesirNo ratings yet
- NCM 109 AnswerDocument20 pagesNCM 109 AnswerBiway RegalaNo ratings yet
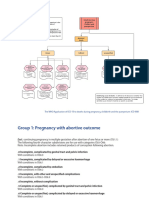
- Kompilasi - ICD MM Dan PM - Reference GuideDocument93 pagesKompilasi - ICD MM Dan PM - Reference GuidehijraNo ratings yet
- Filipino Culture, Values, and Practices in Relation To Difficult Childbearing and ChildrearingDocument8 pagesFilipino Culture, Values, and Practices in Relation To Difficult Childbearing and ChildrearingRheeanne AmilasanNo ratings yet
- Aromatherapy in Pregnancy: Written by Vicki Hobbs ©Document19 pagesAromatherapy in Pregnancy: Written by Vicki Hobbs ©Tama TaroNo ratings yet
- Husband's Role in Detecting Danger Signs of The Wife's Pregnancy Through The Husband's BookDocument6 pagesHusband's Role in Detecting Danger Signs of The Wife's Pregnancy Through The Husband's BookDewi Nopiska LilisNo ratings yet
- Screening and Diagnosis GDMDocument3 pagesScreening and Diagnosis GDMAkarapon SugandhanandaNo ratings yet
- Guideline No. 428 - Management of Dichorionic Twin PregnanciesDocument17 pagesGuideline No. 428 - Management of Dichorionic Twin PregnanciesSandra Díaz MercadoNo ratings yet
- Endometriosis Older Julia 1941 1st PBK Ed New York Annas ArchiveDocument244 pagesEndometriosis Older Julia 1941 1st PBK Ed New York Annas Archivenathanford1No ratings yet
- Jurnal Latihan Kegel ExcerciseDocument6 pagesJurnal Latihan Kegel ExcerciseIksan KhoironiNo ratings yet
- Perilaku Remaja Dan Kehamilan Remaja Di Desa Limakoli, Kabupaten Rote Ndao, Provinsi Nusa Tenggara Timur, IndonesiaDocument10 pagesPerilaku Remaja Dan Kehamilan Remaja Di Desa Limakoli, Kabupaten Rote Ndao, Provinsi Nusa Tenggara Timur, IndonesiaDera SukmanawatiNo ratings yet
- Anatomy and PhysiologyDocument1 pageAnatomy and PhysiologyFaharra VamentaNo ratings yet
- Knowledge Attitude and Practices of Health Workers On Puerperal Sepsis Preventions at Bundibugyo Hospital Bundibugyo DistrictDocument21 pagesKnowledge Attitude and Practices of Health Workers On Puerperal Sepsis Preventions at Bundibugyo Hospital Bundibugyo DistrictKIU PUBLICATION AND EXTENSIONNo ratings yet
- Notions About Child Birth (Natural Birth and Caesarian Section)Document2 pagesNotions About Child Birth (Natural Birth and Caesarian Section)Joseph UkamNo ratings yet
- Judicial AND Xtra Udicial Onfessions: Health LawDocument27 pagesJudicial AND Xtra Udicial Onfessions: Health LawPranavNo ratings yet
- What Is Culture EssayDocument6 pagesWhat Is Culture Essayfz6zke9m100% (2)
- Reproductive Health MindmapDocument11 pagesReproductive Health MindmapSuyagya PundirNo ratings yet
- Clinical Activities: A. Pre - ConsultationDocument13 pagesClinical Activities: A. Pre - ConsultationerykafadsNo ratings yet
- MCN MT 2Document19 pagesMCN MT 2Jekka Ann Dela CruzNo ratings yet