Professional Documents
Culture Documents
BARU InequitiesAccessHealth 2010
Uploaded by
suchika.jnuOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
BARU InequitiesAccessHealth 2010
Uploaded by
suchika.jnuCopyright:
Available Formats
Inequities in Access to Health Services in India: Caste, Class and Region
Author(s): RAMA BARU, ARNAB ACHARYA, SANGHMITRA ACHARYA, A K SHIVA
KUMAR and K NAGARAJ
Source: Economic and Political Weekly , SEPTEMBER 18-24, 2010, Vol. 45, No. 38
(SEPTEMBER 18-24, 2010), pp. 49-58
Published by: Economic and Political Weekly
Stable URL: http://www.jstor.com/stable/25742094
JSTOR is a not-for-profit service that helps scholars, researchers, and students discover, use, and build upon a wide
range of content in a trusted digital archive. We use information technology and tools to increase productivity and
facilitate new forms of scholarship. For more information about JSTOR, please contact support@jstor.org.
Your use of the JSTOR archive indicates your acceptance of the Terms & Conditions of Use, available at
https://about.jstor.org/terms
Economic and Political Weekly is collaborating with JSTOR to digitize, preserve and extend
access to Economic and Political Weekly
This content downloaded from
139.167.49.154 on Sun, 26 Nov 2023 13:40:47 +00:00
All use subject to https://about.jstor.org/terms
Inequities in Access to Health Services in India:
Caste, Class and Region
RAMA BARU, ARNAB ACHARYA, SANGHMITRA ACHARYA, A K SHIVA KUMAR, K NAGARAJ
Despite India's impressive economic performance after India, over the last two decades, has enjoyed accelerated
the introduction of economic reforms in the 1990s, economic growth, but has fared poorly in human develop
ment indicators and health outcomes. Population averages of
progress in advancing the health status of Indians has
health status indicators, such as child health and maternal mor
been slow and uneven. Large inequities in health and tality, remain unacceptably high compared with countries in the
access to health services continue to persist and have south and east Asian region that have similar income levels and
even widened across states, between rural and urban rates of economic growth. Underlying the low population level
indicators, worrisome inequities coincide with the multiple axes
areas, and within communities. Three forms of inequities
of caste, class, gender and regional differences (Deaton and
have dominated India's health sector. Historical Dreze 2009; Claeson et al 2000; Subramanian et al 2006).
inequities that have their roots in the policies and In India, an important determinant of socio-economic inequi
practices of British colonial India, many of which ties in nearly all spheres of well-being is caste. The official classi
fication defines four categories of caste: scheduled castes (scs),
continued to be pursued well after independence;
scheduled tribes (sts), Other Backward Classes (obcs), and oth
socio-economic inequities manifest in caste, class and ers. The scs, the lowest level in the hierarchy, constitute around
gender differentials; and inequities in the availability, 16% of the Indian population, a large percentage of who live in
utilisation and affordability of health services. Of these, rural areas and are landless agricultural labourers. The sts, or
adivasis, often like scs, suffer economic and social deprivation.
critical to ensuring health for all in the immediate future
They comprise around 8% of India's population, obcs and for
will be the effectiveness with which India addresses
ward castes together comprise 76% of India's total population
inequities in provisioning of health services and (rgi 2001).
assurance of quality care. Taking the under-five-mortality rate (usmr), i e, mortality
among children younger than five years; as an indicator, we
describe inequities in the health status. The National Family
Health Survey (nfhs 2005-06) reveals sharp regional and socio
economic divides in health outcomes, with the lower castes, the
poor and the less developed states bearing the burden of mortal
ity disproportionately. High rates of infant mortality and usmr
are, in general, inversely associated with income. These inequi
ties are also accompanied by wide gaps across gender and caste
(Gwatkin 2000; Subramanian et al 2006). The risks of mortality
before the age of five years are higher in girls than in boys; among
scs, sts obcs as compared to others; and in the rural areas of
Uttar Pradesh (up), one of the poorest states in India, than urban
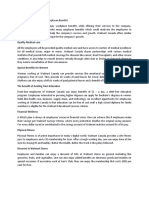
Kerala. Evidence from urban areas in Kerala and from educated
mothers (completing 12 years of education) has shown that low
We would like to thank Sandeep Sharma for data processing and
research assistance. mortality in children younger than five years is, indeed, possible
in India, usmr for the richest income quintile earners is three
Rama Baru (rbaru2002@yahoo.co.uk) is with the Centre of Social
times lower than that for the poorest quintile (Figure 1, p 50).
Medicine and Community Health, JNU, New Delhi. Arnab Acharya
(arnab.acharya@lshtm.ac.uk) is with the London School of Hygiene and
The Indian average for usmr decreased from a rate of 101 (per
Tropical Medicine. Sanghmitra Acharya (sanghmitrasacharya@yahoo. 1,000) to 74 (per 1,000) during the accelerated economic growth
com) is with the Centre of Social Medicine and Community Health, JNU. from 1998 to 2006. However, this is a period marked by increas
A K Shiva Kumar (akshivakumar@gmail.com) is consultant, UNICEF, ing inequities, as shown by a high usmr among the scs and sts,
New Delhi and K Nagaraj (nagaraj@mids.ac.in) is with the Asian College
when compared with the backward classes and others. This
of Journalism, Chennai.
social gap had increased dramatically in the 1990s for the sts, in
Economic & Political weekly BQC3 September 18, 2010 vol xlv no 38 49
This content downloaded from
139.167.49.154 on Sun, 26 Nov 2023 13:40:47 +00:00
All use subject to https://about.jstor.org/terms
SPECIAL ARTICLE
comparison with the Figure 1: Inequities in Under-Five Mortality in India reproductive and child health survey on primary health centres
(2006)
general population, 0 20 40 60 80 100 120 (phcs). For the demand-side analysis, we have used data from
while the social gap three rounds of nfhs, conducted in 1992-93,1995-96 and 2005
between the scs and 06, to obtain information on utilisation of maternal and child
others; and backward health services, antenatal care (anc) and immunisation cover
classes and others have age. To assess utilisation of health services and the associated
persisted from the expenditure, three rounds of National Sample Survey Organisation
early 1990s to 2006. (nsso), i e, nsso 42nd round of 1986-87, 52nd round of 1995-96
For example, the aver and 60th round of 2004 have been used.
age annual rate of
reduction in usmr 2 Features of Health Service Provisioning
between 1998-99 and The present status of health service delivery has its roots in the
2005-06 among sts policy and practices during the British colonial period (Banerji
(3.9%) and scs (4.2%) 1985; Priya 2005). Many of these policies were pursued even after
was lower than that independence and health services were marked by inequities in
among obcs (4.8%) and availability and accessibility. Consensus is that even during the
the rest of the popula post-independence period, health services were under-financed
tion (4.6%) (Figure 2). and biased towards allopathic medicine, urban areas and curative
Trends in India's in Source: (1) HPS and Macro International (2007); NFHS 3,2005-06:
India Voll. services. Indigenous systems like ayurveda, siddha, unani and
fant mortality rates (2) http://www.nfhsindia.org/report.html accessed on
19 June 2009. homeopathy, continue to play only a marginal role in health
(imr) similarly capture service delivery (Banerji 1985).
a slowing down in the rates of improvement in child survival. For Figure 2: Social Gap in Under-Five Mortality for Three Periods 1992-93* 1998-99 and
instance, the average annual rate of reduction in imr, which was 2005-06
2.91% during 1976-86, dropped to 2.84% from 1986 to 1996, and
further to 2.31% during 1996-2006. The decade of the 1980s saw 101
a 27% decline in the country's imr from 110 in 1981 to 80 in 1991.
The next 10 years, 1991-2001, corresponding to the first decade of
economic reforms, witnessed a considerable slowing down in the
rates of reduction, a decline of 19% in imr to 66 in 2001 (Claeson
et al 2000; Mari Bhat 2001).
1 Determinants of Health Inequities
Three major forms of inequities have been largely responsible for
the persistent and even widening differentials in health outcomes:
historical inequities, socio-economic inequities and inequities in
provision and access to health services. Among the various factors NFHS years
* 1992-93 NFHS round did not collect data separately for OBCs and those who are not SCs, STs
that influence health, availability, accessibility and affordability andOBCs.
Source:HPS, 1995.NFHS, 1992-93 HPS and Macro International 2000,2007, NFHS 2,1998-99, NFHS 3:
of health services are important determinants for improving pop 2005-06, Vol 1.
ulation health. Healthcare financing and provisioning arrange
ments play a critical role in reducing or perpetuating existing The public health service institutions are sub-centres and
inequities and shape the pattern of health service use and ex phcs at the most basic or the primary level; community health
penditure (Gilson et al 2007; Mackintosh 2001). This paper seeks centres and hospitals at the secondary and teaching hospitals at
to examine the status of health service delivery in India and the the tertiary level. Over the last six decades, there has been an
constraints it faces for achieving equity by addressing the follow expansion of facilities in the public and private sectors. However,
ing objectives: by and large, this expansion has been inadequate to ensure uni
To examine the inequities in availability, accessibility and af versal coverage and access to quality care. The rural-urban and
fordability across geographic, social and economic groups. interstate variations in the distribution of public facilities and hu
To examine key health service barriers that are responsible for man resources are well known (Duggal et al 2005). These inter
inequities in access. state variations are explained by several factors including insuf
To examine recent initiatives for reducing inequities in availa ficient public investments and failure to focus attention on the
bility, accessibility and affordability of health services. synergies between the role of the centre and the states financing,
In order to examine the first objective, we have relied on sev provisioning and administration of health services. Constitution
eral data sources. For availability of health services the major ally, the responsibility for implementation of health interventions
sources are the Central Bureau of Health Intelligence, Ministry of lies largely on the state governments, with the central govern
Health and Family Welfare, Government of India, and the ment providing policy directions and the financing of national
National Facility Survey Report conducted in 2003 as part of the health programmes.
5? September 18, 2oio vol xlv no 38 E3223 Economic & Political weekly
This content downloaded from
139.167.49.154 on Sun, 26 Nov 2023 13:40:47 +00:00
All use subject to https://about.jstor.org/terms
SPECIAL ARTICLE
Apart from direct state financing, covering only a small segment Table 1: Selected Health and Socio-economic Indicators: Kerala, UP and India
Indicators Year Kerala Uttar Pradesh India
of the population, there are several public insurance schemes for
employees in the organised sectors such as the employees' state Population (in millions)_2009_34 194 1,160
Female-to-male ratio (females per 1,000 males) 2009 1,052 898 932
insurance scheme, central government health scheme, railways
Per capita state domestic product (Rs) 2006-07 33,609 14,649 29,642
and posts and telegraph services. Public and private insurance 2001-05 74 62 63
Life expectancy at birth (years)
schemes cover barely 11% of the population (goi 2006). Conse 2005-06 16 96 74
Under-five mortality rate
quently, healthcare is financed substantially through out-of-pocket Infant mortality rate 2007 13 69 55
(oop) payments by individuals and households. Literacy rate (%) 2001 91 56 65
The private sector, constituting both "for profit" and "non Female literacy rate (%) 2001 88 42 54
profit" institutions, has a sizeable presence in delivery of health Population covered by a sub-centre _4,628 6,416 5
services, which comprises a wide array of institutions with vary Population covered by a PHC 29,570 45,095 3
% of villages having access to a PHC
ing degrees of sophistication in terms of services and qualified within five km 94 48 44
personnel. The "for profit" sector is proportionately larger than
PHC with at least 60% of inputs:
the "non-profit" sector; the latter includes community level pro Infrastructure
_65 17 32
grammes, dispensaries and hospitals that are funded by religious Staff_ _97 53 48
and secular organisations (Nundy 2005). There is diversity and Supply _78 20 40
hierarchy in the institutional composition of the for profit sector Population served per government hospital _1,77,614 6,01,241 1,56,556
consisting of a range of informal practitioners, clinics, small and Population per government hospital bed _1,299 20,041 2,336
% deliveries attended by health personnel 2005-06 99.4 27.2 41.2
large nursing homes, corporate hospitals, diagnostic centres and
%children 12-23 months fully immunised 2005-06
pharmacies (Jesani and Anantharaman 1990; Nandraj 2000; Source: (1) Central Bureau of Health Intelligence, www.nrhm.nic.in accessed on 6 M
Baru 2005). The informal practitioners constitute the largest pro Ministry of Health and Family Welfare, CBHI (2004).
(2) HPS (2003). India Facility Survey, RCH-RHS.
portion in terms of numbers and spread, and provide primary
level services in rural and urban areas (Narayana 2006; Rhode services in the rural and urban areas and across states
and Vishwanathan 1995). The secondary level consists of small are pronounced in terms of infrastructure, human
and large nursing homes that are owned by mostly physician supplies, bed-population ratios and spatial distributio
entrepreneurs and provide outpatient and inpatient services. The institutions. The interstate variations are best illu
majority of these are small institutions, with 85% having less comparing the state of Kerala with that of up; the f
than 25 beds. Tertiary specialty and super-specialty private insti among the best and the latter the worst indicator
tutions comprise only i%-2% of the beds in private sector institu service development and health outcomes (Table i).
tions. They include large specialist hospitals promoted by mostly In spite of the rapid rise in private provisioning of h
big business groups and managed as corporate entities. The Kerala over the past two decades, the relatively bette
secondary and tertiary hospitals are largely skewed towards ing of phcs and the much higher health status in com
urban areas and developed states (goi 2006). The distribution other states of India is essentially due to the inves
of private sector facilities between states Figure 3: Full Immunisation Rate*, Inequities
provisioning
in of basic services by the state
Utilisation of Preventive Care
and regions is even more unequal than Full immunisation (%) government. Studies on Kerala have fur
those in the public sector. This reflects the 0 20 40 60 80 ther highlighted the role of the state in in
tendency to concentrate on better-off states Lower vesting in
quintile ^social development,
24.4 j even
I at low
and regions within them (Bhat 1993,1999; levels of per capita income, and achieving
Baru 2005). Scheduled tribe 31.3
improvements j
in the health, which are com
Uttar Pradesh HiS23
parable to those in middle- and high-income
3 Inequities in Access to countries (Dreze and Sen 1996). up, on the
All India (1992-93) 135.5
Health Services other hand, has a persistence of high pov
Rural 38.6
It is well known that reduction in mortality
and morbidity is partly due to preventive
II
Scheduled castes ! ? 39.7
erty levels and poor health services and so
cial development.
and curative interventions by public health
services. The availability of these services All India (2005-06) ^ H 43.5 j Inequities in Utilisation of
" ! ? Preventive Services
Urban ^mmmmMmmmmmmmmmmi 57.6
is, however, uneven across Indian states be
" !
cause of differences in infrastructure, hu Highestquintile ^^^^^^^^^^^^^^^^^171
The utilisation of preventive services such
as childhood immunisation and anc are
man resources, supplies and spatial distri
bution. In this section we describe the bar
Kerala ^ i 75.3
Mothers with more ^^^^^^^^^^^^^^^^^ effective indicators for assessing the avail
riers to equity and universality in terms of than 12 years
education ! ' of ^HHHHL^HLSplH 752
ability, accessibility and quality at the pri
inequities in availability, utilisation and mary level of health services provisioning.
* Full immunisation includes Bacillus Calmette-Gue>in (BCG against
tuberculosis), measles, and three doses each of diphtheria, pertussis
affordability of healthcare. (whooping cough) and tetanus (DPT) and polio vaccine (excluding The overall indicators for full immunisa
polio vaccine given at birth).
Source: (1) HPS and Macro international (2007), NFHS 3 2005-06: tion are poor in India with variation across
Availability of Care: Inequalities are per
India Voll.
rural and urban areas; states and socio
(2) http://www.nfhsindia.org/factsheet.html accessed on
vasive in the availability of public health 30 September 2009. economic groups (Figure 3).
Economic & Political weekly Q3S3 September 18, 2010 vol xlv no 38 51
This content downloaded from
139.167.49.154 on Sun, 26 Nov 2023 13:40:47 +00:00
All use subject to https://about.jstor.org/terms
SPECIAL ARTICLE -_______ _______ ________-- - - : - :-X- -
The all-India average for full immunisation coveragehigher
show a slightly for the
level of utilisation of
year 2005-06 was 44%. The rural-urbanthedifferential was substan
all-India average, whereas poorer states
Bihar
tial, with a coverage rate of 39% among and up
the rural show
and 58% lower
in the levels of utilisat
urban populations. There has been only an 8%
public improvement in
level.
coverage between 1992-93 and 2005-06.Hospitalisation
A comparison presents
of Kerala
a mixed picture.
and up illustrates the interstate variations. The overallfor
better infrastructure full
public services, such
immunisation coverage for Kerala is Punjab
75.3% with a rural-urban
and Haryana show higher privat
However,
differential of about 17% (69.4% rural inurban).
and 87.5% some other
While states, such as
in the case of up, it is only 22.9% with West Bengal, differential
a rural-urban Rajasthan and the north-eas
of about 12% (20.5% and 32.6% rural dependence on the public sector is evide
and urban, respectively).
up showed an increase of 11.6% in full immunisation
private facilities, coverage
cost and quality of servi
from 1998-99 to 2005-06, while Kerala variations (ibid).
showed a drop in coverage
from 80% 1998-99 to 75% in 2005-06. Reports have indicated
that Kerala has been facing financial and humanof
Affordability resource
Health Services: Affordabi
constraints in the public health services,
is determined
which havebyadversely
the cost of treatment,
affected the coverage in the state (Achutha Menon
manage these Centre
costs, andofits impact on th
Health Sciences 2005). holds (Gilson et al 2007). In India, oop pay
While the all India immunisation coverage is low (44%),
portionately there
large component of total he
is considerable variation across socio-economic
expenditures groups. The payments for co
include direct
testing,
coverage in the highest income quintile (71%) ismedicines andthat
three times transportation. Indir
in the lowest quintile (24.4%). There
ofisearnings
a substantial
due to gap
the in
illness, are not inclu
immunisation coverage between theexpenditures.
sts (31.3%) and
It is others
estimated that 80% of to
(53.8%). Although there has been some and
improvement
97% of private
in coverage
expenditure are borne t
from 26% in 1998-99 to 31% in 2005-06(goi
for2006).
the sts and
The from component
largest 47% of oop e
purchase
to 53.8% for others, the gap has not narrowed of medicines.
significantly acrossEstimates from
these two groups. Survey (nss) for 1999-2000 shows that 70
penditure
All India rate for receiving full anc stood inof
at 51% urban and
women in77% in rural are
cines
2005-06, with a rural-urban differential (Sakthivel
of 43% 2005).
and 74%, respec
Adverse
tively. An imperceptible increase in anc coveragesocio-economic
was reported: differential in
from 43.9% in 1992-93 to 44.2% in 1998-99; an increase
exhibited to 50.7%
by the fact that the poorest rur
of oop
was seen in 2005-06. For Kerala, the overall expenditure
figure was 94% on medicines, wherea
with
expenditure
a rural-urban coverage of 92% and 97%, for
respectively. the richest
Similar to urban quin
the case of full immunisation coverage, a slight
smaller decline
at 65% (Gargin anc
and Karan 2005). In th
riskfrom
coverage has also been reported in Kerala: protection, the high oop expenditur
99% in 1998-99
quintiles
to 94% in 2005-06. In up, the overall figure for adversely. Based
2005-06 was at a on estimates for
low of 26%, with the rural-urban differential of 23%expenditure
ing for health and 41%, due to oop pay
3.5%
respectively. Data across all states show of the population,
an upward or 35 million peop
trend in anc
erty the
coverage, with some notable decline among linetop
(Dreze and Sen 1996). A slight u
performers,
such as Kerala. served from the estimate made in 1999-200
million people, fell below the poverty line
Inequities in Utilisation of CurativeBonu
Services
et al 2007).
The evidence for recent years shows a high (80%) dependence on
Inequities
the private sector for outpatient care, which in Health
is largely Expenditure
due to the Burd
consumption
weakness in the delivery of public health of 2005).
services (Rao healthcare
In is higher in t
2004, a mere 21% of people in ruralurban population.
and 19% in urban This apparent anomaly
areas
people
utilised the public sector for outpatient living in
services. towns for
Figures and cities have bett
inpatient treatment were 42% and 38%private
in ruralservices compared
and urban areas, with those in r
respectively (nsso 2005). For inpatientfore,
care,experience
from a 60% a higher
utilisa financial burd
tion of public services in the 1980s, the healthcare. Summarising
rural and urban utilisation the 2004-05 nsso
data, 6.6%
rate has fallen to 42% and 38%, respectively. of utilisation
As the household of consumption exp
inpatient public services decreases withhealth in rural
an increase and
in the 5.2% in urban areas,
income
quintiles, in the absence of a strong corresponding
public sector,figures of 5.4% and 4.6% in 19
the poorer
In the 60th round of nss (2004-06), the a
groups are the most severely affected (ibid).
expenditure
Interstate variations occur in the utilisation on outpatient
of public services care per treated
for outpatient treatment. Kerala andwas nearly
Tamil 20%
Nadu, of total
which havehousehold consu
whereas
better developed and administered services theprimary
at the corresponding
level, percentage for
52 September i8, 2010 vol xlv no 38 GEES Econo
This content downloaded from
139.167.49.154 on Sun, 26 Nov 2023 13:40:47 +00:00
All use subject to https://about.jstor.org/terms
SPECIAL ARTICLE
at about 13%. With indirect costs and income loss for that period poorest consumption s
due to illness are added, the proportion is close to 33% in rural 20% for the rest of the
and 17% in urban areas. Thus, the expenditure burden of what tion size class. Thus, th
may be called "day-to-day morbidities" (reference period of tion is substantial for n
15 days) is very high, particularly in the rural areas. The burden Figure 5: Burden of Direct Heal
of expenditure for hospitalisation (reference period of one year) Inpatient
35
Treatment in Rural Ar
is almost of the same order as outpatient care. In rural areas, the
CD
burden of direct expenses alone is approximately 18%, being
slightly higher in urban areas.
Figure 4: Health Spending as Percentage of Household Consumption Expenditure
6.61
00
10
0.225 225-255 255-300300-340 340-380380-420 420-470 470-525 525-615 615-775 775-950 950+
mpce class
Source: NSSO 2006.
This trend holds true for outpatient care in the urban areas.
The expenditure burden is very high for the poorest two size
classes; it stays at around 15%-i6% for all but the two richest size
classes. The pattern is different for inpatient care. The expendi
ture burden is very high for the poorest two classes and the three
Rural Urban
richest size classes. The high burden for the richest sections is
Source: NSSO Surveys of Consumption Expenditures 50th, 55th and 60
because they use private (mostly tertiary) and corporate hospitals
In order to capture the
on a significant inequities
scale where and
the cost of care is very high compared bu
with other rungs of the private and public sector
expenditure across consumption (Figure 6).
classes, we
an analysis based onFigure
the 6oth
6: Burden of Direct Health Expenditure onround of the
the Household for Outpatient and
Inpatient Treatment in Urban Areas (2004)
has included households that sought treatm
and inpatient care in rural and urban areas
expenditure incurred. The expenditure in
and indirect expenses, as commonly catego
economics literature.
The formula used for computing the burden
penditure is as follows:
For the consumption size class i, the burden
is the average health-related expenditure du
reference (15 days for non-hospitalised ailmen
0.300 300-350 350-425 425-500 500-575 575-665 665-775 775-915 915-1120 1120-1500 1500-1952 1925+
hospitalised cases) person. C per indisposed
mpce class
Source: NSSO 2006, NSSO 2005.
all consumption expenditure per household
sponding period. Sources of Financing Healthcare: Analysis of data from the nss
shows
Based on the analysis wethat the find
high burden of expenditure
thaton the healthcare, isburde
expenditure across largely financed through two major sources:
consumption (a) household's own show
classes
While the poorer resources, and (b) borrowings.
sections carry In rural areas, close to a fifth of
a higher bur
the better-off, this the health expenses for
burden is outpatient
quite care is financed
heavythrough bor for
consumption classes. rowing;
Total the corresponding
directpercentage for hospitalisation
health-relat is much
percentage of higher at around
household 40% (nsso 2006). The recourse to borrowing,
consumption expend
care in rural areas is while
the being substantial
highest, even in the urban areas,
at is ofaround
a lower or 3
consumption size der compared
class. to the rural areas. The reliance it
However, on borrowing is
decline
staying around 25%, significantly
for higher the for thenext
poorer sections of the population out
seven
size classes. It is compared to the better-off
important to withnote
sharp differentials,
that especially in the f
tion size classes urban areas
account (nsso 2006).60%
for of the popul
The corresponding Several of these observations
burden measure are corroborated by a for
study of inp
areas is even more 482 poor households in
striking. While this burden Udaipur, Rajasthan which showed that i
Economic & Political weekly E353 September 18, 2010 vol xlv no 38 53
This content downloaded from
139.167.49.154 on Sun, 26 Nov 2023 13:40:47 +00:00
All use subject to https://about.jstor.org/terms
SPECIAL ARTICLE _ _
nearly 29%
atof the ho
creating
major source of
absencefina
of
with the reality
trolled that
in t
rising, the poor ofte
variation
consumption levels
between of
th
2007). Thus, illness
cost in o
pub
terious consequences
the private
ishment of the hous
caesarian se
is Rs 1,792
4 Factors even
Affectin
for d
The previous
Rs section
19 in th
utilisationsector
and (Ra
affor
discuss Unregulat
five key healt
to health services.
nology an T
public impact
sector; on
variable
unregulated commer
provisionin
forms; providers'
and lack of ac
know-how
Insufficient Invest
the largest
The low unfavourab
public investm
has been a1993; Sund
significan
tion of Narayana
public servic
low compared
The with
recent
and the and Regul
governmen
bilateral and multila
governmen
lowest forfor servic
countries
over a level care
three-year avr
$0.80, the istry
correspon
and m
total per capita
is a heal
propos
ures, along with
ing ext
good pr
the poorer African
conducting
Government
and spendi
legalis
Assay
penditure, is (elisa
among
due to currently
federalism, la
duce use, quality
variability in av
The long-standing
been w
formu
partly includes
responsible a
f
tor, for and
the
latory pu
Aut
panded byvisioning,
drawing
resources from
tary sub
state
with driven,
public wh
appoin
offering works
tax in se
concess
infrastructural facil
providers,
clinics, in
Unregulated
such Comm
legisl
lated not been f
commercialisa
medical and paramed
and cost Health
of Sec
healthcar
the the period
variability in p
cost and health sect
technical qu
the introduced
largest segment o
an adverseto improve
impact on
et al 2001; were
Kamatintro
200
1995; part
Nandraj of the
2007;
The during
problems arethe
sim
few user
initiatives fees,
for r
54 Septemb
This content downloaded from
139.167.49.154 on Sun, 26 Nov 2023 13:40:47 +00:00
All use subject to https://about.jstor.org/terms
SPECIAL ARTICLE
private sector, decentralisation and public-private partnerships staff and facility amenities. Several studies have commented on
were introduced (Duggal 2005). The evidence on the experience the variable quality of public services due to lack of adequate
of the introduction of user fees in the public sector across states is infrastructure, human resources and indifferent behaviour of
somewhat mixed in terms of impact on levels of utilisation. In public employees (Rao et al 2005; goi 2006). The recent plan
some states, for example, Andhra Pradesh, utilisation of the public documents have acknowledged these as constraints on the qual
sector has improved after health sector initiatives were put in ity of care provided by the public sector (goi 2006).
place (Shariff and Singh 2002). However, the available evidence More recent surveys and studies also show that people are not
shows that user fees have tended to exclude the poorest, despite satisfied with public services and highlight the lack of infrastruc
efforts to ensure that those below the poverty line are exempt ture and indifferent and rude behaviour of personnel as impor
from paying user charges (Garg and Karan 2005). International tant reasons for not using public services. According to the nsso,
experience also corroborates the findings from India and shows "not satisfied with medical treatment" ranks as the primary rea
that even a small user fee charge can exclude the poor from utilis son in both rural and urban areas. This is followed by "lack of
ing health services (Hola and Kremer 2009). availability of services" in rural, and "long waiting" in urban areas.
Not all reform initiatives in health have been led by the World Similarly, the latest nfhs shows that the perception of "poor
Bank. Prominent among the state-led is the Tamil Nadu Medical quality of care" is the most important reason across selected
Supplies Corporation (tnmsc) that has been successful in states. The survey itself does not provide insight into what the
streamlining drug procurement, distribution and controlling determinants of quality are in health services. A recent study
showed that determinants of quality include clinical and inter
costs of medicines in the public services. The Tamil Nadu model
is being adapted by several states in India for ensuring a proper personal dimensions and these influence the choice and utilisa
supply of drugs in the public services. In 1995, the Tamil Nadu tion of anc (Rani et al 2007).
government adopted a list of essential drugs to be provided The assumption that private services offer superior quality of
through the tnmsc. services is not adequately supported by any hard evidence. While
tnmsc, designed and funded entirely by the state government some private sector facilities offer good quality services, this
is responsible for the purchase and distribution of essential drugs cannot be generalised because of the heterogeneity of facilities,
in the public health services. This ranges from tasks that include personnel and their practices. Evidence from micro studies is
identifying suppliers who monitor appropriate storage of drugs in revealing. Private care practitioners along with public care prac
warehouses and its appropriate distribution, tnmsc has laid strict titioners, for example, in Delhi, are more skilled and knowledge
and elaborate procedures to ensure an uninterrupted and quality able in the wealthier areas in comparison to the poorer area
supply of medicines. A drug committee identifies the list of essential (Das and Hammer 2007). Informal practitioners adopt irrational
drugs. It consists of professors of medicine, clinicians in various practices in prescribing medicines for the treatment of communi
medical fields, pharmacologists, a representative from the World cable diseases like malaria, diarrhoea, tuberculosis and fevers
Health Organisation, health secretary and the managing director (Banerjee et al 2004; Uplekar et al 2001; Kamat 2001). Such prac
of tnmsc. All government healthcare institutions and pharma tices are also evident in infertility care services and childbirth
cists are given the list of essential drugs. Thereafter, local health (Unisa 1999). In case of obstetric care, a study of informal practi
officials can request the committee to modify the list in accordance tioners in western Uttar Pradesh shows inappropriate use of
with their local needs. The drugs allocated to phcs are limited to oxytocin to speed up labour in women during home deliveries
54 essential drugs, tnmsc invites tenders by advertising in the (Jeffery et al 2007). These practices are not only inappropriate,
print media, including pharmaceutical trade journals and its but dangerous for maternal health as it results in serious postpar
own web site, with clear guidelines for supplier selection, quality tum complications and related morbidities.
control and distribution. The committee pays the supplier only At the secondary level, a study of private hospitals in Chennai
after receiving a report on quality control. A detailed system of revealed that this sector has grown without any norms for infra
warehousing the drugs and accounting by the health centre are a structure, with a strong tendency to over-provide care, depending
part of the procurement policy (Lalitha 2005 and 2007). on the patients' ability to pay (Muraleedharan 1999). Another
study in rural in Maharashtra revealed that only 55% of private
Variable Quality of Care in Public and Private Sectors: Common sector institutions had registration, only 38% maintained any
complaints against public care cited in the recent nsso (2006) kind of records, and that a remarkably high proportion lacked
and nfhs (1998-99 and 2005-06) include: "Not satisfied with basic facilities. This study showed that close to 30% were being
medical treatment", "lack of availability of services", "long wait run by doctors not trained in the allopathic system of medicine.
ing times", "poor quality of care", and poor interpersonal interac They were being run without adequate facilities and human
tions. Additionally, assessment of the public sectors underscore power, with only 2% employing trained nurses. Only 10% of
poor technical competence, poor accessibility to services, inade hospitals had an ecg monitor, 655 a steriliser and 56% an oxygen
quacy of drugs and supplies, poor staff availability, and poor cylinder (Nandraj and Duggal 1997). Yet another study found
quality and amenities (Rao et al 2005). that caesarean sections were performed three times more in
The quality of health services is dependent on a number of private hospitals than public ones (Homan and Thankappan
factors related to technical competence, accessibility to services, 1999). The extent of variability and lacunae that several of these
interpersonal relations and presence of adequate drugs, supplies, studies have observed in infrastructure, basic facilities, human
Economic & Political weekly [3353 September 18, 2010 vol xlv no ^8 55
This content downloaded from
139.167.49.154 on Sun, 26 Nov 2023 13:40:47 +00:00
All use subject to https://about.jstor.org/terms
SPECIAL ARTICLE =- :_ -= _-_ -__ __ __ __
resources and medical
and equipment
regional inequ
private sector asjority
well. of those wh
Problems in the formal
to private
preventive s
and
physicians tend 2007;
to Peters et
over-prescribe al
ca
to pay; a lack ofMahal et al
registration2002)
proc
inadequate and cultural
infrastructure with barr
poor
(Nandraj and marginalised
Duggal 1997). A gro
com
is that
over-prescription untreated
of mo
medicines, d
Studies on Rural
informal versus urb
practitioners in
they often lack forward castes;
qualifications andan
a
scribing ones.
medicines for Women
the bel
treatmen
access to healthca
Lack of Accountability
to the in
other Pub
cast
regulatory and hps 2007, Rani
institutional et
mech
ability to consumers of health se
both the public 5 Equity
and private Enhan
sector
sector that lack The Health Policy
accountability are
different expressed
behaviour of concern
service provi
sector is prone to the overuse
sioning, use and
and he
ethical practices by the
and nth is
there Plan d
very
have shown that the link
there is between
a high ra
cal and of
paramedicalpublic provision
personnel in t
absence rates are
ingmuch
in higher
order to en
doctors than sector;
health concern
workers ab
and
the secondary orpoor and
tertiary the non-
levels (C
Apart from alised sections,
absenteeism it is es
wel
tion in the cerns
public have
health been
services. ra
P
terms of bribes decades
demandedthrough
for adm
institutions. women's
Corruption groups
is also th
rif
and transfer of ductive technolog
personnel; admissi
education; procurement
ning of drug
irrational an
2005). Drug
Corruption is Action
not Netw
restricted
privatesector broad
also has alliance
its sharefor
of
ethical of
practices. the
There Jan
is a Swast
well-
commissions whengovernmental
doctors refer or
pa
the private concerns
sector. of
Similarly, equity
the ph
their campaigned
representatives offer a for t
varie
prescribing 2008).
specific Under of
brands themf
Phadke 1998; Human
Baru Rights
1998, 2002). Co
W
in public hearings,
subsidies to the called
private
there are reportsSwasthya
of Abhiyan
non-complianc
by corporate care to
hospitals. individual
While the lack private
of health ser
accountability
known, the als,
private academics,
sector is not ng
an
are fewer highlight
checks on their the inad
account
The role of ceedings
consumer of
groups the
in er
limited. An ministers
example of and
an sen
effe
groups was when government-led
they drew b
att
cases of medicalcommunist
negligence and
in s
th
were registered aged
with to put
the pressu
consume
given for axes
medical of inequities
negligence in th
lic and private health
practices services.
are permiT
times, only as a voted into
referral power
portal for
Common Minimu
Barriers for This led
Marginalisedto the fo
Populat
in the Indian (nrhm),
health launched
services hav
56 September 18, 20
This content downloaded from
139.167.49.154 on Sun, 26 Nov 2023 13:40:47 +00:00
All use subject to https://about.jstor.org/terms
_ . _ _ _ _ ________. .=_______ _ __=. ____. _ .=A_ __ _ _ _ _ _ _ARTICLE
The nrhm is a large, centrally-driven programme of the(1) Given the number of programmes that are focusing on t
govern
poor like
ment which has tried to address some of the key inequities and socially marginalised, the need arises for enhanc
underinvestment in financing, human resources, infrastructure
public investments and greater synergies at different levels of
and some aspects of quality in the public sector. It has also
plementation
initi within and across ministries.
ated several measures for accountability such as political
(2)checks
Comprehensive regulation of the public and private sectors
required in provisioning, medical technology and pharmaceutica
and balances, administrative procedures and auditing (Dasgupta
and Qadeer 2005; Shukla 2005). This is critical for controlling costs and improving quality
Many of the strategies focus only on the public sector, while
accountability. Provider behaviour, an essential component of qu
the role of the private sector and its regulation is poorly ity and accountability, requires innovative approaches that perm
denned.
Its focuses on rural areas and less developed states as aa greater
step to voice in monitoring performance to beneficiary comm
nities and their representatives. For the private sector, accounta
wards bridging rural-urban and inter- and intra-state inequities
ity can
in the availability of health services. The review of the nrhm hasbe assured by a combination of legislation, involvement
shown that there are interstate variations in the uptake of the
professional organisations, consumer rights groups and public
programme and there are serious gaps in the availability, deploy
tion. The way forward in the public sector could be the implem
tation of the Indian Public Health Standards and a combination
ment and retention of medical and paramedical personnel.
In response to the high out-of-pocket expenditure onincentives
health and disincentives to induce greater sensitivity and
services and the increasing burden on the poor andcountability
socially of providers at the panchayat or the municipality lev
marginalised, the government has initiated an insurance(3)
scheme,
New and innovative systems of monitoring performance a
evaluating
Rashtriya Swasthya Bima Yojana (rsby). This is a hospital insur progress towards equitable health outcomes need
ance scheme for families below the poverty line as a protection
be introduced. It would be worthwhile, for instance, to adopt
idea of institutionalising a health equity gauge, that helps
from catastrophic expenses. While this is an important protective
track
measure for those below the poverty line, our analysis on inequities, similar to that initiated in South Africa a
burden
of health expenditure across consumption groups showsadopted
that the
by a few middle- and low-income countries at the centr
and state levels. Another innovative initiative is seen in the c
burden is quite substantial for even the rest of the population.
of Health Councils in Brazil that have institutionalised health
6 The Way Forward sues as a primary policy concern both at the local and nation
In order to address the persistence of inequities in health
levelsand
as a citizen's right (Equity Guage 1999). The present g
ernment
access to health services in India, we identify four key areas that can build further on the steps they have started, a
require urgent attention and actions. address inequalities in availability, utilisation and affordabi
withspon
Most of the equity enhancing programmes are centrally greater seriousness, as well as a courtship of democra
voices and the rules of deliberative democracy (Gutman
sored, time bound and vertical interventions. They are sponsored
Thompson 1996; Daniels 2008; Bonu et al 2007).
and implemented by separate ministries with little coordination
let alone synergies between programmes. There has been
(4) aHealth
ten security in India needs to become an urgent nation
dency for these newer initiatives to target the socially and
marginal
political priority. Rapid improvements in health are need
ised and those below poverty line. Our analysis of burden
not of ex to accelerate and sustain India's economic growth; they
only
penditure shows that while the poorest are v/orst affected, the
also fundamental to India gaining recognition as a distinguish
burden is substantial even for the middle quintiles. This holds
middle-income country with improved standards of living and
true for outpatient and inpatient care in rural and urban areas.
duced levels of human deprivation. Focusing on health equity w
This raises concerns regarding targeted approaches that focus to enhancing human capabilities and advancing t
be critical
only on poorest, but argues for universal access to health progress
services. of Indian society over the next decade.
REFERENCES of the Poor", Journal of Economic Perspectives, India, Health Policy and Planning, 8(1): 43-56
Acharya, Sanghmitra (2010): "Caste and Patterns 21(1), 141-67. (London: Oxford University Press).
of Discrimination in Rural Public Health CareBanerjee, A, A Deaton and E Duflo (2004): "Wealth, - (i999): Characteristics of Private Medical Practice
Services" in Sukhdeo Thorat and Katherine S Health and Health Services in Rural Rajasthan", in India: A Provider Perspective: Health Policy and
Newman (ed.), Blocked by Caste-Economic Dis American Economic Review, Vol 94(2), pp 326-30. Planning (London: Oxford University Press).
crimination and Social Exclusion in Modern India
Banerji, D (1985): Health and Family Planning Services Bloom G, B Kanjilal and D H Peters (2008): Regulating
(Delhi: Oxford University Press), pp 208-29. in India: An Epidemiological, Socio-cultural and Health Care Markets in China and India, Health
- (2002): "Health Care Utilisation in Rural North Political Analysis and a Perspective (New Delhi: Affairs, Vol 27, No 4, pp 952-63.
India - A Case of Nirpura", District Meerut, Lok Paksh). Bonu, S, I Bhushan and D H Peters (2007): "Incidence,
study undertaken as part of the Monitoring Baru, R (1998): Private Health Care in India: Social Intensity and Correlates of Catastrophic Out-of
Shifts in Health Sector Policy in Sough Asia Characteristics and Trends (New Delhi: Sage Pub Pocket Health Payments in India", ERD Working
Project, Unpublished repot. Centre of Social lications). Paper No 102, Asian Development Bank, October;
Medicine and Community Health, School of - (2002): "Health Sector Reform: The Indian Expe Manila, Philippines.
Social Sciences, Jawaharlal Nehru University, rience" in A Twaddle (ed.), Health Care Reform CBHI (2004): Central Bureau of Health Investigation,
New Delhi. Around the World (Connecticut: Auburn House). Ministry of Health and Family Welfare, www.
Achutha Menon Centre of Health Sciences (2005): - (2005): "Private Health Sector in India: Raising nrhm.nic.in, accessed on 6 March 2009.
"Current Status of Services Delivery in the Health Inequities" in L V Gangolli, R Duggal, Abhay Chaudhury, N, J Hammer, M Kremer, K Muralidharan
and Family Welfare Sector in Kerala", Sri Chitra Shukla (ed.), Review of Health Care in India and F H Rogers (2006): "Missing in Action: Teacher
Tirunal Institute of Medical Sciences, Thiru (Mumbai: Centre for Enquiry into Health and and Health Worker Absence in Developing Coun
vananthapuram, January. Allied Themes). tries", Journal of Economic Perspectives, 20(1),
Banerjee, A and E Duflo (2007): "The Economic Lives Bhat, R (1993): Public-Private Mix in Health Care in pp 91-116.
Economic & Political weekly EHB3 September 18, 2010 vol xlv no 38 57
This content downloaded from
139.167.49.154 on Sun, 26 Nov 2023 13:40:47 +00:00
All use subject to https://about.jstor.org/terms
SPECIAL ARTICLERTCLE==
Claeson, M, E R Bos, T Mawji and Pathmanathan Iyer, A, G Sen and A George (2007): "The Dynamics of Ministry of Health and Family Welfare, Govern
(2000): "Reducing Child Mortality in India in the Gender and Class in Access to Health Care: ment of India, New Delhi.
New Millennium", Bulletin of the World Health Evidence from Rural Karnataka, India", Inter OECD (2008): Organisation for Economic Cooperation
Organisation, 78:10. national Journal of Health Services, 37(3): 537-54. and Development, data base http://www.oecd.
Daniels, N (2008): Just Health (New York: Cambridge Jeffery, P, A Das, J Dasgupta and R Jeffery (2007): org/dataoecd/62/8/38o84666.pdf accessed on
University Press). "Unmonitored Intrapartum Oxytocin Use in September.
Das, J and J Hammer (2007): "Money for Nothing: The Home Deliveries: Evidence from Uttar Pradesh, Peters, D H, A S Yazbeck, R Sharma, G N V Ramana,
Dire Straits of Medical Practice in Delhi, India", India", Reproductive Health Matters, 15(30), 172-78. L H Pritchett and A Wagstaff (2002): Better Health
Journal of Development Economics, 83, pp 1-36. Jesani, A and S Anantharaman (1990): "Private Sector Systems for India's Poor: Findings, Analysis and
Dasgupta, M (1987): "Selective Discrimination against and Privatisation of Health Care Services: A Re Options (Washington DC: World Bank).
Female Children in Rural Punjab", Population and view Paper" for the ICSSR-ICMR joint panel on Phadke, A (1998): Drug Supply and Use: Towards a
Development Review, 13(1): 77-100. health, Foundation for Research in Community Rational Policy in India (New Delhi: Sage).
Dasgupta, R and I Qadeer (2005): "The National Rural Health, Mumbai, August. Qadeer, I, K Sen and K R Nayar (2001): Public Health
Health Mission (NRHM): A Critical Overview", Kamat, V (2001): "Private Practitioners and Their Role and the Poverty of Reforms: The South Asian
Indian Journal of Public Health, Vol XXXXIX, No 3, in Resurgence of Malaria in Mumbai and Navi Predicament (New Delhi: Sage Publications).
July-September. Mumbai, India: Serving the Affected or Aiding an Rani, M, S Bonu and S Harvey (2007): "Differentials
Deaton, A and J Dreze (2009): "Food and Nutrition in Epidemic?", Health Policy and Planning. in the Quality of Ante Natal Care in India", Inter
India: Facts and Interpretations", Economic & Lalitha, N (2005): "Essential Drugs in Government national Journal for Quality in Health, pp 1-10.
Political Weekly, 44: 7, pp 42-45. Health Care: Emerging Model of Procurement and Rao, S (2005): "Delivery of Services in the Public Sector:
DFID (2002): "Study of the Dynamics and Structure of Supply", Working Paper No 61, Gujarat Institute Financing and Delivery of Healthcare Services in
Private Health Care in Madhya Pradesh", of Development Research, Ahmedabad, September. India", National Commission on Macroeconomics
Department for International Development, India - (2007): "Government Intervention and Prices of and Health Background Papers, Ministry of Health
and Government of Madhya Pradesh, New Delhi. Medicine: Lessons from Tamil Nadu", Working and Family Welfare, Government of India, New Delhi.
Dreze J, A Sen, ed. (1996): Indian Development: Se Paper No 175, Gujarat Institute of Development Rao, S, M Nundy and A S Dua (2005): "Delivery of
lected Regional Perspectives (New Delhi: Oxford Research, Ahmedabad, July. Health Services in the Private Sector: Financing
University Press). Mackintosh, M (2001): "Do Health Care Systems Con and Delivery of Health Care Services in India",
Duggal, R (2005): "Public Expenditures, Investment tribute to Inequalities?" in D Leon and G Walt (ed.), National Commission on Macroeconomics and
and Financing under the Shadow of a Growing Poverty, Inequality and Health: An International Health Background Papers, Ministry of Health and
Private Sector" in L Gangolli, R Duggal, A Shukla Perspective, (Oxford: Oxford University Press). Family Welfare, Government of India, New Delhi.
(ed.), Review of Health Care in India, Centre for Mahal, A, J Singh, F Afridi, V Lamba and A Gumber Ravindran, S (2000): "Engendering Health", Seminar,
Enquiry into Health and Allied Themes, Mumbai. (2002): Who Benefits from Public Health Spending 489.
Equity Gauge (1999): The Health Systems Trust 1999; in India - Results of a Benefit Incidence Analysis for RGI (2001): Census of India, Final Population Tables,
Durban. India, National Council of Applied Economic Re Office of the Registrar General of India, New Delhi.
Garg, C and A K Karan (2005): "Health and Millennium search, New Delhi. Priya, Ritu (2005): "Public Health Services in India: A
Development Goal 1: Reducing Out-of-Pocket Mahal, A, S Taman and A Varshney (2005): "Appropri Historical Perspective" in L V Gangolli, R Duggal,
Expenditures to Reduce Income Poverty-evidence ate Policies for Medical Device Technology: The A Shukla (ed.), Review of Health Care in India, Centre
for India", EQUITAP Project, Working Paper No 15, Case of India: Financing and Delivery of Health for Enquiry into Health and Allied Themes, Mumbai.
Institute of Health Policy, Colombo. Care Services in India", National Commission on Rhode, J and H Vishwanathan (1995): The Rural Private
Gilson, L, J Doherty, R Loewenson and V Francis Macroeconomics and Health Background Papers, Practitioner (New Delhi: Oxford University Press).
(2007): "Challenging Inequity through Health Ministry of Health and Family Welfare, Govern Sakthivel, S (2005): "Access to Essential Drugs and
Systems", Final Report, Knowledge Network on ment of India, New Delhi. Medicines: Financing and Delivery of Health Care
Health Systems, WHO Commission on the Social Mary Bhat, P N (2001): "Recent Trends in Fertility and Services in India", National Commission on
Determinants of Health, June. Mortality in India: Critical Repraissal of Data Macroeconomics and Health Background Papers,
Govender, V and Penn L Kekana (2007): "Gender Bi from Sample Registration System and National Ministry of Health and Family Welfare, Govern
ases and Discrimination: A Review of Health Care Family Health Surveys" in K Srinivasa and ment of India: New Delhi.
Interpersonal Interactions", June (Background M Vlassoff (ed.), Population and Development Sen, G, A Iyer and A George (2002): "Structural Reforms
Paper for the Women and Gender Equity Knowl Nexus in India - Challenges for the New Millennium, and Health Equity: A Comparison of NSS Surveys,
edge Network of the WHO Commission on Social Tata McGraw Hill, New Delhi. 1986-87 and 1995-96", Economic & Political Weekly,
Determinants of Health). Mclntyre, D, M Whitehead G Dahlgren and T Shenglan 6 April, pp 1342-52.
Gol (2006): Approach Paper to the Eleventh Five-Year (2007): "Equity Impacts of Neo-liberal Reforms: Shariff, A and Geeta Singh (2002): "Determinants
Plan, Planning Commission, Government of India, What Should the Policy Be?", International Jour of Maternal Health Care Utilisation in India:
New Delhi. nal of Health Services, Vol 37, No 4, pp 693-709. Evidences from Recent Household Survey",
Gwatkin, D R (2000): "Health Inequalities and Health Muraleedharan, V R (1999): "Characteristics and Working Paper 85, National Council for Applied
of the Poor: What Do We Know? What Can We Structure of the Private Hospital Sector in Urban Economic Research, New Delhi, February.
Do?", Bulletin of the World Health Organisation, India: A Study of Madras City", Small Applied Re Shukla, A (2005): "National Rural Health Mission:
78, pp 3-18. search Paper 5, Partnerships for Health Reform Hope or Disappointment?", Indian Journal of Public
Gupta, I, P Dasgupta (2007): "Choosing between Project, ABT Associates Inc, Bethesda. Health, Vol XXXXIX, No 3, July-September.
Private, Public and No Care" in A Shariff and Nandraj (2000): The Private Health Care Sector: Con - (2008): "Rereading the Alma Ata Declaration:
M Krishnaraj (ed.), State, Markets and Inequali cerns, Challenges and Options (Mumbai: Centre The Need to Say the Unsaid, to Do the Undone",
ties: Human Development in Rural India (New for Enquiry into Health and Allied Themes). Global Social Policy, 8, pp 164-66.
Delhi: Orient Longman). Nandraj, S and R Duggal (1997): Physical Standards in Subramanian, S V, S Nandy, M Irving, D Gordon,
Gutman, A and D Thompson (1996): Democracy and the Private Health Sector: A Case Study of Rural H Lambert and G D Smith (2006): "The Mortality
Disagreement (Cambridge, MA: Harvard Univer Maharashtra, Centre for Enquiry into Health and Divide in India: The Differential Contributions of
sity Press). Allied Themes, Mumbai. Gender, Caste and Standard of Living across the
Hart, T J (2000): "Commentary-Three Decades of the Narayan, T (2008): "Alma Ata and Social Move Life Course", American Journal of Public Health,
Inverse Care Law", British Medical Journal, 320 ments", Global Social Policy, 8:158-61. 96, pp 818-25.
(7226): pp 18-19. Narayana, K V (2006): "The Unqualified Medical Sundar, R (1995): Household Survey of Healthcare
Hola, A and M Kremer (2009): "Prices and Access: Practitioners: Methods of Practice and Nexus Utilisation and Expenditure National Council for
Lessons from Randomised Evaluations in Educa with Qualified Doctors", Working Paper No 70, Applied Economic Research", Working Paper No 53,
tion and Health, Centre for Global Development", Centre for Economic and Social Studies, Hyderabad. New Delhi.
Working Paper No 158. NSSO (2006): "Morbidity, Health Care and the Condi Unisa, S (1999): "Childlessness in Andhra Pradesh:
Homan, R K and K R Thankappan (1999): "An Exami tion of the Aged, National Sample Survey", 60th Treatment Seeking and Consequences', Reproduc
nation of Public and Private Sector Sources of Round (January-June 2004), Report N0507, Min tive Health Matters, 7(13), pp 54-64, May.
In-patient Care in Trivandrum District, Kerala", istry of Statistics and Programme Implementa Uplekar, M, V Panthania and M Raviglione (2001):
Achuta Menon Centre for Health Services, Thiru tion, Government of India, New Delhi. "Private Practitioners and Public Health: Weak
vananthapuram. Nayar, K R (2007): "Social Exclusion, Caste and Links in Tuberculosis Control", The Lancet, 358,
HPS (1995): National Family Health Survey (NFHS) Health - A Review Based on Social Determinants 9285, pp 912-16.
1992-93, Institute of Population Sciences, New Framework", Indian Journal of Medical Research, WHO (1978): Report of the International Conference
Delhi. (126), October, pp 355-63 an Primary Health Care, Alma Ata, USSR, 6-12
- (2003): India Facility Survey, RCH-RHS, Inter Nundy, M (2005): "The Not-for-Profit Sector in Medical September, World Health Organisation, Geneva.
national Institute of Population Science. Care in Financing and Delivery of Health Care - (2008): National Health Accounts, http://www.
HPS and Macro International (2007): National Health Services in India", National Commission on who.int/nha/country/en/index.html, World Health
and Family Survey - 2005-06 (NFHS 3), Mumbai. Macroeconomics and Health background papers, Organisation, accessed on May 2010.
58 September i8, 2010 vol xlv no 38 15321 Economic & Political weekly
This content downloaded from
139.167.49.154 on Sun, 26 Nov 2023 13:40:47 +00:00
All use subject to https://about.jstor.org/terms
You might also like
- Inequities in Access To Health Services PDFDocument10 pagesInequities in Access To Health Services PDFSaurabhPalNo ratings yet
- Draft Paper Ageing, Poverty and Social Security in Orissa: Some Issues and EvidencesDocument21 pagesDraft Paper Ageing, Poverty and Social Security in Orissa: Some Issues and EvidencesakmecoNo ratings yet
- Marital Status, Family Ties, and Self-Rated Health Among Elders in South IndiaDocument18 pagesMarital Status, Family Ties, and Self-Rated Health Among Elders in South IndiazoyaNo ratings yet
- Health and Mortality Status of Scheduled Tribes in IndiaDocument6 pagesHealth and Mortality Status of Scheduled Tribes in IndiaIjahss JournalNo ratings yet
- Dialogues in Health - PaperDocument9 pagesDialogues in Health - PaperMuraleedharan V R IITMNo ratings yet
- Improving Maternal Newborn and Child Health IndiaDocument10 pagesImproving Maternal Newborn and Child Health IndiaAtmajan PallipadNo ratings yet
- Determinants of Health Seeking BehaviourDocument26 pagesDeterminants of Health Seeking BehaviourArnab JanaNo ratings yet
- Socioeconomic Determinants of Infant Mortality Rate in IndiaDocument13 pagesSocioeconomic Determinants of Infant Mortality Rate in IndiaJyotiringa PuzariNo ratings yet
- Basic Characteristics of Indian Society: Lecture 4: Society and CultureDocument7 pagesBasic Characteristics of Indian Society: Lecture 4: Society and CultureJaf ShahNo ratings yet
- Child Health PatraDocument36 pagesChild Health PatraShamindra RoyNo ratings yet
- Assignment # Pre Mid-TermDocument5 pagesAssignment # Pre Mid-TermAryaman DubeyNo ratings yet
- Life Satisfaction and Well-Being at The Intersections of Caste and Gender in IndiaDocument15 pagesLife Satisfaction and Well-Being at The Intersections of Caste and Gender in IndiaLovis KumarNo ratings yet
- 3.isca Irjss 2013 135 PDFDocument5 pages3.isca Irjss 2013 135 PDFAnonymous Gj4wl21SNNo ratings yet
- Gender Inequality in The Light of Child Sex Ratio in India and HaryanaDocument10 pagesGender Inequality in The Light of Child Sex Ratio in India and HaryanaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Chapter - 2 Review of LiteratureDocument16 pagesChapter - 2 Review of LiteratureVeekeshGuptaNo ratings yet
- Anup Kumar MishraDocument11 pagesAnup Kumar MishraMahila Pratishtha JournalNo ratings yet
- Age of HealthDocument12 pagesAge of Healthsgirishri4044No ratings yet
- Andhra Pradesh Human Development Report 2007-c9Document18 pagesAndhra Pradesh Human Development Report 2007-c9Vivek GuptaNo ratings yet
- Employment Aging and Disease in IndiaDocument25 pagesEmployment Aging and Disease in IndiaYusuf AmriNo ratings yet
- Gender Analysis of Healthcare Expenditures in Rural NigeriaDocument13 pagesGender Analysis of Healthcare Expenditures in Rural NigeriaPremier PublishersNo ratings yet
- Written Public Health Ll. U2Document7 pagesWritten Public Health Ll. U2Adanigbo MagretNo ratings yet
- Graded Caste Inequality and PovertyDocument33 pagesGraded Caste Inequality and PovertyAmresh BindNo ratings yet
- CRPC AssignmentDocument7 pagesCRPC AssignmentsriprasadNo ratings yet
- Health Status of Rural Women in OdishaDocument10 pagesHealth Status of Rural Women in OdishaEditor IJTSRDNo ratings yet
- Health Status of Tribal Women in IndiaDocument33 pagesHealth Status of Tribal Women in Indiadon bossNo ratings yet
- Anderson Ray 2010 - Missing Women Age and DiseaseDocument40 pagesAnderson Ray 2010 - Missing Women Age and DiseaseEcon booksNo ratings yet
- JLS 10 01 081 18 186 Bhattacherjee C TX (9) .PMDDocument7 pagesJLS 10 01 081 18 186 Bhattacherjee C TX (9) .PMDChitradip BhattacherjeeNo ratings yet
- VulnerableDocument23 pagesVulnerableSaravana KadirvelNo ratings yet
- Changing Profile of Urban Poverty A Case Study of Jharkhand (India)Document14 pagesChanging Profile of Urban Poverty A Case Study of Jharkhand (India)Ramdayal ChoretiyaNo ratings yet
- Missing Women: Age and Disease: Siwan AndersonDocument39 pagesMissing Women: Age and Disease: Siwan AndersonB20111No ratings yet
- Health Equity in MyanmarDocument5 pagesHealth Equity in MyanmarHein Htet Aung100% (1)
- Prevalence and Potential Determinants of Chronic Disease Among Elderly in India: Rural-Urban PerspectivesDocument16 pagesPrevalence and Potential Determinants of Chronic Disease Among Elderly in India: Rural-Urban PerspectivesMadhu C KNo ratings yet
- Lecture 6: Society and Development: The Model of Inclusive GrowthDocument9 pagesLecture 6: Society and Development: The Model of Inclusive GrowthJaf ShahNo ratings yet
- Health Inequalities BLACHIRDocument13 pagesHealth Inequalities BLACHIRNewton O. OchiengNo ratings yet
- Elderly Women in KashmirDocument5 pagesElderly Women in KashmirEditor IJTSRDNo ratings yet
- Poverty and LOwer Hindu ND MuslimsDocument29 pagesPoverty and LOwer Hindu ND MuslimsParthiban S. GopalNo ratings yet
- Depressive Symptoms Among Women in Raqqa GovernoraDocument10 pagesDepressive Symptoms Among Women in Raqqa GovernoraAmmar ShakerNo ratings yet
- 3765dbde1a96580628d3d10 PDFDocument6 pages3765dbde1a96580628d3d10 PDFDari ThangkhiewNo ratings yet
- Social and Economic Status of Tribal Women in India: - The Challenges and The Road AheadDocument6 pagesSocial and Economic Status of Tribal Women in India: - The Challenges and The Road AheadkousikpaikNo ratings yet
- Ijcm 43 10Document4 pagesIjcm 43 10suvaran sagar bajpaiNo ratings yet
- ReviewDocument29 pagesReviewhilal ahmad mirNo ratings yet
- Origins of Ayurveda Have Been Traced To Around 6,000Document13 pagesOrigins of Ayurveda Have Been Traced To Around 6,000PriyankaNo ratings yet
- Miller 1998Document10 pagesMiller 1998Andri koko Perdana nilakandiNo ratings yet
- Vulnerable Groups in India-Status, Schemes, of India: ConstitutionDocument9 pagesVulnerable Groups in India-Status, Schemes, of India: Constitutionraja sekaranNo ratings yet
- 214-Article Text-1640-1-10-20230502Document6 pages214-Article Text-1640-1-10-20230502nusantaramedikasolusindoNo ratings yet
- Work Participation of Tribal Women in India: A Development PerspectiveDocument4 pagesWork Participation of Tribal Women in India: A Development PerspectiveInternational Organization of Scientific Research (IOSR)No ratings yet
- Horizon CommunityDocument12 pagesHorizon Communityclive muchokiNo ratings yet
- G01334850 PDFDocument3 pagesG01334850 PDFnilaNo ratings yet
- Status of Elderly in India - Ignited Minds JournalsDocument9 pagesStatus of Elderly in India - Ignited Minds JournalsAsad MajidNo ratings yet
- Changing Perspectives of Tribal Health in IndiaDocument4 pagesChanging Perspectives of Tribal Health in IndianageshNo ratings yet
- Gerontology in India: International SpotlightDocument7 pagesGerontology in India: International SpotlightNurul pattyNo ratings yet
- Sem 1Document1 pageSem 1Abdullah ScofieldNo ratings yet
- Cross SectionalDocument10 pagesCross Sectionaldzakiyatul fahmiNo ratings yet
- Women - Health - and - Sustainable Development - 1Document22 pagesWomen - Health - and - Sustainable Development - 1Suman PathakNo ratings yet
- Vol 57 (6), December 2020, p.327-335Document9 pagesVol 57 (6), December 2020, p.327-335librarianNo ratings yet
- SSM - Population Health: Rourke O'Brien, Tiffany Neman, Nathan Seltzer, Linnea Evans, Atheendar VenkataramaniDocument6 pagesSSM - Population Health: Rourke O'Brien, Tiffany Neman, Nathan Seltzer, Linnea Evans, Atheendar Venkataramanimandeep kaurNo ratings yet
- Tribal Population in India: A Public Health Challenge and Road To FutureDocument2 pagesTribal Population in India: A Public Health Challenge and Road To FutureMlbb GameplaysNo ratings yet
- IntroductionStatus of Tribal Women An Indian PerspectiveDocument5 pagesIntroductionStatus of Tribal Women An Indian PerspectiveGoswami AradhanaNo ratings yet
- Gender Inequality in India Causes and ReDocument5 pagesGender Inequality in India Causes and ReVasundhra SharmaNo ratings yet
- Indian Muslims: Struggling for Equality of CitizenshipFrom EverandIndian Muslims: Struggling for Equality of CitizenshipNo ratings yet
- NCM101 - Nursing AssessmentDocument4 pagesNCM101 - Nursing AssessmentTamara RomuarNo ratings yet
- Category B FlyerDocument8 pagesCategory B FlyerHarishNo ratings yet
- Social Work Practice in Healthcare Advanced Approaches and Emerging Trends 1st Edition Allen Test Bank 1Document9 pagesSocial Work Practice in Healthcare Advanced Approaches and Emerging Trends 1st Edition Allen Test Bank 1matthew100% (49)
- NBHS2513 Professional Issues in HealthcareDocument13 pagesNBHS2513 Professional Issues in HealthcareSimon RajNo ratings yet
- The Evaluation of Payment For Obstetric and Gynecology Services - From ACOGDocument14 pagesThe Evaluation of Payment For Obstetric and Gynecology Services - From ACOGWillans Eduardo Rosha HumerezNo ratings yet
- Volunteer in Nursing Home FinalDocument3 pagesVolunteer in Nursing Home FinalJulie KnightNo ratings yet
- Maternal and Child HealthDocument60 pagesMaternal and Child HealthStar AcademyNo ratings yet
- Issu Perkembangan RMDocument13 pagesIssu Perkembangan RMAulia FitriNo ratings yet
- Annotated BibliographyDocument2 pagesAnnotated Bibliographyrajwadi suzyNo ratings yet
- B T M S Gims F: Esearch ProposalDocument5 pagesB T M S Gims F: Esearch ProposalFabiola NogaNo ratings yet
- UntitledDocument69 pagesUntitledShipra BansalNo ratings yet
- QwewqeDocument1 pageQwewqeMuneeb ShahzadNo ratings yet
- Test Bank Advanced Practice Nursing Essential Knowledge For The Profession 4th Edition DeNiscoDocument3 pagesTest Bank Advanced Practice Nursing Essential Knowledge For The Profession 4th Edition DeNiscoFit ragner0% (1)
- Nursing Health Education and Improving Patient Self-Management Intervention Mapping For Healthy Lifestyles, 2nd Edition (Barbara Sassen) (Z-Library)Document358 pagesNursing Health Education and Improving Patient Self-Management Intervention Mapping For Healthy Lifestyles, 2nd Edition (Barbara Sassen) (Z-Library)trishaashleycalvoNo ratings yet
- NHS FPX 5004 Assessment 3 Diversity Project Kickoff PresentationDocument5 pagesNHS FPX 5004 Assessment 3 Diversity Project Kickoff Presentationjoohnsmith070No ratings yet
- WalmartDocument2 pagesWalmartDr Kausalya DeviprasadNo ratings yet
- Understanding Pharmacology For Pharmacy Technician 230904 234215Document862 pagesUnderstanding Pharmacology For Pharmacy Technician 230904 234215Sohail AdnanNo ratings yet
- BT 2023141Document2 pagesBT 2023141Indiana Family to FamilyNo ratings yet
- Biography of Madeleine LeiningerDocument3 pagesBiography of Madeleine LeiningerNajihah :sNo ratings yet
- UC-VPAA-CON-FORM-10a August 2018 REV. 01Document2 pagesUC-VPAA-CON-FORM-10a August 2018 REV. 01Medeah Faye AbesNo ratings yet
- HealthCare System of NigeriaDocument8 pagesHealthCare System of Nigeriavictor jjumaNo ratings yet
- rptHosOPGL 2Document1 pagerptHosOPGL 2Subba Rao SemenchalamNo ratings yet
- School-Based Telemedicine For AsthmaDocument9 pagesSchool-Based Telemedicine For AsthmaJesslynBernadetteNo ratings yet
- 2023 ADL NATHEALTH Digital ReportDocument35 pages2023 ADL NATHEALTH Digital ReportMoumita Roy ChowdhuryNo ratings yet
- Discharge Sample LetterDocument3 pagesDischarge Sample LetterMarcelaNo ratings yet
- Healthcare Quality and Hospital Financial Performance: A Multilevel FrameworkDocument11 pagesHealthcare Quality and Hospital Financial Performance: A Multilevel Frameworkadrian_badriNo ratings yet
- Patient Safety Standards Surveyor Guide For HospitalsDocument58 pagesPatient Safety Standards Surveyor Guide For HospitalsNgụy Lê Thùy DươngNo ratings yet
- Impact of Human Factors On Interprofessional Collaboration and Service User Safety.Document12 pagesImpact of Human Factors On Interprofessional Collaboration and Service User Safety.Brymak BryantNo ratings yet
- The Future of Us Healthcare Whats Next For The Industry Post Covid 19Document13 pagesThe Future of Us Healthcare Whats Next For The Industry Post Covid 19miltechinsightsNo ratings yet
- Nurs 233 Summative Clinical Evaluation-AfDocument3 pagesNurs 233 Summative Clinical Evaluation-Afapi-596284176No ratings yet