You might also like
- Oral Sustained Release Drug Delivery Systems OverviewDocument0 pagesOral Sustained Release Drug Delivery Systems Overviewg20kpNo ratings yet
- Extended Release Drug Delivery ReviewDocument9 pagesExtended Release Drug Delivery ReviewTuyến Đặng ThịNo ratings yet
- Controlled Release Pellets: An Effective Tool in Chronic TherapyDocument26 pagesControlled Release Pellets: An Effective Tool in Chronic TherapyfakhriNo ratings yet
- Sustained Release Matrix Type Drug Delivery System: An OverviewDocument12 pagesSustained Release Matrix Type Drug Delivery System: An OverviewRohit SinghNo ratings yet
- Article Wjpps 14988056511Document12 pagesArticle Wjpps 14988056511Its MENo ratings yet
- Formulation and Evaluation of Glipizide Sustained Release Matrix TabletDocument46 pagesFormulation and Evaluation of Glipizide Sustained Release Matrix TabletInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Publish Review ArticleDocument25 pagesPublish Review ArticleHana HerdianiNo ratings yet
- 1.1 Oral Drug Delivery: Scope and AdvantagesDocument7 pages1.1 Oral Drug Delivery: Scope and AdvantagesPriyanka NairNo ratings yet
- Introduction To Novel Drug Delivery SystDocument5 pagesIntroduction To Novel Drug Delivery SystshreeharilxrNo ratings yet
- Controlled Drug Delivery Systems - 1 PDFDocument6 pagesControlled Drug Delivery Systems - 1 PDFVikash Kushwaha100% (1)
- Diploma EEE DocumentDocument72 pagesDiploma EEE DocumentJaganMohanGuduruNo ratings yet
- NDDS 2017Document12 pagesNDDS 2017otiNo ratings yet
- Controlled Drug DeliveryDocument23 pagesControlled Drug DeliveryAnburaj JamesNo ratings yet
- Transdermal Drug Delivery System (TDDS) - A Multifaceted Approach For Drug DeliveryDocument32 pagesTransdermal Drug Delivery System (TDDS) - A Multifaceted Approach For Drug DeliveryKamranNo ratings yet
- Jurnal Tugas FarmakologiDocument13 pagesJurnal Tugas FarmakologiCiendy ShintyaNo ratings yet
- 17.alekhya Research ArticleDocument8 pages17.alekhya Research ArticleBaru Chandrasekhar RaoNo ratings yet
- Sustained Release Drug Delivery System - A ReviewDocument14 pagesSustained Release Drug Delivery System - A ReviewPranav PatelNo ratings yet
- Bp704t Ndds IDocument25 pagesBp704t Ndds Iapplied chemistNo ratings yet
- 2015 Transdermal Patches A Review On Novel Approach For Drug Delivery PDFDocument18 pages2015 Transdermal Patches A Review On Novel Approach For Drug Delivery PDFDolih Gozali100% (1)
- Ijps258 269Document12 pagesIjps258 269Kristine Dwi PuspitasariNo ratings yet
- Controlled Release Drug Formulation in Pharmaceuticals: A Study On Their Application and PropertiesDocument17 pagesControlled Release Drug Formulation in Pharmaceuticals: A Study On Their Application and PropertiesintanNo ratings yet
- Multi-Layer TabletsDocument14 pagesMulti-Layer Tabletsprasad_ram8850% (2)
- A Review On Controlled Drug Delivery SystemDocument8 pagesA Review On Controlled Drug Delivery SystemDogbey AlbertNo ratings yet
- Advantages Disadvantages: Parts of Hospital FormularyDocument4 pagesAdvantages Disadvantages: Parts of Hospital Formularyjohanna tamargoNo ratings yet
- Pharmaceutics Chapter 7 Novel Drug Delivery System NotesDocument10 pagesPharmaceutics Chapter 7 Novel Drug Delivery System NotesBhuvnesh ChandraNo ratings yet
- Matrix TabletsDocument14 pagesMatrix TabletsJohnNo ratings yet
- Sustained ReleaseDocument9 pagesSustained ReleaseFenny rahmadhanyNo ratings yet
- Gupta Kumar - Nano Meningkatkan BA DLLDocument40 pagesGupta Kumar - Nano Meningkatkan BA DLLHesti HariantiNo ratings yet
- Topical Drug DeliveryDocument21 pagesTopical Drug DeliveryhappyNo ratings yet
- SPO - Controlled ReleaseDocument13 pagesSPO - Controlled Releasewahyu ilahiNo ratings yet
- 6Document11 pages6UgaugaaNo ratings yet
- SRDDS Matrix TabletDocument17 pagesSRDDS Matrix TabletMISBAH KAUSARNo ratings yet
- Drug Delivery and Hydrotropism Dr. Sunil KulkarniDocument5 pagesDrug Delivery and Hydrotropism Dr. Sunil KulkarniKRISHNA SINGHNo ratings yet
- Bcs Drug ReleaseDocument45 pagesBcs Drug ReleaseVekariya RutvikNo ratings yet
- 954-Article Text-2466-1-10-20210617Document6 pages954-Article Text-2466-1-10-20210617Chandresh PatelNo ratings yet
- Extended Release Formulation Review ArticleDocument60 pagesExtended Release Formulation Review ArticleSomasundaram JeevanandhamNo ratings yet
- Good Pharmaceutical Practices OnDocument6 pagesGood Pharmaceutical Practices OnTabassum TumpaNo ratings yet
- Goal Drug Prodrugs and Lead CompoundsDocument6 pagesGoal Drug Prodrugs and Lead CompoundsJovanne D. BrownNo ratings yet
- Modified Release Drug Delivery SystemDocument11 pagesModified Release Drug Delivery SystemArvi KhanNo ratings yet
- NDDS AnswersDocument56 pagesNDDS AnswersPrajwal PatankarNo ratings yet
- RMHP 16 2531Document11 pagesRMHP 16 2531Daniele NichesolaNo ratings yet
- Controlled Injectable Drug Delivery OverviewDocument11 pagesControlled Injectable Drug Delivery OverviewWandikbogweNo ratings yet
- 1 - Pendahuluan - Drug Delivery Systems-09 2016Document26 pages1 - Pendahuluan - Drug Delivery Systems-09 2016Kos KosasihNo ratings yet
- Drug Delivery Systems - An Update ReviewDocument10 pagesDrug Delivery Systems - An Update ReviewenzomontresolNo ratings yet
- Sustained Release Drug Delivery System Potential: The Pharma InnovationDocument13 pagesSustained Release Drug Delivery System Potential: The Pharma InnovationprinceamitNo ratings yet
- Controlled Release DesignDocument88 pagesControlled Release DesignSoma Ranjith100% (1)
- Modified Release Formulations To Achieve The QualiDocument11 pagesModified Release Formulations To Achieve The QualiShannya PuaNo ratings yet
- Pharmacopolitics, Implications and Implementation in Clinical StudiesDocument3 pagesPharmacopolitics, Implications and Implementation in Clinical StudiesNantarat KengkeatchaiNo ratings yet
- GumGhattiDocument14 pagesGumGhattisadafNo ratings yet
- Concept and Design of Rate Controlled Drug DeliveryDocument57 pagesConcept and Design of Rate Controlled Drug Deliveryufahad88% (8)
- A Prolonged Release Parenteral Drug Delivery SystemDocument11 pagesA Prolonged Release Parenteral Drug Delivery SystemronnymcmNo ratings yet
- Biopharmaceutics - BrahmankarDocument414 pagesBiopharmaceutics - Brahmankarmatin586% (57)
- Formulation Development and Evaluation of Sustained Release Tablet Chlorpromazine HCLDocument7 pagesFormulation Development and Evaluation of Sustained Release Tablet Chlorpromazine HCLWJPSR JournalNo ratings yet
- Pharm MGT NotesDocument62 pagesPharm MGT NotesMOHAMMED B KAMARANo ratings yet
- Renal Pharmacotherapy: Dosage Adjustment of Medications Eliminated by the KidneysFrom EverandRenal Pharmacotherapy: Dosage Adjustment of Medications Eliminated by the KidneysNo ratings yet
- Microneedle-mediated Transdermal and Intradermal Drug DeliveryFrom EverandMicroneedle-mediated Transdermal and Intradermal Drug DeliveryNo ratings yet
- Clinical Challenges in Therapeutic Drug Monitoring: Special Populations, Physiological Conditions and PharmacogenomicsFrom EverandClinical Challenges in Therapeutic Drug Monitoring: Special Populations, Physiological Conditions and PharmacogenomicsNo ratings yet
- Essential Pharmacokinetics: A Primer for Pharmaceutical ScientistsFrom EverandEssential Pharmacokinetics: A Primer for Pharmaceutical ScientistsRating: 5 out of 5 stars5/5 (1)
- Prodrug Design: Perspectives, Approaches and Applications in Medicinal ChemistryFrom EverandProdrug Design: Perspectives, Approaches and Applications in Medicinal ChemistryRating: 3 out of 5 stars3/5 (1)
- CH 6701 Cre IiDocument230 pagesCH 6701 Cre IiVaibhav Gupta100% (1)
- ChitosanDocument63 pagesChitosanTamiko MizumaNo ratings yet
- FTIR Spectroscopy Characterization of Poly (Vinyl Alcohol) Hydrogel With Different Hydrolysis Degree and Chemically Crosslinked With GlutaraldehydeDocument10 pagesFTIR Spectroscopy Characterization of Poly (Vinyl Alcohol) Hydrogel With Different Hydrolysis Degree and Chemically Crosslinked With GlutaraldehydeAnderson Fernandez OsorioNo ratings yet
- Magic GelDocument2 pagesMagic GelsonytechoNo ratings yet
- Bigels and Multicomponent Organogels - An Overview From Rheological Perspective - 2021Document25 pagesBigels and Multicomponent Organogels - An Overview From Rheological Perspective - 2021Elena AnghelNo ratings yet
- High Energy Radiation and Polymers, A Review of Commercial Processes and Emerging ApplicationsDocument26 pagesHigh Energy Radiation and Polymers, A Review of Commercial Processes and Emerging ApplicationsMile007No ratings yet
- GIEBEL - Manual Oven Regeneration Silica Gel - ENDocument4 pagesGIEBEL - Manual Oven Regeneration Silica Gel - ENFernando MurrietaNo ratings yet
- Purolite MB400 LDocument1 pagePurolite MB400 LjoaoNo ratings yet
- ELASTIGEL 1000J Technical SpecificationDocument1 pageELASTIGEL 1000J Technical SpecificationMaurice Dan GeroyNo ratings yet
- Ma 051698Document5 pagesMa 051698eduardo dias goisNo ratings yet
- A Strategy For Attacking Excess Water ProductionDocument16 pagesA Strategy For Attacking Excess Water ProductionJose Leonardo Materano PerozoNo ratings yet
- NPTEL Chemical Engineering Solid Catalyst ComponentsDocument254 pagesNPTEL Chemical Engineering Solid Catalyst ComponentsvigeshNo ratings yet
- Rheology of Hyaluronic Acid and Dynamic Facial Rejuvenation: Topographical SpecificitiesDocument8 pagesRheology of Hyaluronic Acid and Dynamic Facial Rejuvenation: Topographical SpecificitiesDanna RomeroNo ratings yet
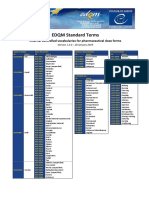
- Standard Terms Internal Vocabularies For Pharmaceutical Dose FormsDocument7 pagesStandard Terms Internal Vocabularies For Pharmaceutical Dose FormsJose De La Cruz De La ONo ratings yet
- Personal Care & Cosmetic Grade HECDocument3 pagesPersonal Care & Cosmetic Grade HECrafaeldelperu1982No ratings yet
- Modification of Food Characteristics With CMCDocument10 pagesModification of Food Characteristics With CMCJR NilNo ratings yet
- HP Drilling Fluid CatalogDocument33 pagesHP Drilling Fluid CatalogmobtelecomNo ratings yet
- Classification and Types of GelsDocument7 pagesClassification and Types of GelskarenNo ratings yet
- Alcoflood 254S - Types PDFDocument16 pagesAlcoflood 254S - Types PDFAnonymous T32l1RNo ratings yet
- Super Water Absorbing Polymeric Gel From Chitosan, Citric Acid and Urea Synthesis and Mechanism of Water AbsorptionDocument9 pagesSuper Water Absorbing Polymeric Gel From Chitosan, Citric Acid and Urea Synthesis and Mechanism of Water AbsorptionRosa VasquezNo ratings yet
- Bottom-Up and Top-Down Nanoparticle Synthesis MethodsDocument35 pagesBottom-Up and Top-Down Nanoparticle Synthesis MethodsRaghendra DubeyNo ratings yet
- Formulation and Evaluation of Zolpidem Nasal in SituDocument12 pagesFormulation and Evaluation of Zolpidem Nasal in SituGopalasatheeskumar KNo ratings yet
- Formulas para SpaDocument41 pagesFormulas para Spaeduardo100% (1)
- Protein Structure-Function Relationships in FoodsDocument213 pagesProtein Structure-Function Relationships in FoodsAmuthachelvi DanielNo ratings yet
- APS - TEMED ReactionDocument11 pagesAPS - TEMED ReactionMichiko MatsuoNo ratings yet
- 12088600Document9 pages12088600deni.sttnNo ratings yet
- AEROSIL® 200: Hydrophilic Fumed SilicaDocument2 pagesAEROSIL® 200: Hydrophilic Fumed SilicaAPEX SONNo ratings yet
- Silica particles deliver drugsDocument8 pagesSilica particles deliver drugsNitesh JajuNo ratings yet
- Colloidal Systems PPT 1416cDocument14 pagesColloidal Systems PPT 1416cpaupalau2010No ratings yet
- The Effect of ShearDocument11 pagesThe Effect of Shearanakren296No ratings yet