You might also like
- Proactive-And-reactive-practices-cabello Ma. Cristina & Cabillo Patrizia Ianne LDocument11 pagesProactive-And-reactive-practices-cabello Ma. Cristina & Cabillo Patrizia Ianne LcristinaNo ratings yet
- Websdr PDFDocument11 pagesWebsdr PDFDoruNastaseNo ratings yet
- Short Answer Questions CHCCSM004Document14 pagesShort Answer Questions CHCCSM004Tmg Preity100% (2)
- Logix 5000 Controllers Tasks, Programs, and RoutinesDocument73 pagesLogix 5000 Controllers Tasks, Programs, and Routinesobi SalamNo ratings yet
- Islamic ArchitectureDocument84 pagesIslamic ArchitecturesidNo ratings yet
- Evidence Based Healthcare DesignDocument66 pagesEvidence Based Healthcare DesignGerry C FinneyNo ratings yet
- Vasuanand Bba ProjectDocument66 pagesVasuanand Bba ProjectMaster PrintersNo ratings yet
- Rod and Pump DataDocument11 pagesRod and Pump DataYoandri Stefania Guerrero CamargoNo ratings yet
- 2005 Coolidge - Psychometric Properties of The Revised Dental Beliefs SurveyDocument9 pages2005 Coolidge - Psychometric Properties of The Revised Dental Beliefs Surveyfabian.balazs.93No ratings yet
- Journal Pone 0094207Document7 pagesJournal Pone 0094207JuanaNo ratings yet
- 2001 Kulich - Factor Structure of The Dental Beliefs Survey in A Dental Phobic PopulationDocument6 pages2001 Kulich - Factor Structure of The Dental Beliefs Survey in A Dental Phobic Populationfabian.balazs.93No ratings yet
- Guidelines For Reporting Reliability and Agreement Studies (GRRAS) Were ProposedDocument12 pagesGuidelines For Reporting Reliability and Agreement Studies (GRRAS) Were ProposedNel LimaNo ratings yet
- An Overview of 19 Instruments Assessing The Doctor-Patient Relationship: Different Models or Concepts Are UsedDocument6 pagesAn Overview of 19 Instruments Assessing The Doctor-Patient Relationship: Different Models or Concepts Are UsedDaria MoldovianNo ratings yet
- 2009 Abrahamsson - Dental Beliefs Factor Structure of The Revised Dental Beliefs Survey in ADocument8 pages2009 Abrahamsson - Dental Beliefs Factor Structure of The Revised Dental Beliefs Survey in Afabian.balazs.93No ratings yet
- 2023 Lu - RCT MetaqDocument13 pages2023 Lu - RCT Metaqfabian.balazs.93No ratings yet
- Jurnal ReferensiDocument10 pagesJurnal ReferensiBidang KeperawatanNo ratings yet
- Measuring Children's Dental Anxiety: Oral Cancer /paediatric DentistryDocument2 pagesMeasuring Children's Dental Anxiety: Oral Cancer /paediatric DentistryManda JoanNo ratings yet
- Patient Provider Communication Data Linking Process and Outcomes in Oncology CareDocument8 pagesPatient Provider Communication Data Linking Process and Outcomes in Oncology CareMuhammad HafizhNo ratings yet
- Patient-Centred Consultations and Outcomes in Primary Care: A Review of The LiteratureDocument11 pagesPatient-Centred Consultations and Outcomes in Primary Care: A Review of The LiteratureIan Mizzel A. DulfinaNo ratings yet
- The Association Between Health Care Staff EngagementDocument10 pagesThe Association Between Health Care Staff Engagementtsa638251No ratings yet
- Patient Experience Quest-Addo 2021Document19 pagesPatient Experience Quest-Addo 2021Claudia MoksidyNo ratings yet
- 2007 CESItem Level PsychometricsDocument15 pages2007 CESItem Level PsychometricsCamila Andrea Barrera BlancoNo ratings yet
- 2002 Dutch CI - SiDocument4 pages2002 Dutch CI - SiFreddy Campos SotoNo ratings yet
- Dentist-Patient Communication and Patientsã  ™ Satisfaction With Prosthetic Dentistry Treatment Among Saudi Adults: A Cross-Sectional StudyDocument16 pagesDentist-Patient Communication and Patientsã  ™ Satisfaction With Prosthetic Dentistry Treatment Among Saudi Adults: A Cross-Sectional StudyIJAR JOURNALNo ratings yet
- 10 1016@j Socscimed 2019 112391Document8 pages10 1016@j Socscimed 2019 112391fatmadita17No ratings yet
- Doctor-Patient CommunicationDocument10 pagesDoctor-Patient CommunicationrhismaNo ratings yet
- Patient Education and CounselingDocument6 pagesPatient Education and CounselingLeni AgustinNo ratings yet
- Validity of Scores From Communication Skills Instruments For Patients and Their Dental Student-CliniciansDocument8 pagesValidity of Scores From Communication Skills Instruments For Patients and Their Dental Student-CliniciansXinyue XuNo ratings yet
- Assessment Task 3 AT 3 - Literature Review MatrixDocument17 pagesAssessment Task 3 AT 3 - Literature Review Matrixdanilo jr siquig100% (1)
- Patient Satisfaction DissertationDocument9 pagesPatient Satisfaction DissertationBuyCollegePapersSingapore100% (1)
- Impact - Ijranss-1. Ijranss - Length of Stay Reporting in Forensic Secure Care Can Be Augmented by An Overarching Framework To Map Patient Journey in Mentally Disordered Offender Pathway ForDocument38 pagesImpact - Ijranss-1. Ijranss - Length of Stay Reporting in Forensic Secure Care Can Be Augmented by An Overarching Framework To Map Patient Journey in Mentally Disordered Offender Pathway ForImpact JournalsNo ratings yet
- Metaanalisis Castro Et Al. 2019Document37 pagesMetaanalisis Castro Et Al. 2019LauraNo ratings yet
- Journal Homepage: - : IntroductionDocument8 pagesJournal Homepage: - : IntroductionIJAR JOURNALNo ratings yet
- Importance of Biostatistics To Improve The Quality of Medical JournalsDocument6 pagesImportance of Biostatistics To Improve The Quality of Medical JournalsAnand KasiNo ratings yet
- Outcomes Research What Is It and Why Does It MatteDocument10 pagesOutcomes Research What Is It and Why Does It MatteAnnushqua ShuklaNo ratings yet
- Humphris 2009Document8 pagesHumphris 2009Anonymous 9KcGpvNo ratings yet
- The Enduring and Evolving Nature of The Patient-PhysicianDocument11 pagesThe Enduring and Evolving Nature of The Patient-PhysicianSYLVIA RAMIS ASENJONo ratings yet
- Effect of Probiotics As A Complement To Non Surgical Periodontal Therapy in Chronic Periodontitis A Systematic RevieDocument7 pagesEffect of Probiotics As A Complement To Non Surgical Periodontal Therapy in Chronic Periodontitis A Systematic RevieMohammedNo ratings yet
- Cerebral PalsyDocument7 pagesCerebral PalsysaadchalidNo ratings yet
- What Are Patients Expectations of Orthodontic TreDocument9 pagesWhat Are Patients Expectations of Orthodontic TreAly OsmanNo ratings yet
- Investigation of Effective Communication Skills: in BuildingDocument23 pagesInvestigation of Effective Communication Skills: in BuildingItrat ShiraziNo ratings yet
- Dentist-Patient Relationships and Oral Health Impact in Australian AdultsDocument8 pagesDentist-Patient Relationships and Oral Health Impact in Australian AdultsNisaNo ratings yet
- How The Doc Should (Not) Talk - When Breaking Bad News With NegationsDocument7 pagesHow The Doc Should (Not) Talk - When Breaking Bad News With NegationsDr. Daniel Gutierrez GarciaNo ratings yet
- Evidence-Basedprosthodontics: Fundamental Considerations, Limitations, and GuidelinesDocument17 pagesEvidence-Basedprosthodontics: Fundamental Considerations, Limitations, and GuidelinesRohan BhagatNo ratings yet
- Does Doctor-Patient Stability Affect The Provision of Good Medical Care?Document5 pagesDoes Doctor-Patient Stability Affect The Provision of Good Medical Care?Arif EndotelNo ratings yet
- Cunningham - Perceptions of Outcomes of Orthodontic Treatment in Adolescent Patients - A Qualitative StudyDocument21 pagesCunningham - Perceptions of Outcomes of Orthodontic Treatment in Adolescent Patients - A Qualitative StudyMilton david Rios serratoNo ratings yet
- 2008 Öhrn - Dental Beliefs Patients Specific Attitudes Towards Dentists and Dental Hygienists ADocument9 pages2008 Öhrn - Dental Beliefs Patients Specific Attitudes Towards Dentists and Dental Hygienists Afabian.balazs.93No ratings yet
- Emergency Department Patient Experience - A Systematic Review of The LiteratureDocument6 pagesEmergency Department Patient Experience - A Systematic Review of The LiteratureMauricio Garcia RomeroNo ratings yet
- Clinical Reasoning in Dentistry: A Conceptual Framework For Dental EducationDocument13 pagesClinical Reasoning in Dentistry: A Conceptual Framework For Dental EducationDrSanaa AhmedNo ratings yet
- Factors in Uencing Satisfaction With The Process of Orthodontic Treatment in Adult PatientsDocument9 pagesFactors in Uencing Satisfaction With The Process of Orthodontic Treatment in Adult PatientsLikhitaNo ratings yet
- Assessing What Matters Most To Patients With or atDocument16 pagesAssessing What Matters Most To Patients With or atandreamandu25No ratings yet
- Far Eastern University Institute of Nursing: Clinical QuestionDocument6 pagesFar Eastern University Institute of Nursing: Clinical QuestionshielaniNo ratings yet
- Highlight Bubu 1Document7 pagesHighlight Bubu 1soniNo ratings yet
- 12 Evidence Based Period Ontology Systematic ReviewsDocument17 pages12 Evidence Based Period Ontology Systematic ReviewsAparna PandeyNo ratings yet
- Determinant of Patient SatisfactionDocument8 pagesDeterminant of Patient SatisfactionAhmad Nurhadi Al-GhazaliNo ratings yet
- Mental Health Services Research Methodology 2002Document8 pagesMental Health Services Research Methodology 2002Kats CoelloNo ratings yet
- Changes in Symptoms of Anxiety, Depression, and PTSD in An RCT-study of Dentist-Administered Treatment of Dental AnxietyDocument11 pagesChanges in Symptoms of Anxiety, Depression, and PTSD in An RCT-study of Dentist-Administered Treatment of Dental AnxietyMaria GuzuNo ratings yet
- Strength and Limitations of Early Warning ScoreDocument33 pagesStrength and Limitations of Early Warning ScorePerawat CPNS 2018 RSUP Dr. KariadiNo ratings yet
- International Journal of Pediatric OtorhinolaryngologyDocument4 pagesInternational Journal of Pediatric Otorhinolaryngologyzaenal abidinNo ratings yet
- Cheng - Bridges Et Al 2015 - Dental - Update - A Review of Communication Models in Healthcare ContextsDocument5 pagesCheng - Bridges Et Al 2015 - Dental - Update - A Review of Communication Models in Healthcare ContextsXinyue XuNo ratings yet
- Integrative Literature CompletedDocument20 pagesIntegrative Literature Completedapi-431939757No ratings yet
- Services Production and Patient Satisfaction in Primary CareDocument10 pagesServices Production and Patient Satisfaction in Primary CareLindsey JonesNo ratings yet
- 1 s2.0 S2452301116301225 MainDocument10 pages1 s2.0 S2452301116301225 MainNia AnggreniNo ratings yet
- Making The Best Clinical Decision DCNADocument18 pagesMaking The Best Clinical Decision DCNAJohnNo ratings yet
- Hey Man 2018Document7 pagesHey Man 2018Sung Soon ChangNo ratings yet
- Quality Measures: The Revolution in Patient Safety and OutcomesFrom EverandQuality Measures: The Revolution in Patient Safety and OutcomesDeeb N. SalemNo ratings yet
- 2019 Höglund - Evaluation of The Ability of Dental Clinicians To Rate Dental AnxietyDocument7 pages2019 Höglund - Evaluation of The Ability of Dental Clinicians To Rate Dental Anxietyfabian.balazs.93No ratings yet
- 2020 Cai - Efficacy of Aromatherapy On Dental Anxiety A Systematic Review of Randomised andDocument19 pages2020 Cai - Efficacy of Aromatherapy On Dental Anxiety A Systematic Review of Randomised andfabian.balazs.93No ratings yet
- 2023 Andrade - REVIEWDocument4 pages2023 Andrade - REVIEWfabian.balazs.93No ratings yet
- 2022 Muhaish - Dental Anxiety Screening and Management Practices in Dental Practice in Eastern Province Saudi ArabiaDocument12 pages2022 Muhaish - Dental Anxiety Screening and Management Practices in Dental Practice in Eastern Province Saudi Arabiafabian.balazs.93No ratings yet
- 2023 Taheri - Associations-Between-The-Perception-Of-Dental-Pain-And-Pain-Anxiety-Mental-Pain-And-Dental-Anxiety-InDocument16 pages2023 Taheri - Associations-Between-The-Perception-Of-Dental-Pain-And-Pain-Anxiety-Mental-Pain-And-Dental-Anxiety-Infabian.balazs.93No ratings yet
- 2017 IbrahimDocument7 pages2017 Ibrahimfabian.balazs.93No ratings yet
- 22445-2022-Summer-Model-Answer-Paper (Msbte Study Resources)Document27 pages22445-2022-Summer-Model-Answer-Paper (Msbte Study Resources)Piyush NikamNo ratings yet
- Penjelasan IMRAD StructureDocument2 pagesPenjelasan IMRAD Structureaji bondesNo ratings yet
- Biodiversity ReportDocument52 pagesBiodiversity ReportAdrian HudsonNo ratings yet
- 300 Top Fluid Mechanics Multiple Choice Questions With Answers PDFDocument20 pages300 Top Fluid Mechanics Multiple Choice Questions With Answers PDFpiluNo ratings yet
- Cept FinalDocument14 pagesCept FinalVighnesh MalagiNo ratings yet
- Laboratory Activity No 3Document11 pagesLaboratory Activity No 3MAE MALALUANNo ratings yet
- Excel Subhadip NandyDocument9 pagesExcel Subhadip NandyNihilisticDelusionNo ratings yet
- JNTUK SGPA Calculator - JNTU Kakinada R20, R19, R16 SGPA Calculator OnlineDocument3 pagesJNTUK SGPA Calculator - JNTU Kakinada R20, R19, R16 SGPA Calculator OnlineRamesh Dasari0% (1)
- 1 Man Is The Crowning Glory of God's CreationDocument12 pages1 Man Is The Crowning Glory of God's CreationCaptainBreezy YeezyNo ratings yet
- "L8" Drive End: Operation - Assembly Instructions and Parts List ForDocument7 pages"L8" Drive End: Operation - Assembly Instructions and Parts List ForACCA PumpsNo ratings yet
- Projects & Operations: IN: NE Power Systm ImprvmDocument5 pagesProjects & Operations: IN: NE Power Systm ImprvmGaurang PatelNo ratings yet
- Free LinkDocument40 pagesFree LinkiguinhocoelhaoNo ratings yet
- Pakistan: Nation-State, State-Nation or Multinational State?Document12 pagesPakistan: Nation-State, State-Nation or Multinational State?Asif KhanNo ratings yet
- (E) Chapter 1 - Origin of Soil and Grain SizeDocument23 pages(E) Chapter 1 - Origin of Soil and Grain SizeLynas Beh TahanNo ratings yet
- Abrar AwolDocument153 pagesAbrar AwolErmias Assaminew AlmazNo ratings yet
- IPS e El 110Document105 pagesIPS e El 110alinaghibNo ratings yet
- Mathematics IDocument247 pagesMathematics IShreya PankajNo ratings yet
- Clapham - Creativity TrainingDocument11 pagesClapham - Creativity TrainingNevenka JakšićNo ratings yet
- Theodore Metochites 1981 Greek Orthodox Theological ReviewDocument47 pagesTheodore Metochites 1981 Greek Orthodox Theological ReviewMatt BrielNo ratings yet
- Wuolah Free Use of EnglishDocument20 pagesWuolah Free Use of EnglishCristina CórcolesNo ratings yet
- Economics Key WordsDocument30 pagesEconomics Key WordsJanetNo ratings yet
- Grammar - File12 C ROMERO VIDALDocument3 pagesGrammar - File12 C ROMERO VIDALYuy Oré Pianto50% (2)
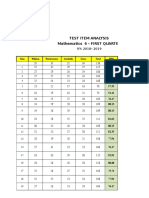
- Test Item Analysis Mathematics 6 - FIRST QUARTER: Item Wisdom Perseverance Gratitude Grace Total MPSDocument6 pagesTest Item Analysis Mathematics 6 - FIRST QUARTER: Item Wisdom Perseverance Gratitude Grace Total MPSQUISA O. LAONo ratings yet