Professional Documents
Culture Documents
The Validity of Survivorship Analysis in Total.10
The Validity of Survivorship Analysis in Total.10
Uploaded by
yoel mitreOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
The Validity of Survivorship Analysis in Total.10
The Validity of Survivorship Analysis in Total.10
Uploaded by
yoel mitreCopyright:
Available Formats
( opynghi 959 by The Journal of Bone and Joint Surgerc, Incorporated
The Validity of Survivorship Analysis
Downloaded from http://journals.lww.com/jbjsjournal by BhDMf5ePHKav1zEoum1tQfN4a+kJLhEZgbsIHo4XMi0hC
in Total Joint Arthroplasty*
ywCX1AWnYQp/IlQrHD3i3D0OdRyi7TvSFl4Cf3VC1y0abggQZXdgGj2MwlZLeI= on 11/13/2023
BY FREDERICK DOREY, PH.D.t, AND HARLAN C. AMSTUTZ, M.D.t, LOS ANGELES, CALIFORNIA
/rom the Division of Orthopaedic Surgery. University of California, Los Angeles. School of Medicine, Los Angeles
ABSTRACT: The use of survivorship analysis re- tient’s status at the time of follow-up is unknown. According
quires an assumption that patients who are lost to follow- to follow-up procedures at the University of California at
up are no more or less likely to be at risk of failure of Los Angeles, patients who are lost to follow-up are those
an operation or a procedure than are patients who are who were due for a follow-up visit but who did not respond
still being followed. This is a major assumption in long- to a written request for a follow-up evaluation. This lack
term orthopaedic studies, in which a high percentage of of response may be due to factors that were not related to
patients are usually lost to follow-up. the status of the arthroplasty, such as the patient’s having
We compared the survivorship curve for the first relocated, having died, or having been dissatisfied with the
100 Tharies replacements done at our institution (which inconvenience of returning for follow-up examination.
were completed by September 1977), using data that The first long-term survivorship analysis for Tharies
were collected in the standard way up to 1985, through replacements was performed in 1985 and was based on all
a letter requesting a follow-up visit, with the curve for 585 patients who had had a Tharies replacement’. At that
the same patients that was based on almost complete time, a substantial number of patients were lost to follow-
follow-up data that were gathered by telephone from up, as is common in long-term orthopaedic studies com-
1985 on. The similarity of the two curves suggested that prising large numbers of patients. The usual method of
the assumptions that are necessary for the validity of survivorship analysis treats patients who are lost to follow-
survivorship analysis are reasonable, even in the ortho- up similarly to those who are still being followed and who
paedic setting, in which many patients are lost to follow- have not yet had a failed result. Both groups of patients are
up. referred to as being censored at the time of the most recent
The usefulness of the survivorship curve for pre- follow-up.
diction was also evaluated by comparing the curve based A major assumption of the survivorship analysis is that
on the first forty-six of the 100 Tharies replacements the mechanism of censorship is independent from the mech-
(before 1977) with the curve based on the last fifty-four anism of failure. This assumption becomes a problem if the
such operations (from January 1977 to September 1977). reason for the patient’s being lost to follow-up is related to
The results of these two comparisons suggest that the present status of the prosthesis.
survivorship analysis is a valid technique to use in the Another valid concern pertains to the use of the sur-
long-term evaluation of patients who have had a joint vivorship curve as a predictive tool. If such a curve does
replacement. not have some predictability for future implants in similar
patients under similar conditions, its use as an analytical
Survivorship analysis in the evaluation of total joint tool is limited.
arthroplasty has recently come into common use as an an- In this study, we used results of the first 100 Tharies
alytical technique, and it may soon be the preferred method replacements to investigate these concerns. We compared
of analysis of long-term clinical studies28. Of major con- the 1985 Kaplan-Meier survivorship curve7 (based on the
cern is the independent assumption that patients who are routine follow-up procedures at our institution, and hence-
lost to follow-up are no more or less likely to have had an forth referred to as the standard 1985 curve) with the 1985
operation that failed than are patients who are still being curve that would have been obtained ifthere had been almost
followed. complete follow-up data available for all patients (referred
A patient is considered to be lost to follow-up if he or to as the complete 1985 curve). In this comparison, we were
she missed the most recent follow-up visit, so that the pa- investigating the validity of the independence of the lost-
to-follow-up assumption.
* No benefits in any form have been received or will be received from In addition, in order to evaluate the predictive ability
a commercial party related directly or indirectly to the subject ofthis article.
No funds were received in support of this study.
of a survivorship curve, we compared the standard 1985
t Division of Orthopaedic Surgery. University of California, Los Kaplan-Meier curve, based on patients who had an operation
Angeles, School of Medicine, Center for the Health Sciences, 10833 Le
Conte Avenue, Los Angeles, California 90024-6902. Please address re-
before 1977, with the complete 1987 curve, based on pa-
quests for reprints to Dr. Dorey. tients who had an operation in 1977. In this second com-
544 ThE JOURNAL OF BONE AND JOINT SURGERY
VALIDITY OF SURVIVORSHIP ANALYSIS IN TOTAL JOINT ARTHROPLASTY 545
TABLE I
DATA ON THE FIRST ONE HUNDRED THARIES PROSTHES ES, IMPLANTED BE TWEEN JUNE 1975 AND SEPTEMBER 1977*
Total Pre-1977 1977
(N = 100) (N = 46) (N = 54)
Age (mean and standard deviation) (vrs.) 41 ± 15 42 ± 15 40 ± 15
Sex (percentage of men) 54 46 61
Downloaded from http://journals.lww.com/jbjsjournal by BhDMf5ePHKav1zEoum1tQfN4a+kJLhEZgbsIHo4XMi0hC
Etiology
Osteoarthritis 26 19 37
Osteonecrosis 21 19 23
ywCX1AWnYQp/IlQrHD3i3D0OdRyi7TvSFl4Cf3VC1y0abggQZXdgGj2MwlZLeI= on 11/13/2023
Congenital dislocation of the hip 16 21 12
Rheumatoid arthritis/juvenile 16 15 17
rheumatoid arthritis
Surgeon (percentage of H. C. A.) 72 78 68
* All variables except age are given as percentages.
parison, the usefulness of the survivorship curve as a prosthesis and had not been seen since 1984. This search
predictor of future results was assessed. consisted of reviewing the charts and using any available
information on patients, friends, and relatives that could be
Materials and Methods used for contacting the patients by telephone. Information
At the University of California, Los Angeles, the nor- on all subsequent operations for revision (our definition of
mal protocol for follow-up consists of return visits at six failure) was obtained by telephone. Because of the asso-
months; at one, two, and four years; and every one to four ciation of the Thames prosthesis with our institution, several
years thereafter, depending on the decision of the attending revision operations of University of California, Los An-
surgeon, which is based on the most recent evaluation of geles, patients that were performed by outside physicians
the patient. When a population of patients is to be analyzed, were reported directly to us, and no extra effort was needed
a letter requesting that a follow-up appointment be made is on our part. Using the time when the revision was done as
sent to patients for whom there is inadequate follow-up. our definition of time to failure, contact by telephone was
With this protocol, some patients who have not been seen adequate for obtaining complete follow-up information on
for the previous two to three years would still not be regarded these patients for the subsequent survivorship analysis.
as lost to follow-up ifthey had been seen at the most recently
Results
scheduled visit
and were not yet due for the next visit.
In June 1987, we initiated an extensive follow-up Assumption of Independence
search for the first 100 patients who had received a Tharies The first 100 Tharies prostheses were implanted be-
0
w
(I,
F-
0
z o-o”STANDARD” 1985 ANALYSIS
F-
z 29 REVISIONS
LU
0
.-. “COMPLETE” 1985 ANALYSIS
Li
0 41 REVISIONS
2 3 4 5 6 7 8 9
YEARS
TIME TO REViSION OF EITHER COMPONENT
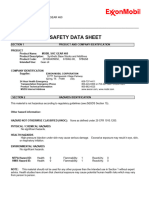
FIG. 1
Kaplan-Meier survivorship curve, based on the standard 1985 data, compared with the 1985 curve, based on almost complete data. This comparison
evaluates the assumption of independence that is necessary for the survivorship analysis to be valid.
VOL. 71-A, NO. 4, APRIL 1989
546 FREDERICK DOREY AND H. C. AMSTUTZ
TABLE II revisions that were known to have been performed by that
COMPARISON OF PATIENTS WHO HAD INCOMPLETE DATA WITH THOSE time, while actually there had been forty-one revisions by
WHO HAD COMPLETE DATA, BASED ON THE STANDARD 1985 ANALYSIS*
1985 . In addition, there was an average of three more years
Incomplete Complete of follow-up for the patients who had not yet had a failed
Data Data result. Despite the missing information, the standard 1985
(N=45) (N=55)
curve gives an accurate description of the survivorship of
Downloaded from http://journals.lww.com/jbjsjournal by BhDMf5ePHKav1zEoum1tQfN4a+kJLhEZgbsIHo4XMi0hC
Age (mean and standard deviation) (yrs.) 42 ± 16 40 ± 14 the prosthesis over time.
Weight (mean and standard deviation)(kg) 71 ± 12 69 ± 14
Sex (percentage of men) 67 42 Predictive Ability
ywCX1AWnYQp/IlQrHD3i3D0OdRyi7TvSFl4Cf3VC1y0abggQZXdgGj2MwlZLeI= on 11/13/2023
Surgeon (percentage of H. C. A.) 72 73
To assess the usefulness of the Kaplan-Meier curve in
Etiology
predicting results for future patients, we compared the stan-
Post-traumatic osteoarthntis 42 18
Avascular necrosis 16 25 dard 1985 Kaplan-Meier curve, based on the patients who
Congenital dislocation of the hip S 25 had had a Thames replacement before 1977, with the corn-
Rheumatoid arthritis 21 13
plete 1987 Kaplan-Meier curve, based on the patients who
* All variables except age and weight are given as percentages. had had the operation in 1977 (Fig. 2). Since the two groups
represent reasonably homogeneous populations, this corn-
tween June 1975 and September 1977. Table I is a summary parison could be made.
of the information on these patients. At the time of the 1985 While the first five years of the curves are not similar,
analysis, there had been twenty-nine revisions, but, more the long-term estimates are almost identical. Because the
importantly, only twenty-six of the seventy-one patients two populations are not identical in all variables, we did
who had not had a revision had been followed for at least not expect the curves to be identical. However, since the
eight years, even though all patients had a potential for eight populations are similar with respect to the more important
years of follow-up. Thus, for the 1985 analysis there was variables (Table I), we did expect the curves to be close,
complete eight-year information available on only 55 per which they are.
cent of the patients. These curves are based on samples that are about one-
Table II is a comparison of the characteristics of the half as large as those in Figure 1 , and due to the small size,
patients for whom complete data were available with those there is less precision in the estimates. The effect of the
of the remaining patients. The two populations had similar small size is illustrated by the fact that, although the esti-
characteristics, especially with respect to the important var- mates at three years are 84 and 98 per cent for the pre-1977
iables of age and weight. and 1977 curves, the 95 per cent confidence intervals for
Using the data that were collected in 1987, we were the true values overlap at these points in time. A statistical
able to recalculate what the 1985 curve would have been if analysis using the Mantel-Cox log-rank test to compare the
complete information had been available at that time. Figure two curves7 leads to the conclusion that the curves do not
1 shows a comparison of the ten-year Kaplan-Meier curve differ significantly from each other (p < 0. 147). These
that was based on the standard 1985 information with the curves could result from two random samples from the same
ten-year curve that was based on the complete 1985 data. underlying population of patients.
This comparison is summarized in Table III. The two curves
are almost identical, despite the fact that the 1985 curve Discussion
had complete eight-year data for 90 per cent of the patients, The current study provides encouraging evidence that
compared with only 55 per cent of the patients in the stan- the assumption of independence, which is necessary for the
dard 1985 analysis. Kaplan-Meier survivorship curve to be valid, is true. Thus,
The standard 1985 curve was based on the twenty-nine patients who are lost to follow-up are not at increased or
TABLE III
COMPARISON OF THE TEN-YEAR KAPLAN-MEIER CURVE BASED ON STANDARD 1985 DATA
WITH THE TEN-YEAR CURVE BASED ON COMPLETE 1985 DATA
Ten-Year
Kaplan-Meier Curve Ten-Year Curve
(Standard 1985 Data) (Complete 1985 Data)
Revisions (no.) 29 41
Patients who had not had a revision who had 26 49
follow-up of at least eight years (no.)
Mean duration of follow-up of patients 67.9 94.6
who had not had a revision (mos.)
Estimated rate of failure (per cent)
At five years 19 18
At nine years 46 41
ThE JOURNAL OF BONE AND JOINT SURGERY
VALIDITY OF SURVIVORSHIP ANALYSIS IN TOTAL JOINT ARTHROPLASTY 547
LU
Downloaded from http://journals.lww.com/jbjsjournal by BhDMf5ePHKav1zEoum1tQfN4a+kJLhEZgbsIHo4XMi0hC
o-0PRE 77 SURGERIES
F-
0
ywCX1AWnYQp/IlQrHD3i3D0OdRyi7TvSFl4Cf3VC1y0abggQZXdgGj2MwlZLeI= on 11/13/2023
z .-. 1977 SURGERIES
F-
z P = 0.114
LU
0
LU
0
1 2 3 4 5 6 7 8 9
YEARS
TIME TO REVISION OF EITHER COMPONENT
FIG. 2
Kaplan-Meier survivorship curves comparing the standard 1985 data for patients who had an operation before 1977 with the 1987 data for patients
who had an operation in 1977. This comparison evaluates the predictive value of a survivorship curve.
decreased risk of needing an operation for revision, com- equally, without regard to their clinical status. Finally, at
pared with those who return for follow-up evaluation. This the time of analysis, the characteristics of patients for whom
is important because in long-term orthopaedic studies, a the data are incomplete should be similar to those of patients
large percentage of patients is frequently lost to follow-up. for whom the data are complete. If these criteria are sat-
It is very time-consuming and expensive to keep track of isfied, we believe that our results justify the use of survi-
large numbers of patients. We have sometimes spent a total vorship analysis, even if a large percentage of patients has
of more than eight hours trying to contact only one patient. been lost to follow-up.
The problem of being lost to follow-up is not likely to be Our second comparison provides evidence of the use-
solved with better follow-up procedures, due to limitations fulness of the Kaplan-Meier curve in predicting results for
of time and cost. Also, if the assumption is true, the extra future patients. Considering the small size of the samples,
time and expense that are involved in tracking down patients we were encouraged by the long-term similarity of the two
who are lost to follow-up may not be justified for studies curves. The major reason for this similarity is the homo-
involving large numbers of patients. geneity of the patients in the two groups. We would not
A comparison should always be made, however, be- expect curves based on sixty to seventy-year-old patients to
tween the characteristics of patients who are lost to follow- provide any information on results for future patients in the
up and those of patients who are still being followed, in thirty to forty-year-old age bracket. Special care should be
order to evaluate whether there might be some bias in the taken, when comparing results in the literature, to ensure
former group. For example, the ages, etiologies, and di- that the groups that are being compared are similar with
agnoses at the time of operation should be similar for the regard to important prognostic variables, such as age, di-
two groups. If there is a difference, the assumption of in- agnosis, and level of activity, before reaching any conclu-
dependence should be questioned, and more effort should sions.
be made to at least make contact by telephone with a large Thus, while it is important to obtain as much up-to-
percentage of the missing patients, in order to verify if any date information on patients as possible, it does not seem
bias actually exists between the two groups. necessary to make an extraordinary effort in this direction
For the results that are presented here to be applicable in order to obtain valid survival curves. The designation of
to other medical centers, three criteria must be met. First, all patients who have not had a revision as censored seems
a continual effort must be made to follow all patients. Sec- to produce valid survival curves, which yield unbiased es-
ond, the follow-up effort should be applied to all patients timates of true curves.
References
1 . AMSTUTZ, H. C.; DOREY, FREDERICK; and O’CARROLL, P. F. : THARIES Resurfacing Arthroplasty. Evolution and Long-Term Results. Clin. Orthop.,
213: 92-114, 1986.
2. CORNELL, C. N. , and RANAWAT, C. S. : Survivorship Analysis of Total Hip Replacements. Results in a Series of Active Patients Who Were Less
than Fifty-five Years Old. J. Bone and Joint Surg. , 68-A: 1430-1434, Dec. 1986.
VOL. 71-A, NO. 4. APRIL 1989
548 FREDERICK DOREY AND H. C. AMSTUTZ
3. DOBBS, H. S.: Survivorship of Total Hip Replacements. J. Bone and Joint Surg. , 62-B(2): 168-173, 1980.
4. DOREY, F. , and AMSTUTZ, H. C. : Survivorship Analysis in the Evaluation of Joint Replacement. J. Arthroplasty, 1: 63-69, 1986.
5. JINNAH, R. H.; AMSTUTZ, H. C. ; TOOKE, S. M. : DOREY, FRED; and DALSETH, TERESA: The UCLA Chamley Experience: A Long-Term Follow-
up Study Using Survival Analysis. Clin. Orthop. . 211: 164-172, 1986.
6. KIM, W. C.; GROGAN, THOMAS: AMSTUTZ, H. C. ; and DOREY, FREDERICK: Survivorship Comparison ofTHARIES and Conventional Hip Arthroplasty
in Patients Younger than 40 Years Old. Clin. Orthop. , 214: 269-277, 1987.
7. LEE, E. 1. : Statistical Methods for Survival Data Analysis. Belmont, California, Lifetime Learning, 1980.
8. PAVLOV, P. W.: A 15-Year Follow-up Study of 512 Consecutive Charnley-Muller Total Hip Replacements. J. Arthroplasty, 2: 151-156, 1987.
Downloaded from http://journals.lww.com/jbjsjournal by BhDMf5ePHKav1zEoum1tQfN4a+kJLhEZgbsIHo4XMi0hC
ywCX1AWnYQp/IlQrHD3i3D0OdRyi7TvSFl4Cf3VC1y0abggQZXdgGj2MwlZLeI= on 11/13/2023
Copyright 1989 by The Journal of Bone and Joint Surgery. Incorporated
Management of Neuromuscular Spinal Deformities
with Luque Segmental Instrumentation*
BY OHENEBA BOACHIE-ADJEI, M.D.t, JOHN E. LONSTEIN, M.D4, ROBERT B. WINTER, M.D.,
STEVEN KOOP, M.D., KEITH VANDEN BRINK, M.D.I, AND FRANCIS DENIS, M.D., MINNEAPOLIS, MINNESOTA
From St. Paul and Fairview Riverside Hospitals. Minneapolis, and Gillette Children’s Hospital, St. Paul
ABSTRACT: Forty-six patients who had a neuro- rate of complications was 48 per cent. Pseudarthrosis
muscular spinal deformity were treated with arthrodesis occurred in three patients (6.5 per cent). There were no
and Luque segmental spinal instrumentation and were major neurological deficits related to the correction or
followed for an average of three years. Twenty-two pa- to the use of sublaminar wires. Three patients died, one
tients had cerebral palsy and twenty-four had another in the immediate postoperative period and the other two
neuromuscular disease. In thirty-nine patients, the ar- at eighteen months and four years after the original
throdesis was extended to the sacrum. Eleven patients procedure, due to causes unrelated to the operation.
who had severe scoliosis as well as pelvic obliquity and
decompensation of the torso had a combined anterior Patients who have a progressive or non-progressive
and posterior arthrodesis; the other thirty-five patients neuromuscular disorder are at high risk for the development
had a one-stage posterior procedure. Preoperatively, the of serious and devastating spinal deformity’3729. These pa-
average scoliosis was 74 degrees; this was corrected to tients have more complex problems than do patients who
39 degrees at follow-up. Final corrections were similar have idiopathic scoliosis. Spinal deformity, especially in a
for scoliosis and were better for pelvic obliquity and patient who has spastic cerebral palsy, is difficult to control
decompensation of the torso in patients who had com- with a brace, and it may progress even after skeletal maturity
bined anterior and posterior arthrodesis. The results for has been reached46’25. These patients also may have pelvic
scoliosis and pelvic obliquity in patients who had a spas- obliquity, dislocation of the hip, limited balance or ability
tic deformity were similar to the results in patients who to sit, back pain, and, in some circumstances, a serious
had a flaccid deformity. Correction of decompensation decrease in pulmonary function6”52022’2628’33. Treatment of
of the torso was better in patients who had a spastic spinal deformity secondary to neuromuscular disease pre-
deformity. sents a great challenge to the surgeon. Even with the advent
Postoperatively, a brace was used in half of the of newer surgical techniques, pertinent questions remain.
patients in each group; this did not appear to affect the Among these are: (1) Is Luque instrumentation appropriate
amount of correction in either group, although the result for a patient who has neuromuscular spinal deformity? (2)
may have been influenced by the selection process. The What is the role of the combination of anterior release and
posterior Luque instrumentation? (3) How predictable are
* No benefits in any form have been received or will be received from
a commercial party related directly or indirectly to the subject ofthis article.
correction of the curve and maintenance of correction in the
No funds were received in support of this study. various types of deformities? (4) Is external immobilization
t Twin Cities Scoliosis Center, Department of Orthopaedic Surgery,
University of Minnesota, 920 East 28th Street, Minneapolis, Minnesota
necessary after Luque instrumentation for neuromuscular
55407. Please address requests for reprints to Dr. Boachie-Adjei. scoliosis? (5) Is the Galveston technique reliable for ex-
:1: Minnesota Spine Center, Fairview Riverside Hospital, 2312 South
tending an ai-throdesis across the lumbosacral junction in a
Sixth Street, Minneapolis, Minnesota 55454.
§ Gillette Children’s Hospital, 200 University Avenue East, St. Paul, patient who has neuromuscular scoliosis?
Minnesota 55101.
The purpose of this paper is to review our experience
#{182}
Shnners Hospital for Crippled Children, 1900 Richmond Road,
Lexington, Kentucky 40502. with arthrodesis and Luque segmental spinal instrumentation
THE JOURNAL OF BONE AND JOINT SURGERY
You might also like
- Diabetic Foot CareDocument50 pagesDiabetic Foot CareaswiniNo ratings yet
- Air Optix Multi Focal Fitting GuideDocument2 pagesAir Optix Multi Focal Fitting Guidestrawberry88328100% (1)
- Bedside Ultrasound BookDocument274 pagesBedside Ultrasound Bookbilly thomas0% (1)
- NCP 2Document3 pagesNCP 2romelyn100% (1)
- First Lecture Intro BMEDocument32 pagesFirst Lecture Intro BMEAbdulwahab ThiabNo ratings yet
- Introduction To Bedside Ultrasound Volume 1 - Matt and MikeDocument274 pagesIntroduction To Bedside Ultrasound Volume 1 - Matt and MikeAnyaNo ratings yet
- Abscesso Cutâneo NEJMDocument9 pagesAbscesso Cutâneo NEJMJulio CesarNo ratings yet
- Does Total Knee Replacement Restore NormDocument9 pagesDoes Total Knee Replacement Restore NormSahithya MNo ratings yet
- Resistance After Selective Decontamination 𠄽ocument2 pagesResistance After Selective Decontamination –Kyomukama Racheal ClaireNo ratings yet
- Resultados de La Liberación Lateral Aislada en Inestabilidad Patelofemoral, Metanalisis 2019Document8 pagesResultados de La Liberación Lateral Aislada en Inestabilidad Patelofemoral, Metanalisis 2019Daniel Cancino CallirgosNo ratings yet
- Stability of Treatments For LuxationDocument4 pagesStability of Treatments For LuxationKeilin ChavezNo ratings yet
- The Perme Scale Score As A Predictor of Functional Status and Complications After Discharge From The Intensive Care Unit in Patients Undergoing Liver TransplantationDocument6 pagesThe Perme Scale Score As A Predictor of Functional Status and Complications After Discharge From The Intensive Care Unit in Patients Undergoing Liver TransplantationKaren MuñozNo ratings yet
- Main PDFDocument6 pagesMain PDFEdison HernandezNo ratings yet
- Assessment of Upper Extremity Function in Multiple SclerosisDocument7 pagesAssessment of Upper Extremity Function in Multiple Sclerosissarawu9911No ratings yet
- Assessment and Treatment of Children With Cerebral PalsyDocument13 pagesAssessment and Treatment of Children With Cerebral PalsyLizza Mora RNo ratings yet
- Postoperative Ileus: Cristina R. Harnsberger, MD Justin A. Maykel, MD Karim Alavi, MD, MPHDocument5 pagesPostoperative Ileus: Cristina R. Harnsberger, MD Justin A. Maykel, MD Karim Alavi, MD, MPHfatima chrystelle nuñalNo ratings yet
- Validation The Long Sitting Test On Subjects With Lliosacral DysfunctionDocument10 pagesValidation The Long Sitting Test On Subjects With Lliosacral Dysfunction黃郁庭No ratings yet
- Increasing Time To Operation Is Associated With Decreased Survival in Patients With A Positive FAST Examination Requiring Emergent LaparotomyDocument5 pagesIncreasing Time To Operation Is Associated With Decreased Survival in Patients With A Positive FAST Examination Requiring Emergent LaparotomyEvelyn GrandaNo ratings yet
- A Comparative Analysis of Functional and Patient RDocument6 pagesA Comparative Analysis of Functional and Patient RmirandaroydsNo ratings yet
- Yao2017 Article DoesLaparoscopicAdhesiolysisDeDocument8 pagesYao2017 Article DoesLaparoscopicAdhesiolysisDeInamullah FurqanNo ratings yet
- Current Approaches To Free Flap Monitoring: Albert H. Chao, MD Susan Lamp, BSN, RN, CPSNDocument5 pagesCurrent Approaches To Free Flap Monitoring: Albert H. Chao, MD Susan Lamp, BSN, RN, CPSNGuma KipaNo ratings yet
- 2020ICU - Icu 62 569Document8 pages2020ICU - Icu 62 569andryzell1987No ratings yet
- Amelar 1968Document12 pagesAmelar 1968Sexologia Del OesteNo ratings yet
- A Clinical Practice Guideline For The Use Of.6Document85 pagesA Clinical Practice Guideline For The Use Of.6LEONARDO ALEX CORROTEANo ratings yet
- Module 2 PDFDocument23 pagesModule 2 PDFRui ViegasNo ratings yet
- Revision Total Hip Arthroplasty For Instability: Surgical Techniques and PrinciplesDocument11 pagesRevision Total Hip Arthroplasty For Instability: Surgical Techniques and Principlesleidy-riverosNo ratings yet
- 2022 - Association Between Compliance With Enhanced Recovery After Surgery (ERAS) ProtocolsDocument13 pages2022 - Association Between Compliance With Enhanced Recovery After Surgery (ERAS) ProtocolsClarissa Simon FactumNo ratings yet
- Outcomes After Acute Versus Delayed Total Elbow ArDocument8 pagesOutcomes After Acute Versus Delayed Total Elbow ArLuis Guillermo Buitrago BuitragoNo ratings yet
- Systematic Review Rotationplasty-FULL PAPERDocument7 pagesSystematic Review Rotationplasty-FULL PAPERfhmanshoriNo ratings yet
- Eras SystectomyDocument9 pagesEras Systectomymehmet kabaaliNo ratings yet
- Examen Fisico RodillaDocument10 pagesExamen Fisico RodillaURGENCIAS HUSRTNo ratings yet
- 10 1053@j Jfas 2019 09 019Document7 pages10 1053@j Jfas 2019 09 019Han's OfficialNo ratings yet
- Selection of Patients For Through-The-Knee AmputationDocument6 pagesSelection of Patients For Through-The-Knee AmputationEGNo ratings yet
- 3 - Extended Focused Assessment With Sonography in TraumaDocument6 pages3 - Extended Focused Assessment With Sonography in TraumaMarcelo RibeiroNo ratings yet
- Criterion and Construct Validity of Prosthesis-IntDocument20 pagesCriterion and Construct Validity of Prosthesis-IntNada GhammemNo ratings yet
- The Fate of Patients Not Returning For Follow Up.2Document5 pagesThe Fate of Patients Not Returning For Follow Up.2yoel mitreNo ratings yet
- Early Versus Late Preventive Ileostomy Closure.21Document10 pagesEarly Versus Late Preventive Ileostomy Closure.21JOSENo ratings yet
- Implementation of A Urogynecology-Specific EnhancedDocument10 pagesImplementation of A Urogynecology-Specific EnhancedangelinputriNo ratings yet
- Luthringer 2019Document14 pagesLuthringer 2019Cristian Diaz KooNo ratings yet
- Functional Radiological Results and Quality of Life After Primary Total Hip ArthroplastyDocument7 pagesFunctional Radiological Results and Quality of Life After Primary Total Hip ArthroplastyAthenaeum Scientific PublishersNo ratings yet
- Errors in Strabismus SurgeryDocument5 pagesErrors in Strabismus SurgerySASNo ratings yet
- Articol ExtensoDocument5 pagesArticol ExtensoDavid CalinNo ratings yet
- Aob 21 208Document5 pagesAob 21 208MmdNo ratings yet
- Implantes en Pacientes Con RadioterapiaDocument7 pagesImplantes en Pacientes Con RadioterapiaLidise Hernandez AlonsoNo ratings yet
- 10 - Long-Term Outcome of Planovalgus Foot Surgical Correction in Children With Cerebral PalsyDocument7 pages10 - Long-Term Outcome of Planovalgus Foot Surgical Correction in Children With Cerebral PalsyJoe MehannaNo ratings yet
- Indications of Amputation After Limb-Salvage Surgery of Patients With Extremity-Located Bone and Soft-Tissue Sarcomas: A Retrospective Clinical StudyDocument5 pagesIndications of Amputation After Limb-Salvage Surgery of Patients With Extremity-Located Bone and Soft-Tissue Sarcomas: A Retrospective Clinical Studyrjs2w6xbbsNo ratings yet
- Development and Implementation of A Comprehensive Enhanced Recovery After Surgery Eras Protocol For Lumbar Spine Fusion The Singapore ExperienceDocument8 pagesDevelopment and Implementation of A Comprehensive Enhanced Recovery After Surgery Eras Protocol For Lumbar Spine Fusion The Singapore ExperienceHerald Scholarly Open AccessNo ratings yet
- Adaptive Equipnient Used in T E Rehabilitation of Hip Arthroplasty PatientsDocument6 pagesAdaptive Equipnient Used in T E Rehabilitation of Hip Arthroplasty PatientsMarina ENo ratings yet
- Arlen - 2016 - Outcomes of Complex Robot-AssistedDocument6 pagesArlen - 2016 - Outcomes of Complex Robot-AssistedAntonio López MolláNo ratings yet
- To Salvage (Routinely) or Not To Salvage: That Is The QuestionDocument4 pagesTo Salvage (Routinely) or Not To Salvage: That Is The QuestionEmman AmborNo ratings yet
- 50 Patients With OsteosarcomaDocument9 pages50 Patients With Osteosarcomarizaldy achmad kNo ratings yet
- Age-Based Outcomes of Cheilectomy For The Treatment of Hallux RigidusDocument6 pagesAge-Based Outcomes of Cheilectomy For The Treatment of Hallux RigidusmilenabogojevskaNo ratings yet
- Ijwh 6 829Document10 pagesIjwh 6 829noony 98No ratings yet
- A Clinical Practice Guideline For The Use of Ankle-Foot Orthoses and Functional Electrical Stimulation Post-StrokeDocument85 pagesA Clinical Practice Guideline For The Use of Ankle-Foot Orthoses and Functional Electrical Stimulation Post-Strokecamila hernandezNo ratings yet
- Enhanced Recovery After Surgery JournalDocument9 pagesEnhanced Recovery After Surgery JournalDea DickytaNo ratings yet
- Propensity Score-Matched Analysis of Enhanced Recovery After Surgery in Total Hip Arthroplasty For Displaced Femoral Neck FracturesDocument6 pagesPropensity Score-Matched Analysis of Enhanced Recovery After Surgery in Total Hip Arthroplasty For Displaced Femoral Neck FracturesVõ Văn Phúc ToànNo ratings yet
- Jarbo OJSM Lever TestDocument7 pagesJarbo OJSM Lever Testashlyn granthamNo ratings yet
- Outcomes of Surgery For Sacral Chordoma and Impact of Complications - A Report of 50Document11 pagesOutcomes of Surgery For Sacral Chordoma and Impact of Complications - A Report of 50Hugo JBNo ratings yet
- 10.7556 Jaoa.2012.112.12.775Document8 pages10.7556 Jaoa.2012.112.12.775Helena TregubovaNo ratings yet
- Plantar and Medial Heel Pain: Diagnosis and Management: Review ArticleDocument9 pagesPlantar and Medial Heel Pain: Diagnosis and Management: Review ArticleGhani AbdurahimNo ratings yet
- Fabio Febrian JurnalDocument3 pagesFabio Febrian JurnallarasatiNo ratings yet
- Physical Therapy in The Postoperative of Proximal Femur Fracture in Elderly. Literature ReviewDocument4 pagesPhysical Therapy in The Postoperative of Proximal Femur Fracture in Elderly. Literature ReviewEcsekiel MirandaNo ratings yet
- Koksal 2017Document1 pageKoksal 2017PaulHerreraNo ratings yet
- Atlas of Operative Procedures in Surgical OncologyFrom EverandAtlas of Operative Procedures in Surgical OncologyNo ratings yet
- Safety in Radiation OncologyDocument4 pagesSafety in Radiation Oncologyapi-711248154No ratings yet
- 8 The Affective Neuroscience Personality Scales: Normative Data and ImplicationsDocument14 pages8 The Affective Neuroscience Personality Scales: Normative Data and ImplicationsMaximiliano PortilloNo ratings yet
- Oleh: Heru Nurcahyo Magister Pendidikan Biologi Pps Uny 2019Document110 pagesOleh: Heru Nurcahyo Magister Pendidikan Biologi Pps Uny 2019RheaNo ratings yet
- C. Pasternatsky Symptom IsDocument11 pagesC. Pasternatsky Symptom IsareenNo ratings yet
- Jurnal Kepuasan Pengguna Aplikasi E-PpgbmDocument7 pagesJurnal Kepuasan Pengguna Aplikasi E-PpgbmkesmasseribuNo ratings yet
- Social Media: How Hospitals Use It, and Opportunities For Future UseDocument14 pagesSocial Media: How Hospitals Use It, and Opportunities For Future UseFaizaNadeemNo ratings yet
- Clinical Quiz 5Document1 pageClinical Quiz 5Samia RahmanNo ratings yet
- Children Under Juvenile Justice Intervention: A Case StudyDocument24 pagesChildren Under Juvenile Justice Intervention: A Case StudyMabhel Navarro GobNo ratings yet
- PIA Calabarzon 5 PRs (April 23, 2013), Dispatch For April 24, 2013 (Wednesday), 13 Photonews, 12 Weather Watch, 3 Regl - Watch, 2 OFW Watch, 16 Online NewsDocument29 pagesPIA Calabarzon 5 PRs (April 23, 2013), Dispatch For April 24, 2013 (Wednesday), 13 Photonews, 12 Weather Watch, 3 Regl - Watch, 2 OFW Watch, 16 Online NewsPia QuezonNo ratings yet
- Mobil SHC Gear 460Document9 pagesMobil SHC Gear 460kiranNo ratings yet
- UNIT-3 Gueridon ServiceDocument4 pagesUNIT-3 Gueridon ServiceOliver Hakim HadaouiNo ratings yet
- CRMTCS 6.docx LEGAL MEDDocument7 pagesCRMTCS 6.docx LEGAL MEDRendell EusebioNo ratings yet
- 4 CovidDocument47 pages4 CovidAbhishek toppoNo ratings yet
- 3103GF Halinski MichaelDocument6 pages3103GF Halinski MichaelrjjrerNo ratings yet
- NICUDocument68 pagesNICUdipali dhayagudeNo ratings yet
- Phadraig Et Al 2019 - Systematic DesensitizationDocument16 pagesPhadraig Et Al 2019 - Systematic DesensitizationCarlindo e CarlindoNo ratings yet
- Attach 03 - School Wins Monitoring Form - v. 2017.05.25Document6 pagesAttach 03 - School Wins Monitoring Form - v. 2017.05.25Emile Zamore100% (1)
- Configuration of Circle of Willis in Bangladeshi Population An Observational StudyDocument3 pagesConfiguration of Circle of Willis in Bangladeshi Population An Observational StudyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- The Cognitive Emotional and Social Sequlae of Stroke Psychological and Ethical Concern in Post Stroke AdaptationDocument11 pagesThe Cognitive Emotional and Social Sequlae of Stroke Psychological and Ethical Concern in Post Stroke AdaptationFahim Abrar KhanNo ratings yet
- JC Oncology55211005Document32 pagesJC Oncology55211005Neenuch ManeenuchNo ratings yet
- A Dangerous Method Film AnalysisDocument2 pagesA Dangerous Method Film AnalysisCleo-Jill TungolNo ratings yet
- Orthojournal V1issue1 04Document94 pagesOrthojournal V1issue1 04Yipno Wanhar El MawardiNo ratings yet
- Principle 3: Segment The Pleasure, Combine The PainDocument4 pagesPrinciple 3: Segment The Pleasure, Combine The PainMujtaba KhalilNo ratings yet
- Lecture 4 Urinary Data For K CalculationDocument29 pagesLecture 4 Urinary Data For K Calculationmahmoudnageh38No ratings yet
- IABP 11page CS100 Aog enDocument11 pagesIABP 11page CS100 Aog enRN333No ratings yet
- Junsay, Twinkle Mae D. Section A - Group 10 History #1Document15 pagesJunsay, Twinkle Mae D. Section A - Group 10 History #1Twinkle Mae JunsayNo ratings yet