You might also like
- 2 1 Flash Klasa 6 Mod 1b Test ExtendedDocument4 pages2 1 Flash Klasa 6 Mod 1b Test ExtendedMonika Ciepłuch-Jarema100% (1)
- Pharma Fluid and ElectrolytesDocument7 pagesPharma Fluid and ElectrolyteskristiannedenNo ratings yet
- Anaphy 03Document8 pagesAnaphy 03johannayao05No ratings yet
- Fluids and ElectrolytesDocument7 pagesFluids and ElectrolytesKarren FernandezNo ratings yet
- LL Transport Across Membrane Repaired Compatibility Mode 1Document5 pagesLL Transport Across Membrane Repaired Compatibility Mode 1Liana Rose MeregildoNo ratings yet
- CellDocument8 pagesCellVivaMapwaNo ratings yet
- TransportDocument56 pagesTransportPavan TummalaNo ratings yet
- Physio Mga TermsDocument6 pagesPhysio Mga TermsLei FernandezNo ratings yet
- Fluid Elec Trans PediaDocument9 pagesFluid Elec Trans PediayayayanizaNo ratings yet
- Cell TransportDocument38 pagesCell TransportCassandra DyNo ratings yet
- Lesson 4 Cellular TransportDocument25 pagesLesson 4 Cellular Transportyukuhamaru fenNo ratings yet
- Movement Across The Cell MembraneDocument43 pagesMovement Across The Cell MembraneanggaryanputraNo ratings yet
- Cell Membranes and TransportDocument32 pagesCell Membranes and TransportTobiNo ratings yet
- Cell TransportDocument24 pagesCell Transportbreadboi23100% (1)
- Cellular TransportDocument23 pagesCellular TransportMelvin Earl AgdaNo ratings yet
- Happ Lec Chapter 3Document9 pagesHapp Lec Chapter 3Raniel SilimNo ratings yet
- Body FluidDocument2 pagesBody FluidDiana YucosingNo ratings yet
- Cell Transport NotesDocument23 pagesCell Transport NotesxjoerenoxNo ratings yet
- Cellular Transport NotesDocument21 pagesCellular Transport NotesMCTCOLTDNo ratings yet
- Cell Membrane Transport PhysioDocument37 pagesCell Membrane Transport PhysioWandera GodfreyNo ratings yet
- Unit 3 BiologyDocument8 pagesUnit 3 BiologyChristine MoniqueNo ratings yet
- Cell Structure and FunctionsDocument10 pagesCell Structure and FunctionsQsh SinoroNo ratings yet
- Cellular TransportDocument26 pagesCellular TransportRara SorayaNo ratings yet
- NCM112 MS 1 Week 1Document11 pagesNCM112 MS 1 Week 1Lerry Claire LimosNo ratings yet
- Cell Transport Mechanisms: Passive and Active Transport Across MembranesDocument19 pagesCell Transport Mechanisms: Passive and Active Transport Across MembranesYSABEL VLOGS DANIELLENo ratings yet
- Cellular Transport MechanismsDocument49 pagesCellular Transport MechanismsSittie Amira G. ModawNo ratings yet
- Cell Transport NotesDocument24 pagesCell Transport Notesysablack1No ratings yet
- 17 - Fluid-Electrolyte-And-Acid-Base-Balance-Lledo-MontibonDocument14 pages17 - Fluid-Electrolyte-And-Acid-Base-Balance-Lledo-MontibonFranz Earl Niño Albesa100% (1)
- Cell Membrane and Cell Transport Notes NewDocument21 pagesCell Membrane and Cell Transport Notes NewEliezer Andres Gonzalez ChirinosNo ratings yet
- Transpor Membran Sel 2Document24 pagesTranspor Membran Sel 2Wisyam FebrianNo ratings yet
- Transport Mec Hanisms in Biological MembranesDocument51 pagesTransport Mec Hanisms in Biological Membranesjm earlytepNo ratings yet
- Cell Membrane Structure and Transport FunctionsDocument2 pagesCell Membrane Structure and Transport FunctionsCELLINA CLARISSE DE LEONNo ratings yet
- Cell Membrane Structure and Function: The Fluid Mosaic ModelDocument75 pagesCell Membrane Structure and Function: The Fluid Mosaic Modelvinay chaudhary100% (1)
- The Body Fluid Compartments & HomeostasisDocument7 pagesThe Body Fluid Compartments & HomeostasisEstellaNo ratings yet
- Fluid and Electrolyte Balance: Key Concepts for Maintaining HomeostasisDocument8 pagesFluid and Electrolyte Balance: Key Concepts for Maintaining Homeostasiskamae_070305No ratings yet
- Cell Membrane Structure and FunctionsDocument22 pagesCell Membrane Structure and FunctionsxCutex XwolfiechanXNo ratings yet
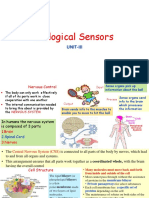
- Biological Sensors: Unit-IiiDocument64 pagesBiological Sensors: Unit-Iiiestraj1954No ratings yet
- 7 Transport-Mechanism2Document62 pages7 Transport-Mechanism2aldrin braganzaNo ratings yet
- Chapter 3 ReveiwerDocument8 pagesChapter 3 ReveiwerrizzamaegomezoctavianoNo ratings yet
- Cell Transport Types & ProcessesDocument41 pagesCell Transport Types & ProcessesBlace MontefalcoNo ratings yet
- Movement of Substance Across The MembraneDocument47 pagesMovement of Substance Across The MembranenoralizaaliNo ratings yet
- Still - Hillsong United With Lyrics - mp4Document79 pagesStill - Hillsong United With Lyrics - mp4Cenando BodanioNo ratings yet
- Cell Membranes: Osmosis and DiffusionDocument27 pagesCell Membranes: Osmosis and DiffusionFrita AnnisaNo ratings yet
- 1.3, 1.4 Cell Membrane and TransportDocument30 pages1.3, 1.4 Cell Membrane and TransportMaria MoronNo ratings yet
- NCM 112 - Fluids & Electrolytes: Homeostasis and Transport MechanismsDocument7 pagesNCM 112 - Fluids & Electrolytes: Homeostasis and Transport MechanismsMary Claire MasoNo ratings yet
- Movement of Substances Across The Plasma Membrane: Compiled & Prepared by Dsalleh (2021)Document25 pagesMovement of Substances Across The Plasma Membrane: Compiled & Prepared by Dsalleh (2021)Dewi SallehNo ratings yet
- Topic 1.4Document17 pagesTopic 1.4Fatima ZaidiNo ratings yet
- Transport MechanismDocument4 pagesTransport Mechanismbugaspearl0No ratings yet
- All Organisms and Their Cells Respond To External Conditions To Maintain A Stable Internal Condition. They Are MaintainingDocument54 pagesAll Organisms and Their Cells Respond To External Conditions To Maintain A Stable Internal Condition. They Are MaintainingKaylee Lopez Student - KnightdaleHSNo ratings yet
- Fluids and Electrolytes: Maintaining BalanceDocument12 pagesFluids and Electrolytes: Maintaining BalanceArlene DamoNo ratings yet
- Lipids Biologial Membrane Transport Part II PDFDocument24 pagesLipids Biologial Membrane Transport Part II PDFJia HuiNo ratings yet
- Cell Membrane Transport and StructureDocument46 pagesCell Membrane Transport and StructureFawa'idul KhoirNo ratings yet
- PCOL211 Introduction To PharmacologyDocument6 pagesPCOL211 Introduction To PharmacologyLady RabadonNo ratings yet
- Movement Across the Plasma MembraneDocument33 pagesMovement Across the Plasma MembraneAthirah BadrulshamNo ratings yet
- 10 - Transportation and Lipid Bilayer - 2020Document29 pages10 - Transportation and Lipid Bilayer - 2020tireddoodleNo ratings yet
- Cell Membrane - Corrected by SheenaDocument46 pagesCell Membrane - Corrected by SheenaJasmine YiNo ratings yet
- Membrane Transport MechanismsDocument23 pagesMembrane Transport MechanismsSIMBA The Lion KingNo ratings yet
- ANAPHY-REVIEWER-LAB-PRELIMDocument13 pagesANAPHY-REVIEWER-LAB-PRELIMdjiamaeduremdezNo ratings yet
- Cell Transport Powerpoint NotesDocument33 pagesCell Transport Powerpoint Notesapi-644325383No ratings yet
- Column FootingDocument57 pagesColumn Footingnuwan01100% (7)
- Worthy - Elevation WorshipDocument1 pageWorthy - Elevation WorshipSabine J.100% (1)
- Concept of StateDocument10 pagesConcept of StateAryansh ShuklaNo ratings yet
- A Drop of Blood: Casting Time Range Components Duration Casting Time Range Components DurationDocument6 pagesA Drop of Blood: Casting Time Range Components Duration Casting Time Range Components DurationCristobal RencoretNo ratings yet
- Medical Terminology TermsDocument28 pagesMedical Terminology TermsNikka Moreen DagdagNo ratings yet
- Seal Pores & ImperfectionsDocument1 pageSeal Pores & ImperfectionsP176414 Mohammad MazanNo ratings yet
- Quest The Last RemnantDocument67 pagesQuest The Last Remnantding suheNo ratings yet
- Types of swords from around the worldDocument4 pagesTypes of swords from around the worldДмитрий МихальчукNo ratings yet
- Digital control engineering lecture on z-transform and samplingDocument13 pagesDigital control engineering lecture on z-transform and samplingjin kazamaNo ratings yet
- Zooniverse Book 2022Document28 pagesZooniverse Book 2022Dr Pankaj DhussaNo ratings yet
- Discover Over 70 Player Classes and RacesDocument1 pageDiscover Over 70 Player Classes and RacesFred FrançaNo ratings yet
- Labcelldivision ErikagutierrezDocument10 pagesLabcelldivision Erikagutierrezapi-336047220No ratings yet
- Surat Kecil Untuk TuhanDocument9 pagesSurat Kecil Untuk TuhanAsgarPurnamaNo ratings yet
- Bernard BTB MIG GunsDocument8 pagesBernard BTB MIG GunsEdwin Mauricio Gallego OsorioNo ratings yet
- Beneficiation of Cassiterite From Primary Tin OresDocument11 pagesBeneficiation of Cassiterite From Primary Tin OresSULMAGNo ratings yet
- CH 2.2: Separable Equations: X F DX DyDocument9 pagesCH 2.2: Separable Equations: X F DX DyPFENo ratings yet
- GTA San Andreas CheatDocument9 pagesGTA San Andreas CheatHatta YanuarNo ratings yet
- Effect of Water Immersion On Mechanical Properties of Polyurethane ...Document8 pagesEffect of Water Immersion On Mechanical Properties of Polyurethane ...konshoeNo ratings yet
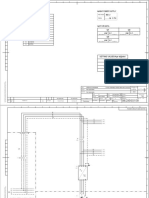
- EKO75 KW VST Air Cooled Electrical DiagramDocument13 pagesEKO75 KW VST Air Cooled Electrical DiagramBerat DeğirmenciNo ratings yet
- Bronchiolitis A Practical Approach For The General RadiologistDocument42 pagesBronchiolitis A Practical Approach For The General RadiologistTara NareswariNo ratings yet
- DM3xxx Accessory List LeafletDocument2 pagesDM3xxx Accessory List LeafletAdvantec SrlNo ratings yet
- Systems Design: Job-Order Costing and Process Costing: MANAGEMENT ACCOUNTING - Solutions ManualDocument16 pagesSystems Design: Job-Order Costing and Process Costing: MANAGEMENT ACCOUNTING - Solutions ManualBianca LizardoNo ratings yet
- Iodine Summaryupdate 2016Document26 pagesIodine Summaryupdate 2016FrankNo ratings yet
- Final Seminar ReportDocument35 pagesFinal Seminar ReportHrutik BhandareNo ratings yet
- About Softprom by ERCDocument26 pagesAbout Softprom by ERCMaryna KuryshchenkoNo ratings yet
- Philips HD5 enDocument5 pagesPhilips HD5 enmohamed boufasNo ratings yet
- Ac+lic Lab Manual 2018-19Document76 pagesAc+lic Lab Manual 2018-19Samanvi SaatviNo ratings yet
- AstigmatismDocument1 pageAstigmatismAmmellya PutriNo ratings yet
- Singaporean Notices To Mariners: Section ContentDocument35 pagesSingaporean Notices To Mariners: Section ContentGaurav SoodNo ratings yet