You might also like
- Proprioceptive Neuromuscular Facilitation (PNF)Document76 pagesProprioceptive Neuromuscular Facilitation (PNF)Hasan KhawaldehNo ratings yet
- Proprioceptive Neuromuscular Facilitation (PNF)Document76 pagesProprioceptive Neuromuscular Facilitation (PNF)Hasan KhawaldehNo ratings yet
- Course - Fundamentals of Traditional Chinese Medicine - Center For True HealingDocument49 pagesCourse - Fundamentals of Traditional Chinese Medicine - Center For True HealingAry Nogueira100% (1)
- Rivers - Jane Ayurveda For Beginners - Understand and Apply Essential Ayurvedic Principles and PracticDocument146 pagesRivers - Jane Ayurveda For Beginners - Understand and Apply Essential Ayurvedic Principles and PracticbazediNo ratings yet
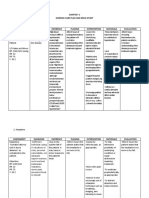
- NCP For Dizziness and HeadacheDocument4 pagesNCP For Dizziness and Headachekarthi karthi100% (1)
- Basic Concepts in Occupational MedicineDocument52 pagesBasic Concepts in Occupational MedicineEldorhezaNo ratings yet
- Typhoid FeverDocument20 pagesTyphoid FeverKylie GolindangNo ratings yet
- Cognitive-Behavioral Therapy For Body Dysmorphic DisorderDocument9 pagesCognitive-Behavioral Therapy For Body Dysmorphic DisorderArmando ValladaresNo ratings yet
- 1st Grading Exam MAPEHDocument4 pages1st Grading Exam MAPEHSherlita Vargas Mainit DurogNo ratings yet
- Susan Edwards - Neurological PhysiotherapyDocument293 pagesSusan Edwards - Neurological Physiotherapyharcaian_cristina90% (20)
- NCLEX-RN Test Plan (Detailed Candiate Version)Document62 pagesNCLEX-RN Test Plan (Detailed Candiate Version)Filipino Nurses CentralNo ratings yet
- Assessment and Interventions For Perinatal DepressionDocument168 pagesAssessment and Interventions For Perinatal Depressiondavid100% (1)
- Medical Ethics and Law (Questions and Answers) Prof. Ahmed Ammar PDFDocument15 pagesMedical Ethics and Law (Questions and Answers) Prof. Ahmed Ammar PDFRabia Khaira100% (1)
- Assessment Management of PainDocument104 pagesAssessment Management of PainCharles B. LópezNo ratings yet
- Implementation Strategies For Health Systems in Low-AcountriesDocument135 pagesImplementation Strategies For Health Systems in Low-AcountriesAlbert Lawrence Kwansa0% (1)
- Emergency Care Emt 13th Edition Ebook PDFDocument61 pagesEmergency Care Emt 13th Edition Ebook PDFadolfo.milliken17896% (48)
- Referat Sudden Death - ForensikDocument44 pagesReferat Sudden Death - ForensikMuhamad PascadhNo ratings yet
- Perinatal Depression FINAL Web 0 (001-078) PDFDocument78 pagesPerinatal Depression FINAL Web 0 (001-078) PDFMARIA PAULA FLOREZ GIRALDONo ratings yet
- Week 6-MCQ in EBP-1Document36 pagesWeek 6-MCQ in EBP-1Hasan KhawaldehNo ratings yet
- Psychiatry EmergencyDocument121 pagesPsychiatry EmergencyDr. Jayesh Patidar67% (6)
- MNCHNDocument45 pagesMNCHNAnn Margareth Salazar-ManaloNo ratings yet
- THCU - SituationalAssesmentToolsDocument273 pagesTHCU - SituationalAssesmentToolsdhernández_gualdrónNo ratings yet
- The Medical Research Handbook - Clinical Research Centre PDFDocument96 pagesThe Medical Research Handbook - Clinical Research Centre PDFDaveMartoneNo ratings yet
- Dialog Percakapan Bidan Tugas Bahs Inggris DedeDocument5 pagesDialog Percakapan Bidan Tugas Bahs Inggris DedeSardianto TurnipNo ratings yet
- Mcginley 2009Document10 pagesMcginley 2009Fernanda AhumadaNo ratings yet
- Khoury 2013 Mindfulness-MetaanalysDocument9 pagesKhoury 2013 Mindfulness-Metaanalysrohit singhNo ratings yet
- Bal MI Et Al 2016Document17 pagesBal MI Et Al 2016jackNo ratings yet
- A Critical Review of Cosmetic Treatment Outcomes in Body Dysmorphic DisorderDocument8 pagesA Critical Review of Cosmetic Treatment Outcomes in Body Dysmorphic DisorderJuliano MarquesNo ratings yet
- Delre 2012Document8 pagesDelre 2012Sergio AlonsoNo ratings yet
- 2016 - Abdulmalik - Community Mental Health A Brief, Global PerspectiveDocument4 pages2016 - Abdulmalik - Community Mental Health A Brief, Global PerspectiveRAFAELA PAOLA VASQUEZ VILCHEZNo ratings yet
- GERDDocument17 pagesGERDIntan AnanthaNo ratings yet
- Fletcher 2016Document10 pagesFletcher 2016Christina Putri BongzueNo ratings yet
- 1 s2.0 S0956053X17303069 MainDocument30 pages1 s2.0 S0956053X17303069 MainAlain DelonNo ratings yet
- Barbato Et Al-2018-Cochrane Database of Systematic ReviewsDocument79 pagesBarbato Et Al-2018-Cochrane Database of Systematic ReviewsfiskaderishaNo ratings yet
- 1 s2.0 S1013905221000481 Main 2Document10 pages1 s2.0 S1013905221000481 Main 2Palena PintoNo ratings yet
- Consciousness and Cognition: Denholm J. Aspy, Paul Delfabbro, Michael ProeveDocument11 pagesConsciousness and Cognition: Denholm J. Aspy, Paul Delfabbro, Michael ProeveKatja GoiteNo ratings yet
- Exposición Ocupacional A Campos Magnéticos de Frecuencia Extremadamente Baja y Riesgo de Enfermedad de AlzheimerDocument11 pagesExposición Ocupacional A Campos Magnéticos de Frecuencia Extremadamente Baja y Riesgo de Enfermedad de AlzheimerLucilaNo ratings yet
- A Review of The Literature On Citation Impact IndicatorsDocument27 pagesA Review of The Literature On Citation Impact IndicatorsroaaNo ratings yet
- Patient Perceptions of Clinical Care in Complementary MedicineDocument12 pagesPatient Perceptions of Clinical Care in Complementary MedicinevtcNo ratings yet
- 1 s2.0 S2352550922003116 MainDocument16 pages1 s2.0 S2352550922003116 MainCristina SalasNo ratings yet
- Criteria and Practices For Lean and Green Performance AssessmentDocument17 pagesCriteria and Practices For Lean and Green Performance AssessmentNuriaNo ratings yet
- The Effects of Fluoride in Thedrinking WaterDocument83 pagesThe Effects of Fluoride in Thedrinking Waterfreitas420danielNo ratings yet
- Clinical Trials and Regulatory Science in CardiologyDocument8 pagesClinical Trials and Regulatory Science in Cardiologyfister19 rifaudinNo ratings yet
- Beneficios de Los Micronutrientes en La GestacionDocument94 pagesBeneficios de Los Micronutrientes en La GestacionAdrián Pérez VázquezNo ratings yet
- Ed 594157Document100 pagesEd 594157KALAVALA MAHESH BABUNo ratings yet
- NICE Evidence Review 2022 SLTDocument150 pagesNICE Evidence Review 2022 SLTSusan BernalesNo ratings yet
- Systematic Review of Salutogenic-Oriented Lifestyle Randomised Controlled Trials For Adults With Type 2 Diabetes MellitusDocument13 pagesSystematic Review of Salutogenic-Oriented Lifestyle Randomised Controlled Trials For Adults With Type 2 Diabetes MellitusluizaromerouspNo ratings yet
- 1 s2.0 S0738399120300677 MainDocument9 pages1 s2.0 S0738399120300677 MainemmaNo ratings yet
- Health Literacy and AdherenceDocument8 pagesHealth Literacy and Adherencehairun hairunNo ratings yet
- Vaccine SCDocument19 pagesVaccine SCNaman AgarwalNo ratings yet
- Gardening Is Beneficial For Health: A Meta-AnalysisDocument8 pagesGardening Is Beneficial For Health: A Meta-AnalysisHaritha DeviNo ratings yet
- Clinical Psychology ReviewDocument11 pagesClinical Psychology ReviewAlex SolorzanoNo ratings yet
- Childrens Social-Emotional Wellbeing Paper PDFDocument46 pagesChildrens Social-Emotional Wellbeing Paper PDFAndreia SilvaNo ratings yet
- National Standards Project,: Findings ConclusionsDocument92 pagesNational Standards Project,: Findings Conclusionsluiztaz07No ratings yet
- What Is Stopping The Automotive Industry From Going Green? A Systematic Review of Barriers To Green Innovation in The Automotive IndustryDocument11 pagesWhat Is Stopping The Automotive Industry From Going Green? A Systematic Review of Barriers To Green Innovation in The Automotive IndustryCHRISTY UKONo ratings yet
- ArticuloDocument5 pagesArticuloJuliana Nathaly SanabriaNo ratings yet
- Social Cognitive Interventions For People With SchizophreniaDocument17 pagesSocial Cognitive Interventions For People With SchizophreniaCheesyPorkBellyNo ratings yet
- Psychiatry Research: Bing Cao, Dong-Fang Wang, Mei-Yan Xu, Ya-Qiong Liu, Lai-Lai Yan, Jing-Yu Wang, Qing-Bin LuDocument7 pagesPsychiatry Research: Bing Cao, Dong-Fang Wang, Mei-Yan Xu, Ya-Qiong Liu, Lai-Lai Yan, Jing-Yu Wang, Qing-Bin LuRuy AntonucciNo ratings yet
- Flodgren 2016Document86 pagesFlodgren 2016Joaquín Guillermo González ArocaNo ratings yet
- Teamwork in Healthcare: Promoting Effective Teamwork in Healthcare in CanadaDocument47 pagesTeamwork in Healthcare: Promoting Effective Teamwork in Healthcare in CanadawendyNo ratings yet
- The Role of Neural Artificial Intelligence For Diagnosis and Treatment Planning in Endodontics A Qualitative ReviewDocument12 pagesThe Role of Neural Artificial Intelligence For Diagnosis and Treatment Planning in Endodontics A Qualitative ReviewkarenyaxencorrearivasNo ratings yet
- Diabetes Empowerment Dan Psikososial ParameterDocument14 pagesDiabetes Empowerment Dan Psikososial ParameterMuhammad MulyadiNo ratings yet
- Meta Analise Das InfiltraçõesDocument10 pagesMeta Analise Das InfiltraçõesAnderson Soares SouzaNo ratings yet
- A Ann Ischemic StrokeDocument38 pagesA Ann Ischemic StrokeSons YesuNo ratings yet
- 2009 Ostomy - Care - ManagementDocument117 pages2009 Ostomy - Care - Managementdurdane palabiyik yilmazNo ratings yet
- 10 1016@j Dental 2020 03 020Document37 pages10 1016@j Dental 2020 03 020angi trujilloNo ratings yet
- FASJ - 2017 - Valisena - TX of Mortons Neuroma - Systematic ReviewDocument11 pagesFASJ - 2017 - Valisena - TX of Mortons Neuroma - Systematic ReviewJacob DoughertyNo ratings yet
- Pulse Oximetry Screening For Critical Congenital Heart DefectsDocument83 pagesPulse Oximetry Screening For Critical Congenital Heart DefectsFajar YuniftiadiNo ratings yet
- ADA Clinical Practice Guidelines Handbook - 2013 UpdateDocument59 pagesADA Clinical Practice Guidelines Handbook - 2013 Updateمازن كريم حمودNo ratings yet
- Lower Folate Levels in SchizophreniaDocument8 pagesLower Folate Levels in SchizophreniaIqbal AbdillahNo ratings yet
- International Journal of Pediatric OtorhinolaryngologyDocument10 pagesInternational Journal of Pediatric OtorhinolaryngologySiti Hidayatul FitriNo ratings yet
- Handoll Et Al-2003-The Cochrane Distales de RadioDocument77 pagesHandoll Et Al-2003-The Cochrane Distales de RadioSusan LyNo ratings yet
- Atherosclerosis: Review QDocument9 pagesAtherosclerosis: Review QAsri RachmawatiNo ratings yet
- Behavioral and Social Science Foundations For Future Physicianssecond PDFDocument45 pagesBehavioral and Social Science Foundations For Future Physicianssecond PDFPravin PatelNo ratings yet
- The Agile Approach to Adaptive Research: Optimizing Efficiency in Clinical DevelopmentFrom EverandThe Agile Approach to Adaptive Research: Optimizing Efficiency in Clinical DevelopmentNo ratings yet
- The Matrix System at Work: An Evaluation of the World Bank's Organizational EffectivenessFrom EverandThe Matrix System at Work: An Evaluation of the World Bank's Organizational EffectivenessNo ratings yet
- Stroke, Cognitive de Cits, and Rehabilitation Still An Incomplete Picture JournalDocument8 pagesStroke, Cognitive de Cits, and Rehabilitation Still An Incomplete Picture JournalPutri YunandaNo ratings yet
- A Treatment-Based Classification Approach To Low Back PainDocument80 pagesA Treatment-Based Classification Approach To Low Back PainHasan KhawaldehNo ratings yet
- Stroke, Cognitive de Cits, and Rehabilitation Still An Incomplete Picture JournalDocument8 pagesStroke, Cognitive de Cits, and Rehabilitation Still An Incomplete Picture JournalPutri YunandaNo ratings yet
- The Natural History of Depression Up To 15 Years After StrokeDocument6 pagesThe Natural History of Depression Up To 15 Years After StrokeHasan KhawaldehNo ratings yet
- Lab 5 Closed Kinetic Chain Requires That The Distal Segment Is Fixed (Closed)Document1 pageLab 5 Closed Kinetic Chain Requires That The Distal Segment Is Fixed (Closed)Hasan KhawaldehNo ratings yet
- Case StudyDocument2 pagesCase StudyHasan KhawaldehNo ratings yet
- Kinsiology Lab 3Document3 pagesKinsiology Lab 3Hasan KhawaldehNo ratings yet
- Kinesiology LAB (3) : Joint Surface PositionsDocument3 pagesKinesiology LAB (3) : Joint Surface PositionsHasan KhawaldehNo ratings yet
- Lab 1 Physical AgentsDocument15 pagesLab 1 Physical AgentsHasan KhawaldehNo ratings yet
- Home Work 3Document1 pageHome Work 3Hasan KhawaldehNo ratings yet
- Everyday English 1 PrintableDocument171 pagesEveryday English 1 PrintableHasan KhawaldehNo ratings yet
- Ankle Planter Flexion: Test: Patient Raises Heel From Floor Consecutively Through Full Range of Plantar FlexionDocument30 pagesAnkle Planter Flexion: Test: Patient Raises Heel From Floor Consecutively Through Full Range of Plantar FlexionHasan KhawaldehNo ratings yet
- Everyday English 1 PrintableDocument171 pagesEveryday English 1 PrintableHasan KhawaldehNo ratings yet
- Odds Ratio DiagramsDocument1 pageOdds Ratio DiagramsHasan KhawaldehNo ratings yet
- Neurological Examination Made Practical PDFDocument206 pagesNeurological Examination Made Practical PDFNorman VallejoNo ratings yet
- Test BankDocument17 pagesTest BankHasan KhawaldehNo ratings yet
- Premarket Notification 510 (K) Guidance For Contact Lens Care Products (PDF Only)Document172 pagesPremarket Notification 510 (K) Guidance For Contact Lens Care Products (PDF Only)Ganesh NatarajanNo ratings yet
- CIRCI Guidelines 2015Document6 pagesCIRCI Guidelines 2015Wissam SleimanNo ratings yet
- Cabaleiro - Developing A Method To Assessing The MunicipalDocument23 pagesCabaleiro - Developing A Method To Assessing The MunicipalNave InodNo ratings yet
- Wound InfectionDocument6 pagesWound InfectionCatarina DiasNo ratings yet
- Universal Precautions (UP)Document26 pagesUniversal Precautions (UP)Avigael Gabriel AvilesNo ratings yet
- NCM 109 Maternal Lecture Lesson: CausesDocument2 pagesNCM 109 Maternal Lecture Lesson: CausesJanelle ArcillaNo ratings yet
- Leave RuleDocument28 pagesLeave RuleMd. Sahir KhanNo ratings yet
- Fourth Grading NotesDocument70 pagesFourth Grading NotesMini RinnNo ratings yet
- Comfort, Effectiveness, AND Self-Awareness AS Criteria OF Improvement IN Psychotherapy"2Document10 pagesComfort, Effectiveness, AND Self-Awareness AS Criteria OF Improvement IN Psychotherapy"2Ilaria PacificoNo ratings yet
- Physical Layout PICUDocument8 pagesPhysical Layout PICUMeena Koushal0% (1)
- ADHD in ChildrenDocument10 pagesADHD in ChildrenDebbie KlippNo ratings yet
- DoctorsHanbook ch14 PDFDocument10 pagesDoctorsHanbook ch14 PDFEdsel JavellanaNo ratings yet
- Pre and Post Operative Care: To: DR - Biniyam.G By: Biniam.MDocument55 pagesPre and Post Operative Care: To: DR - Biniyam.G By: Biniam.MBini JaminNo ratings yet
- Family PlanningDocument15 pagesFamily PlanningOkky isNo ratings yet
- Psychologist Cover Letter ExampleDocument4 pagesPsychologist Cover Letter Exampleafjzcgeoylbkku100% (2)
- BookDocument193 pagesBookFran SeptaNo ratings yet
- Mei Penyakit UmumDocument1 pageMei Penyakit Umumghaniangga11No ratings yet
- 8 Effect of Exercises in The Management of PDFDocument254 pages8 Effect of Exercises in The Management of PDFAmalia RiaNo ratings yet
- Medical Terminology Chapter 3 Verified AnswersDocument8 pagesMedical Terminology Chapter 3 Verified AnswersGregg ProducerNo ratings yet