You might also like
- Complementary and Alternative Medical Lab Testing Part 3: CardiologyFrom EverandComplementary and Alternative Medical Lab Testing Part 3: CardiologyRating: 1 out of 5 stars1/5 (1)
- Dapa-Ckd 2020 NejmDocument11 pagesDapa-Ckd 2020 NejmInês MendonçaNo ratings yet
- Nejmoa 2024816Document11 pagesNejmoa 2024816Cessar OrnlsNo ratings yet
- AURORA: Is There A Role For Statin Therapy in Dialysis Patients?Document4 pagesAURORA: Is There A Role For Statin Therapy in Dialysis Patients?Ravan WidiNo ratings yet
- Empagliflozin Outcome Trial in Patients With Chronic Heart Failure and A Reduced Ejection Fraction - American College of CardiologyDocument5 pagesEmpagliflozin Outcome Trial in Patients With Chronic Heart Failure and A Reduced Ejection Fraction - American College of CardiologyJackeline PazNo ratings yet
- Clinical Outcomes in Antihypertensive Treatment of Type 2 Diabetes, Impaired Fasting Glucose Concentration, and NormoglycemiaDocument9 pagesClinical Outcomes in Antihypertensive Treatment of Type 2 Diabetes, Impaired Fasting Glucose Concentration, and NormoglycemiaHoài ThươngNo ratings yet
- 10.1016j.amjcard.2010.01.355 FurosemidDocument4 pages10.1016j.amjcard.2010.01.355 FurosemiddenanurbaniazharNo ratings yet
- Lowering Study (4S) : PatientsDocument7 pagesLowering Study (4S) : PatientsLuisao MerchNo ratings yet
- 27 - Comparison of Fenofibrate Vs Gemfibrozil in The Management of Hypertriglyceridemia in Patients With Chronic Heart DiseaseDocument6 pages27 - Comparison of Fenofibrate Vs Gemfibrozil in The Management of Hypertriglyceridemia in Patients With Chronic Heart DiseaseirenesuharmanNo ratings yet
- Trial of Darbepoetin Alfa in Diabetes, Kidney Disease and AnemiaDocument3 pagesTrial of Darbepoetin Alfa in Diabetes, Kidney Disease and Anemiasally cummingsNo ratings yet
- Dapa CKDDocument11 pagesDapa CKDCarlos Andres Tejeda PerezNo ratings yet
- Dapaglifozina y Anemia en Enfermedad Renal Crónica NEJMDocument10 pagesDapaglifozina y Anemia en Enfermedad Renal Crónica NEJMDolores AlemánNo ratings yet
- New England Journal Medicine: The ofDocument10 pagesNew England Journal Medicine: The ofAlina PirtacNo ratings yet
- Dibacakan Oleh:: Achmad Nur Affendick Adriana Wulandari Dionisia I. Madin Ineke Lani Dimara Lis AmitasariDocument39 pagesDibacakan Oleh:: Achmad Nur Affendick Adriana Wulandari Dionisia I. Madin Ineke Lani Dimara Lis AmitasariMc'onethree BrownNo ratings yet
- 2021 - Nejm - Figaro-DkdDocument12 pages2021 - Nejm - Figaro-DkdLuiz Fernando Fonseca VieiraNo ratings yet
- Accord StudyDocument2 pagesAccord StudyCarlos Danilo Noroña CNo ratings yet
- ARTICLEDocument13 pagesARTICLEHamzah MohiuddinNo ratings yet
- Cardiovascular Benefit of Empagliflozin Across The Spectrum of Cardiovascular Risk Factor Control in The Empa-Reg Outcome TrialDocument11 pagesCardiovascular Benefit of Empagliflozin Across The Spectrum of Cardiovascular Risk Factor Control in The Empa-Reg Outcome TrialBaginda Yusuf SiregarNo ratings yet
- Dapagliflozin and Cardiovascular Outcomes in Type 2 DiabetesDocument12 pagesDapagliflozin and Cardiovascular Outcomes in Type 2 DiabetesAlina PopaNo ratings yet
- AHA 2022 - Efficacy and Safety of Dapagliflozin in Type 2 Diabetes According to Baseline Blood PressureDocument11 pagesAHA 2022 - Efficacy and Safety of Dapagliflozin in Type 2 Diabetes According to Baseline Blood PressureBigPharma HealtcareNo ratings yet
- Clinical Cardiology - 2023 - Mo - Efficacy of Sacubitril Valsartan and SGLT2 Inhibitors in Heart Failure With ReducedDocument9 pagesClinical Cardiology - 2023 - Mo - Efficacy of Sacubitril Valsartan and SGLT2 Inhibitors in Heart Failure With ReducedLuluil MunirohNo ratings yet
- Article 9Document10 pagesArticle 9vzwsvt7hgkNo ratings yet
- Clinical Outcomes in Patients With Atrial Fibrillation and Frailty: Insights From The ENGAGE AF-TIMI 48 TrialDocument1 pageClinical Outcomes in Patients With Atrial Fibrillation and Frailty: Insights From The ENGAGE AF-TIMI 48 TrialKeshav NagpalNo ratings yet
- Diabetic Nephropathy: Landmark Clinical TrialsDocument45 pagesDiabetic Nephropathy: Landmark Clinical TrialsTRP TSYONo ratings yet
- Controversies in Hypertension II: The Optimal Target Blood PressureDocument13 pagesControversies in Hypertension II: The Optimal Target Blood PressureFideoPereNo ratings yet
- 1 s2.0 S2213177921003346 MainDocument14 pages1 s2.0 S2213177921003346 Maingladian yanuriskaNo ratings yet
- Abstracts: Nephrology Dialysis TransplantationDocument1 pageAbstracts: Nephrology Dialysis TransplantationrezkyfikriNo ratings yet
- 1 s2.0 S2213177917305358 MainDocument10 pages1 s2.0 S2213177917305358 MainMayar HassanNo ratings yet
- CHARM Alt TrialDocument5 pagesCHARM Alt TrialCristian Villarroel SNo ratings yet
- 3738 Full PDFDocument8 pages3738 Full PDFAnonymous CGmgvauebNo ratings yet
- DAPA - CKD Resets eGFR Floor For Safe SGLT2i UseDocument2 pagesDAPA - CKD Resets eGFR Floor For Safe SGLT2i UseHuynh DucNo ratings yet
- Pi Is 0272638616302645Document9 pagesPi Is 0272638616302645Eko PrasNo ratings yet
- 2832 FullDocument6 pages2832 FullAdwin AlamsyaputraNo ratings yet
- Nejmoa 010746Document9 pagesNejmoa 010746Mmle BlaséNo ratings yet
- ESCAPE Study - JAMA 2005Document9 pagesESCAPE Study - JAMA 2005MICHAEL AMARILLO CORREANo ratings yet
- CJN 08900722 Full-1Document15 pagesCJN 08900722 Full-1Ricardo IbarraNo ratings yet
- Phco 23 15 1564 31963Document9 pagesPhco 23 15 1564 31963كسلان اكتب اسميNo ratings yet
- MIMS Doctor August 2016 RGDocument43 pagesMIMS Doctor August 2016 RGDeddy SupriyadiNo ratings yet
- Olmesartan Amlodipin HCTDocument14 pagesOlmesartan Amlodipin HCTale_rhdNo ratings yet
- Journal Reading IPD Assa BudiDocument21 pagesJournal Reading IPD Assa BudiASSA AYUNo ratings yet
- Cardiorenal Outcomes in The CANVAS, DECLARE-TIMI 58, and EMPA-REG OUTCOME Trials - A Systematic ReviewDocument9 pagesCardiorenal Outcomes in The CANVAS, DECLARE-TIMI 58, and EMPA-REG OUTCOME Trials - A Systematic ReviewVaibhav DafaleNo ratings yet
- 【DAPA-CKD FSGS】Safety and efficacy of dapagliflozin in patients with focal segmental glomerulosclerosis a prespecified analysis of the DAPA-CKDDocument10 pages【DAPA-CKD FSGS】Safety and efficacy of dapagliflozin in patients with focal segmental glomerulosclerosis a prespecified analysis of the DAPA-CKD陈诗哲No ratings yet
- Cardiology: Nature ReviewsDocument15 pagesCardiology: Nature ReviewsluonganhsiNo ratings yet
- DELIVERing Progress in HFpEF NEJM 2022Document3 pagesDELIVERing Progress in HFpEF NEJM 2022Πάνος ΣταγήςNo ratings yet
- RusslanDocument11 pagesRusslandalialamasbonita1093No ratings yet
- Prevalence of Dyslipidemia in Patients on StatinsDocument7 pagesPrevalence of Dyslipidemia in Patients on StatinsKaryn Olascuaga-CastilloNo ratings yet
- Cardiovascular and Renal Outcomes With Efpeglenatide in Type 2 DiabetesDocument12 pagesCardiovascular and Renal Outcomes With Efpeglenatide in Type 2 DiabetesMoeez AkramNo ratings yet
- Nej Mo A 2024816Document20 pagesNej Mo A 2024816Ahmad Mutta'inNo ratings yet
- JAMA Internal Medicine - : Original InvestigationDocument9 pagesJAMA Internal Medicine - : Original Investigationhenry leonardo gaona pinedaNo ratings yet
- Empagliflozin in Prevention of Cardiovascular Disease Among Patients With Diabetes Mellitus Type 2Document4 pagesEmpagliflozin in Prevention of Cardiovascular Disease Among Patients With Diabetes Mellitus Type 2tb9No ratings yet
- Long-Term Outcomes of Lercanidipine Versus Other Calcium Channel Blockers in Newly Diagnosed Hypertension: A Nationwide Cohort StudyDocument8 pagesLong-Term Outcomes of Lercanidipine Versus Other Calcium Channel Blockers in Newly Diagnosed Hypertension: A Nationwide Cohort StudyApt. Mulyadi PrasetyoNo ratings yet
- The Dapagliflozin and Prevention of Adverse Outcomes in Chronic Kidney Disease (DAPA-CKD) Trial: Baseline CharacteristicsDocument12 pagesThe Dapagliflozin and Prevention of Adverse Outcomes in Chronic Kidney Disease (DAPA-CKD) Trial: Baseline CharacteristicsSorina ElenaNo ratings yet
- Intensive Glycemic Control in The ACCORD and ADVANCE Trials - EditorialDocument4 pagesIntensive Glycemic Control in The ACCORD and ADVANCE Trials - EditorialSheebaNo ratings yet
- High-Dose Clopidogrel, Prasugrel or Ticagrelor: Trying To Unravel A Skein Into A Ball. Alessandro Aprile, Raffaella Marzullo, Giuseppe Biondi Zoccai, Maria Grazia ModenaDocument8 pagesHigh-Dose Clopidogrel, Prasugrel or Ticagrelor: Trying To Unravel A Skein Into A Ball. Alessandro Aprile, Raffaella Marzullo, Giuseppe Biondi Zoccai, Maria Grazia ModenaDrugs & Therapy StudiesNo ratings yet
- Ijms-22-00287Document10 pagesIjms-22-00287vidhi parekhNo ratings yet
- Clinical Experience With A Lowdose Fixed Combination of Perindopril Plus Indapamide in A Primarycare Setting The PretendDocument7 pagesClinical Experience With A Lowdose Fixed Combination of Perindopril Plus Indapamide in A Primarycare Setting The Pretendguugle gogleNo ratings yet
- Agodoa Jama 2002Document12 pagesAgodoa Jama 2002NandaCastroMedUFJFNo ratings yet
- Evolocumab and Clinical Outcomes in Patients With Cardiovascular DiseaseDocument10 pagesEvolocumab and Clinical Outcomes in Patients With Cardiovascular Diseasepopov357No ratings yet
- Ijda 5 024 PDFDocument5 pagesIjda 5 024 PDFKumarsai DurusojuNo ratings yet
- Effects of Anacetrapib in Patients With Atherosclerotic Vascular DiseaseDocument11 pagesEffects of Anacetrapib in Patients With Atherosclerotic Vascular DiseaseCirca NewsNo ratings yet
- 2021 ESC Guidelines On Cardiac Pacing andDocument94 pages2021 ESC Guidelines On Cardiac Pacing andLeo Purba100% (1)
- SAMPLE Solve Exam Type Maths P3Document10 pagesSAMPLE Solve Exam Type Maths P3Binod KumarNo ratings yet
- Arrhythmia in Cardiac SarcoidosisDocument12 pagesArrhythmia in Cardiac SarcoidosisBinod KumarNo ratings yet
- ESC Guidelines CardiomyopathiesDocument124 pagesESC Guidelines CardiomyopathiesSergio Mora CanelaNo ratings yet
- 2019 ESC Guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS) The Task Force for the diagnosis and management of acute pulmonary embolism of the European Society of Cardiology (ESC)Document61 pages2019 ESC Guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS) The Task Force for the diagnosis and management of acute pulmonary embolism of the European Society of Cardiology (ESC)AdelaNo ratings yet
- Guias ESC para Insuficiencia Cardiaca CronicaDocument128 pagesGuias ESC para Insuficiencia Cardiaca CronicaKarla HernandezNo ratings yet
- Ehab 484Document111 pagesEhab 484aslinNo ratings yet
- MATHS PARTNER Book 5 - Sample PagesDocument10 pagesMATHS PARTNER Book 5 - Sample PagesBinod KumarNo ratings yet
- 2021 ESC/EACTS Guidelines For The Management of Valvular Heart DiseaseDocument72 pages2021 ESC/EACTS Guidelines For The Management of Valvular Heart DiseaseAdriana VladutuNo ratings yet
- ESC Arterial Hypertension 2018Document98 pagesESC Arterial Hypertension 2018ddantoniusgmailNo ratings yet
- 2020 ESC Guidelines On Sports Cardiology and Exercise in Patients With Cardiovascular DiseaseDocument80 pages2020 ESC Guidelines On Sports Cardiology and Exercise in Patients With Cardiovascular DiseaseBinod KumarNo ratings yet
- 2020 ESC Guidelines For The Management of Adult Congenital Heart DiseaseDocument84 pages2020 ESC Guidelines For The Management of Adult Congenital Heart DiseaseBinod KumarNo ratings yet
- 4 5931499803149076504 PDFDocument126 pages4 5931499803149076504 PDFCristianAltunaSotomayorNo ratings yet
- Ehaa575 PDFDocument79 pagesEhaa575 PDFPatricia MarceloNo ratings yet
- Ehz 467Document66 pagesEhz 467Cosmina Alina MoscuNo ratings yet
- Ghid Dislipidemie 2019Document78 pagesGhid Dislipidemie 2019Ema PetrescuNo ratings yet
- 2019 ESC Guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS) The Task Force for the diagnosis and management of acute pulmonary embolism of the European Society of Cardiology (ESC)Document61 pages2019 ESC Guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS) The Task Force for the diagnosis and management of acute pulmonary embolism of the European Society of Cardiology (ESC)AdelaNo ratings yet
- ESC Guidelines Hypertrophic CardiomyopathyDocument55 pagesESC Guidelines Hypertrophic CardiomyopathyFlavian ȚuțuianuNo ratings yet
- 2018 ESC-EACTS Guidelines On Myocardial RevascularizationDocument96 pages2018 ESC-EACTS Guidelines On Myocardial RevascularizationTony Miguel Saba SabaNo ratings yet
- Syncope Guideline ESC 2018Document69 pagesSyncope Guideline ESC 2018ddantoniusgmailNo ratings yet
- Guidlines Gagal Jantung Dengan Kehamilan 2018 EscDocument84 pagesGuidlines Gagal Jantung Dengan Kehamilan 2018 EscanakratukuberasNo ratings yet
- Pericardial DiseaseDocument44 pagesPericardial DiseaseAlin AmaliyahNo ratings yet
- ESC Guidelines on Diagnosis and Treatment of Aortic DiseasesDocument62 pagesESC Guidelines on Diagnosis and Treatment of Aortic DiseasesDidi SNo ratings yet
- 2018 AHA Guidelines For Management of Blood CholesterolDocument66 pages2018 AHA Guidelines For Management of Blood CholesterolsarumaxNo ratings yet
- Ehv319 PDFDocument54 pagesEhv319 PDFPrisela Zharaswati SagaNo ratings yet
- J Jacc 2020 11 0907Document39 pagesJ Jacc 2020 11 0907Mister SimpleNo ratings yet
- 2020 Acute Chest Pain in The Emergency Department 20222Document36 pages2020 Acute Chest Pain in The Emergency Department 20222Binod KumarNo ratings yet
- 2021 AC and APT Decision Pathway For AF VTE and PCI ASCVDDocument30 pages2021 AC and APT Decision Pathway For AF VTE and PCI ASCVDPeter Albeiro Falla CortesNo ratings yet
- Influenza B SymptomsDocument5 pagesInfluenza B SymptomsHoonchyi KohNo ratings yet
- Impact of Domestic Violence On FamiliesDocument2 pagesImpact of Domestic Violence On FamiliesNastassia CampbellNo ratings yet
- Bacteria Causing Respiratory Tract Infections: Damanhour University Faculty of PharmacyDocument7 pagesBacteria Causing Respiratory Tract Infections: Damanhour University Faculty of Pharmacyزياد محمدNo ratings yet
- Sarawak Handbook of Medical Emergencies, 3rd EdDocument410 pagesSarawak Handbook of Medical Emergencies, 3rd EdKelvin SuNo ratings yet
- Lecture 1 Cancer IntroductionDocument18 pagesLecture 1 Cancer IntroductionShreeyaNo ratings yet
- Dr. Sheeba Farooqui, Dr. Manisha Sharma, Dr. NamrataDocument31 pagesDr. Sheeba Farooqui, Dr. Manisha Sharma, Dr. NamrataSheeba SiddiquiNo ratings yet
- Precious Marie Dipus - Synthesis PaperDocument5 pagesPrecious Marie Dipus - Synthesis PaperPreciousNo ratings yet
- Diagnosis and Management of Dyslipidemia in Family PracticeDocument19 pagesDiagnosis and Management of Dyslipidemia in Family PracticeMikhaela Katrina AzarconNo ratings yet
- Advances in Cancer Immunotherapy 2019 - Latest TrendsDocument21 pagesAdvances in Cancer Immunotherapy 2019 - Latest TrendsSWAGATIKA CHANDANo ratings yet
- Understanding Spina BifidaDocument3 pagesUnderstanding Spina BifidaSham ObaidatNo ratings yet
- The Influence of Spleen On Portal HemodynamicsDocument1 pageThe Influence of Spleen On Portal HemodynamicsdenisegmeloNo ratings yet
- Continuum Parasomnias No REM 2021Document13 pagesContinuum Parasomnias No REM 2021siralkNo ratings yet
- Module 2 - Civic Welfare Training Service 2Document2 pagesModule 2 - Civic Welfare Training Service 2Ezekiel MirandaNo ratings yet
- 4'Rs of Radiobiology: Nilesh Kumar PG Radiation Physics Deapartment of Radiation PhysicsDocument23 pages4'Rs of Radiobiology: Nilesh Kumar PG Radiation Physics Deapartment of Radiation Physicsnilesh kumarNo ratings yet
- Forensic Emergency MedicineDocument36 pagesForensic Emergency MedicinePrajwal Rao KNo ratings yet
- 1-Upper GI Malignancy (Moodle)Document31 pages1-Upper GI Malignancy (Moodle)Abdulrahman NanakaliNo ratings yet
- Common Signs and Symptoms of Drug Dependence and AddictionDocument4 pagesCommon Signs and Symptoms of Drug Dependence and AddictionAbbygail WasilNo ratings yet
- SEMINARDocument31 pagesSEMINARDeveshNo ratings yet
- J Jacc 2023 02 011Document3 pagesJ Jacc 2023 02 011Evania BeatriceNo ratings yet
- ATI RN Mental Health Online Practice BDocument38 pagesATI RN Mental Health Online Practice Bseansdrew2No ratings yet
- Ais Student Medical and Health Declaration Form 2023-24Document7 pagesAis Student Medical and Health Declaration Form 2023-24hafizvy6No ratings yet
- Notes Skin Eye Ears Infections MicrobioDocument18 pagesNotes Skin Eye Ears Infections MicrobioChristiel John MagtibayNo ratings yet
- ACCRE Test Parameters 2022Document3 pagesACCRE Test Parameters 2022jishnu.m89No ratings yet
- CT BrainDocument230 pagesCT BrainpraveenbhavniNo ratings yet
- Amlodipine - Drug StudyDocument2 pagesAmlodipine - Drug StudyAcads useNo ratings yet
- Reference For Assignment 2Document2 pagesReference For Assignment 2chrisNo ratings yet
- Common illnesses and injuriesDocument2 pagesCommon illnesses and injuriesNastya Bondar'No ratings yet
- Common ICD 10 CodesDocument2 pagesCommon ICD 10 CodesAhmadNo ratings yet
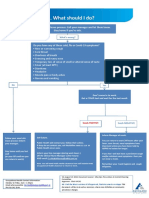
- What To Do If Youre Sick FlowchartDocument1 pageWhat To Do If Youre Sick FlowchartfuckyouNo ratings yet
- Ringworm in CatsDocument4 pagesRingworm in CatsZain AsifNo ratings yet