Professional Documents
Culture Documents
Dehghan Latestproof
Uploaded by
Sam SallyOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Dehghan Latestproof
Uploaded by
Sam SallyCopyright:
Available Formats
See discussions, stats, and author profiles for this publication at: https://www.researchgate.
net/publication/319363211
Associations of fats and carbohydrate intake with cardiovascular disease and
mortality in 18 countries from five continents (PURE): A prospective cohort
study
Article in The Lancet · August 2017
DOI: 10.1016/S0140-6736(17)32252-3
CITATIONS READS
897 11,324
356 authors, including:
Mahshid Dehghan Andrew Mente
McMaster University McMaster University
90 PUBLICATIONS 8,812 CITATIONS 130 PUBLICATIONS 13,306 CITATIONS
SEE PROFILE SEE PROFILE
Xiaohe Zhang Sumathi Swaminathan
Tongji University St. John's Research Institute
23 PUBLICATIONS 4,299 CITATIONS 85 PUBLICATIONS 6,465 CITATIONS
SEE PROFILE SEE PROFILE
All content following this page was uploaded by Mariz Sintaha on 06 November 2019.
The user has requested enhancement of the downloaded file.
Articles
Associations of fats and carbohydrate intake with
cardiovascular disease and mortality in 18 countries from
five continents (PURE): a prospective cohort study
Mahshid Dehghan, Andrew Mente, Xiaohe Zhang, Sumathi Swaminathan, Wei Li, Viswanathan Mohan, Romaina Iqbal, Rajesh Kumar,
Edelweiss Wentzel-Viljoen, Annika Rosengren, Leela Itty Amma, Alvaro Avezum, Jephat Chifamba, Rafael Diaz, Rasha Khatib, Scott Lear,
Patricio Lopez-Jaramillo, Xiaoyun Liu, Rajeev Gupta, Noushin Mohammadifard, Nan Gao, Aytekin Oguz, Anis Safura Ramli, Pamela Seron,
Yi Sun, Andrzej Szuba, Lungiswa Tsolekile, Andreas Wielgosz, Rita Yusuf, Afzal Hussein Yusufali, Koon K Teo, Sumathy Rangarajan, Gilles
Dagenais, Shrikant I Bangdiwala, Shofiqul Islam, Sonia S Anand, Salim Yusuf, on behalf of the Prospective Urban Rural Epidemiology (PURE)
study investigators*
Summary
Background The relationship between macronutrients and cardiovascular disease and mortality is controversial. Most Published Online
available data are from European and North American populations where nutrition excess is more likely, so their August 29, 2017
http://dx.doi.org/10.1016/
applicability to other populations is unclear. S0140-6736(17)32252-3
See Online/Comment
Methods The Prospective Urban Rural Epidemiology (PURE) study is a large, epidemiological cohort study of http://dx.doi.org/10.1016/
individuals aged 35–70 years (enrolled between Jan 1, 2003, and March 31, 2013) in 18 countries with a median follow- S0140-6736(17)32241-9
up of 7·4 years (IQR 5·3–9·3). Dietary intake of 135 335 individuals was recorded using validated food frequency *Investigators listed in the
questionnaires. The primary outcomes were total mortality and major cardiovascular events (fatal cardiovascular appendix
disease, non-fatal myocardial infarction, stroke, and heart failure). Secondary outcomes were all myocardial Population Health Research
infarctions, stroke, cardiovascular disease mortality, and non-cardiovascular disease mortality. Participants were Institute, McMaster University,
Hamilton, ON, Canada
categorised into quintiles of nutrient intake (carbohydrate, fats, and protein) based on percentage of energy provided (M Dehghan PhD, A Mente PhD,
by nutrients. We assessed the associations between consumption of carbohydrate, total fat, and each type of fat with X Zhang MSc, Prof K K Teo MD,
cardiovascular disease and total mortality. We calculated hazard ratios (HRs) using a multivariable Cox frailty model S Rangarajan MSc,
with random intercepts to account for centre clustering. S I Bangdiwala PhD, S Islam MSc,
Prof S Yusuf DPhil); Department
of Health Research Methods,
Findings During follow-up, we documented 5796 deaths and 4784 major cardiovascular disease events. Higher Evidence, and Impact,
carbohydrate intake was associated with an increased risk of total mortality (highest [quintile 5] vs lowest quintile McMaster University,
Hamilton, ON, Canada
[quintile 1] category, HR 1·28 [95% CI 1·12–1·46], ptrend=0·0001) but not with the risk of cardiovascular disease or
(A Mente); St John’s Research
cardiovascular disease mortality. Intake of total fat and each type of fat was associated with lower risk of total mortality Institute, St John’s National
(quintile 5 vs quintile 1, total fat: HR 0·77 [95% CI 0·67–0·87], ptrend<0·0001; saturated fat, HR 0·86 [0·76–0·99], Academy of Health Sciences,
ptrend=0·0088; monounsaturated fat: HR 0·81 [0·71–0·92], ptrend<0·0001; and polyunsaturated fat: HR 0·80 [0·71–0·89], Sarjapur Road, Koramangala,
Bangalore, Karnataka, India
ptrend<0·0001). Higher saturated fat intake was associated with lower risk of stroke (quintile 5 vs quintile 1, HR 0·79 [95% CI
(S Swaminathan PhD); State Key
0·64–0·98], ptrend=0·0498). Total fat and saturated and unsaturated fats were not significantly associated with risk of Laboratory of Cardiovascular
myocardial infarction or cardiovascular disease mortality. Disease, Fuwai Hospital,
National Center for
Cardiovascular Disease, Peking
Interpretation High carbohydrate intake was associated with higher risk of total mortality, whereas total fat and
Union Medical College &
individual types of fat were related to lower total mortality. Total fat and types of fat were not associated with Chinese Academy of Medical
cardiovascular disease, myocardial infarction, or cardiovascular disease mortality, whereas saturated fat had an Sciences, Beijing, China
inverse association with stroke. Global dietary guidelines should be reconsidered in light of these findings. (Prof W Li PhD, X Liu PhD,
N Gao BSc, Y Sun MSc); Madras
Diabetes Research Foundation,
Funding Full funding sources listed at the end of the paper (see Acknowledgments). Chennai, India
(Prof V Mohan MD);
Introduction studies done in European and North American countries Departments of Community
Health Sciences and Medicine,
Cardiovascular disease is a global epidemic with 80% of such as Finland, where the intake of saturated fatty Aga Khan University, Karachi,
the burden of disease in low-income and middle-income acids (about 20% of total energy intake) and cardio Pakistan (R Iqbal PhD); PGIMER
countries.1 Diet is one of the most important modifiable vascular disease mortality were both very high.4 Further School of Public Health,
risk factors for cardiovascular disease and other non- more, dietary recommendations are based on the Chandigarh, India (Prof
R Kumar MD); Centre of
communicable diseases and current guidelines recom assumption of a linear association between saturated Excellence for Nutrition,
mend a low-fat diet (<30% of energy) and limiting fatty acid intake and LDL cholesterol, and then the Faculty of Health Sciences,
saturated fatty acids to less than 10% of energy intake by association between LDL cholesterol and cardiovascular North-West University,
replacing them with unsaturated fatty acids.2 However, disease events. However, this assumption does not Potchefstroom, South Africa
(E Wentzel-Viljoen PhD);
recommendations on lowering saturated fatty acids are consider the effect of saturated fatty acids on other Department of Molecular and
largely based on one ecological study3 and observational lipoproteins (eg, HDL cholesterol), ratio of total
www.thelancet.com Published online August 29, 2017 http://dx.doi.org/10.1016/S0140-6736(17)32252-3 1
Articles
Clinical Medicine, Sahlgrenska
Academy, University of Research in context
Gothenburg, Sweden
(Prof A Rosengren MD); Health Evidence before this study American and European countries where nutrition excess is of
Action by People TC 1/1706, We did a systematic search in PubMed for relevant articles concern. It is not clear whether this can be extrapolated to other
Medical College PO, published between Jan 1, 1960, and May 1, 2017, restricted to countries where undernutrition is common. Moreover, North
Trivandrum, India
(L I Amma MD); Dante
the English language. Our search terms included “carbohydrate”, American and European populations consume a lower
Pazzanese Institute of “total fat”, “saturated fatty acid”, “monounsaturated fatty acid”, carbohydrate diet than populations elsewhere where most
Cardiology, Sao Paulo, Brazil “polyunsaturated fatty acid”, “total mortality”, and people consume very high carbohydrate diets mainly from
(Prof A Avezum MD); University “cardiovascular disease”. We searched published articles by title refined sources. Consistent with most data, but in contrast to
of Zimbabwe, College of Health
Sciences, Department of
and abstract to identify relevant studies. We also hand-searched dietary guidelines, we found fats, including saturated fatty
Physiology, Harare, Zimbabwe reference lists of eligible studies. We considered studies if they acids, are not harmful and diets high in carbohydrate have
(J Chifamba DPhil); Estudios evaluated association between macronutrient intake and total adverse effects on total mortality. We did not observe any
Clínicos Latinoamérica, ECLA, mortality or cardiovascular disease. The studies cited in this detrimental effect of higher fat intake on cardiovascular events.
Rosario, Argentina (R Diaz MD);
Institute of Community and
report are not an exhaustive list of existing research. Existing Our data across 18 countries adds to the large and growing
Public Health, Birzeit evidence on the associations of fats and carbohydrate intake body of evidence that increased fats are not associated with
University, Birzeit , occupied with cardiovascular disease and mortality are mainly from North higher cardiovascular disease or mortality.
Palestinian territory America and Europe.
(R Khatib PhD); Faculty of Implications of all the available evidence
Health Sciences, Department of Added value of this study Removing current restrictions on fat intake but limiting
Biomedical Physiology &
Current guidelines recommend a low fat diet (<30% of energy) carbohydrate intake (when high) might improve health. Dietary
Kinesiology, Simon Fraser
University, Burnaby, BC, and limiting saturated fatty acids to less than 10% of energy guidelines might need to be reconsidered in light of consistent
Canada (Prof S Lear PhD); intake by replacing them with unsaturated fatty acids. findings from the present study, especially in countries outside
Fundacion Oftalmologica de The recommendation is based on findings from some North of Europe and North America.
Santander-FOSCAL,
Floridablanca-Santander,
Colombia cholesterol to HDL cholesterol, or on apolipoproteins
(Prof P Lopez-Jaramillo MD);
Eternal Heart Care Centre and
(which could be a better marker of cardiovascular Methods
Research Institute, Jaipur, India disease risk)5,6 and blood pressure, which also affect the Study design and participants
(Prof R Gupta MD); Isfahan risk of cardiovascular disease.7 The design and methods of the PURE study have been
Cardiovascular Research Recently, several meta-analyses of randomised trials described previously.1,14–16 PURE recruitment occurred
Centre, Cardiovascular
and prospective cohort studies8–10 and ecological between Jan 1, 2003, and March 31, 2013, and included
Research Institute, Isfahan
University of Medical Sciences, studies,11 largely done in European and North American individuals aged 35–70 years from 18 low-income,
Isfahan, Iran countries, showed either no association or a lower risk middle-income, and high-income countries on five
(N Mohammadifard PhD); between saturated fatty acid consumption with total continents. We aimed to include populations that varied
Istanbul Medeniyet University,
Faculty of Medicine,
mortality and cardiovascular disease events.12,13 The by socioeconomic factors while ensuring feasibility of
Department of Internal uncertainty regarding the effect of saturated fatty acids long-term follow-up when selecting the participating
Medicine, Goztepe, Istanbul, on clinical outcomes in part might be due to the fact countries. We included three high-income (Canada,
Turkey (A Oguz MD); Faculty of that most observational cohort studies have been done Sweden, and United Arab Emirates), 11 middle-income
Medicine, Universiti Teknologi
MARA, Selangor, Malaysia
in high-income countries8,9 where saturated fatty acid (Argentina, Brazil, Chile, China, Colombia, Iran,
(A S Ramli MD); Universidad de intake is within a limited range (about 7–15% of Malaysia, occupied Palestinian territory, Poland, South
La Frontera, Temuco, energy). Furthermore, it is not known whether findings Africa, and Turkey) and four low-income countries
Araucanía, Chile (P Seron PhD); obtained from European and North American countries (Bangladesh, India, Pakistan, and Zimbabwe), based on
Division of Angiology, Wroclaw
Medical University, Wroclaw,
where nutritional excess is more common, can be gross national income per capita from the World Bank
Poland (Prof A Szuba MD); extrapolated to other regions of the world where classification for 2006 when the study was initiated.
University of the Western Cape, nutritional inadequacy might be more common. The Additional countries have joined PURE, but since follow-
Bellville, Western Province, Prospective Urban Rural Epidemiology (PURE) study up in these countries is incomplete, they are not included
Cape Town, South Africa
(L Tsolekile MPH); University of
provides a unique opportunity to study the impact of in the present analyses. The study was coordinated by the
Ottawa Department of diet on total mortality and cardiovascular disease in Population Health Research Institute (PHRI; Hamilton
Medicine, Ottawa, ON, Canada diverse settings, such as those where overnutrition is Health Sciences, Hamilton, ON, Canada). More details of
(Prof A Wielgosz MD); common and where undernutrition is of greater the sampling and recruitment strategy used in PURE are
Independent University,
Bangladesh, Dhaka,
concern. In this study, our primary aim was to assess detailed in the Article by Miller and colleagues17 and an
Bangladesh (R Yusuf PhD); the association of fats (total, saturated fatty acids, and earlier report.18
Dubai Medical University, unsaturated fats) and carbohydrate with total mortality
Hatta Hospital, Dubai Health
and cardiovascular disease events. The secondary aim Procedures
Authority, Dubai, United Arab
Emirates was to examine associations between these nutrients Data were collected at the community, household, and
(A Hussein Yusufali MD); and myocardial infarction, stroke, cardiovascular individual levels. Within participating communities,
Université Laval, Institut disease mortality, and non-cardiovascular disease our goal was to enrol an unbiased sample of households.
Universitaire de Cardiologie,
mortality. Households were eligible if at least one member was
2 www.thelancet.com Published online August 29, 2017 http://dx.doi.org/10.1016/S0140-6736(17)32252-3
Articles
between 35 and 70 years of age, and the household stroke, cardiovascular disease mortality, and non-cardio Ville de Québec, QC, Canada
intended to stay in the current address for another vascular disease mortality. The numbers of cases of heart (G Dagenais MD); and
Department of Medicine,
4 years. Standardised questionnaires were used to failure were too few to be analysed separately. McMaster University,
collect information about demographic factors, The follow-up period varied based on the date when Hamilton, ON, Canada
socioeconomic status (education, income, and recruitment began at each site or country. During the (Prof S S Anand)
employment), lifestyle (smoking, physical activity, and follow-up period contact was made with every participant Correspondence to:
alcohol intake), health history, and medication use. on an annual basis either by telephone or by a face-to- Dr Mahshid Dehghan, Population
Health Research Institute,
Physical activity was assessed using the International face interview with the local research team. The median
DBCVS Research Institute,
Physical Activity Questionnaire.19 History of diabetes duration of follow-up was 7·4 years (IQR 5·3–9·3), which McMaster University,
was self-reported. Physical assessment included weight, varied across countries (appendix p 22). Room C1-102, 237 Barton Street
height, waist and hip circumferences, and blood East, Hamilton, ON, L8L 2X2,
Canada
pressure. Detailed follow-up occurred at 3, 6, and 9 years Statistical analysis mahshid.dehghan@phri.ca
and repeated measures of selected risk factors, causes of Continuous variables were expressed as means (SDs)
death, other health outcomes, and community data and categorical variables as percentages. Education was See Online for appendix
were collected. Standard ised case-report forms were categorised as none, primary school (first 6 years), or
used to record data on major cardiovascular events and secondary school (7–11 years) and college, trade school,
mortality during follow-up, which were adjudicated or university (>11 years). Smoking was categorised as
centrally in each country by trained physicians using never, former, or current smoker. Physical activity was
standard definitions (appendix pp 8–17). Data were categorised based on the metabolic equivalent of task
electronically transferred to the PHRI where quality (MET) per min per week into low (<600 MET min
control checks were undertaken. per week), moderate (600–3000 MET min per week), and
Participants’ habitual food intake was recorded using high (>3000 MET min per week) activity. Waist-to-hip
country-specific (or region-specific in India) validated ratio (waist circumferences [cm]/hip circumferences
food frequency questionnaires (FFQs) at baseline. [cm]) was used as a continuous variable. Since food
Where a validated FFQ was not available (ie, Argentina), patterns are culture dependent and dietary patterns
we developed and validated FFQs using a standard are generally related to geographical region rather
method.20–30 Multiple 24-h dietary recalls were used as than income region, we categorised countries into
the reference method to validate the FFQs in about seven regions. Regions included China, south Asia
60–250 participants from each country (appendix p 18). (Bangladesh, India, and Pakistan), North America,
To convert food into nutrients, country-specific nutrient Europe (Canada, Poland, and Sweden), South America
databases were constructed with information on (Argentina, Brazil, Chile, and Colombia), Middle East
43 macronutrients and micronutrients. The nutrient (Iran, occupied Palestinian territory, Turkey, and United
databases are primarily based on the United States Arab Emirates), southeast Asia (Malaysia), and Africa
Department of Agriculture food composition database (South Africa and Zimbabwe). For the overall analysis,
(release 18 and 21), modified with reference to local food participants were categorised into quintiles of nutrient
composition tables, and supplemented with recipes of intake (carbohydrate, fats, and protein) based on
local mixed dishes.31 However, for Canada, China, India, percentage of energy (% E) provided by nutrients, which
Malaysia, South Africa, Sweden, and Turkey we used the was computed by dividing energy from the nutrient by
nutrient databases that were used for validation of the the total daily energy intake (eg, for carbohydrate,
FFQs. The FFQ was administered together with other %E=([carbohydrate (g) × 4]/total energy intake
questionnaires at the baseline. [kcal]) × 100). To assess the shape of associations between
For the current analysis, we included all outcome events nutrients and events we used restricted cubic splines,
known to us until March 31, 2017. 148 723 participants fitting a restricted cubic spline function with three knots.
completed the FFQ, of which 143 934 participants had We calculated hazard ratios (HRs) using a multivariable
plausible energy intake (500–5000 kcal per day) and had Cox frailty model with random intercepts to account for
no missing values on age and sex. We excluded centre clustering (which also adjusts for region and
1230 participants (0·8% of the cohort) because follow-up country). Estimates of HRs and 95% CIs are presented
information was not available and 7369 participants with for percentage of energy from carbohydrate, total protein,
a history of cardiovascular disease (5·0% of the cohort). total fat, and types of fat. All models were adjusted for
The remaining 135 335 individuals were included in this age and sex. Additionally, all multivariable models were
analysis (appendix p 19). adjusted for education, smoking, physical activity, waist-
to-hip ratio, history of diabetes, urban or rural location,
Outcomes and total energy intake.
The primary outcomes were total mortality and major In subgroup analyses, since higher carbohydrate (but
cardiovascular events (fatal cardiovascular disease, non- lower fat) consumption is more common in Asian
fatal myocardial infarction, stroke, and heart failure). countries32,33 and lower carbohydrate intake (and higher
Secondary outcomes were all myocardial infarctions, fat) in non-Asian countries11 we examined whether the
www.thelancet.com Published online August 29, 2017 http://dx.doi.org/10.1016/S0140-6736(17)32252-3 3
Articles
effect of carbohydrate and fats on outcomes were region subgroup analyses due to low statistical power to
consistent in these two regions. The countries in Asia detect subgroup interactions). Since the impact of
included Bangladesh, China, India, Malaysia, and macronutrient intake on outcome events might or might
Pakistan; the remaining countries were considered to be not occur through changes in waist-to-hip ratio, we
non-Asian countries. We used this approach for two main excluded waist-to-hip ratio from the multivariable models
reasons: to assess the consistency of the associations in secondary analyses to assess the impact on estimates.
across regions representing different levels of nutrient The effect of isocaloric replacement (as 5% of energy) of
intake, with Asian countries characterising higher carbohydrate with saturated and unsaturated fats and
carbohydrate (and lower fat) consumption and non-Asian protein was estimated using multivariable nutrient density
countries capturing lower carbohydrate intake (and models.34 In this modelling approach, the percentage of
higher fat); and to maximise the power within regions energy intake from saturated and unsaturated fats and
(compared with examining effects within smaller protein were included as exposures with total energy as a
geographical regions with fewer people and relatively few covariate. The coefficients in this model indicate change in
events). Participants were categorised into region-specific outcomes by replacement of carbohydrate (as 5% of
quintile categories of nutrient intake based on the intake energy) by other nutrients. For all analyses, the criterion
distribution of participants in Asian and non-Asian for statistical significance was α=0·05. Statistical analyses
countries, with the lowest quintile category used as were done with SAS software, version 9.3. Spline curves
reference group within regions (we did not do further were generated with the SAS LGTPHCURV9 Macro.
Overall China South Asia Europe and South America Middle East Southeast Asia Africa (n=4558)
(n=135 335) (n=42 152) (n=29 560) North America (n=22 626) (n=11 485) (n=10 038)
(n=14 916)
Age (years) 50·29 (9·92) 50·58 (9·82) 48·18 (10·24) 53·01 (9·18) 51·13 (9·69) 48·57 (9·23) 51·47 (9·96) 49·98 (10·35)
Male 56 422 (41·7%) 17 575 (41·7%) 12 887 (43·6%) 6567 (44·0%) 8685 (38·4%) 4930 (42·9%) 4323 (43·1%) 1455 (31·9%)
Urban location 71 300 (52·7%) 20 170 (47·9%) 14 224 (48·1%) 10 488 (70·3%) 12 896 (57·0%) 6526 (56·8%) 4841 (48·2%) 2155 (47·3%)
Systolic blood pressure (mm Hg) 130·9 (22·2) 132·9 (22·2) 125·8 (21·2) 132·0 (20·4) 131·7 (22·7) 127·1 (20·3) 135·2 (23·1) 138·9 (27·5)
Waist-to-hip ratio 0·87 (0·08) 0·86 (0·07) 0·87 (0·09) 0·88 (0·09) 0·890 (0·08) 0·89 (0·09) 0·83 (0·08 ) 0·84 (0·087)
Current smoker 28 410/134 449 9588/41 670 6799/29 468 2256/14 888 4709/22 548 2178/11 485 1532/9943 1348/4447
(21·1%) (23·0%) (23·1%) (15·2%) (20·9%) (19·0%) (15·4%) (30·3%)
Education
Pre-secondary school 57 438/134 981 14 113/42 036 15 135/29 432 1138/14 903 13 298/22 565 6935/11 485 4263/10 032 2556/4528
(42·6%) (33·6%) (51·4%) (7·6%) (58·9%) (60·4%) (42·5%) (56·5%)
Secondary school 51 730/134 981 21 853/42 036 10 239/29 432 4649/14 903 5471/22 565 3114/11 485 4551/10 032 1853/4528
(38·3%) (52·0%) (34·8%) (31·2%) (24·3%) (27·1%) (45·4%) (40·9%)
Post-secondary school 25 813/134 981 6070/42 036 4058/29 432 9116/14 903 3796/22 565 1436/11 485 1218/10 032 119/4528
(19·1%) (14·4%) (13·8%) (61·2%) (16·8%) (12·5%) (12·1%) (2·6%)
Physical activity
Low (<600 MET per min per week) 22 022/125 945 6424/41 534 5588/25 999 826/13 628 2889/21 567 2452/11 342 3315/9428 528/2447
(17·5%) (15·5%) (21·5%) (6·1%) (13·4%) (21·6%) (35·2%) (21·6%)
Moderate (600–3000 MET per min 47 850/125 945 17 518/41 534 8903/25 999 4757/13 628 6944/21 567 5290/11 342 3336/9428 1102/2447
per week) (38·0%) (42·2%) (34·2%) (34·9%) (32·2%) (46·6%) (35·4%) (45·0%)
High (>3000 MET per min per week) 56 073/125 945 17 592/41 534 11 508/25 999 8045/13 628 11 734/21 567 3600/11 342 2777/9428 817/2447
(44·5%) (42·4%) (44·3%) (59·0%) (54·4%) (31·7%) (29·5%) (33·4%)
History of diabetes 9634 (7·1%) 1610 (3·8%) 2723 (9·2%) 785 (5·3%) 1530 (6·8%) 1405 (12·2%) 1351 (13·5%) 230 (5·1%)
Energy from carbohydrate (%) 61·2% (11·6) 67·0% (9·8) 65·4% (11·3) 52·4% (8·1) 57·6% (11·4) 53·5% (7·5) 53·9% (8·2) 63·3% (11·5)
Energy from fat (%) 23·5% (9·3) 17·7% (7·8) 22·7% (10·4) 30·5% (6·0) 25·2% (7·7) 30·3% (6·1) 29·2% (5·9) 22·8% (8·3)
Energy from protein (%) 15·2% (3·6) 15·3% (2·3) 11·6% (1·9) 16·7% (2·7) 17·5% (3·8) 16·9% (2·8) 17·1% (3·2) 13·4% (3·0)
Energy from saturated fatty acids (%) 8·0% (4·1) 5·7% (2·7) 8·4% (5·2) 10·9% (3·7) 8·9% (3·4) 10·2% (2·9) 9·2% (2·1) 5·9% (2·8)
Energy from monounsaturated fatty 8·1% (3·7) 6·8% (2·9) 5·9% (3·1) 11·2% (2·6) 9·0% (3·2) 10·2% (3·0) 11·8% (3·9) 7·2% (3·2)
acids (%)
Energy from polyunsaturated fatty 5·3% (3·0) 4·2% (2·8) 6·2% (4·0) 4·8% (1·3) 4·4% (1·6) 7·0% (1·9) 8·2% (2·0) 6·0% (2·9)
acids (%)
Energy from protein (%) 15·2% (3·6) 15·3% (2·8) 11·7% (1·9) 16·7% (2·7) 17·5% (3·8) 16·9% (2·8) 17·2% (3·2) 13·4% (3·0)
Energy from animal protein (%) 6·4% (4·5) 5·6% (3·4) 1·9% (1·9) 9·3% (3·0) 10·5% (4·9) 8·9% (3·0) 7·3% (3·1) 5·2% (3·1)
Energy from plant protein (%) 8·8% (2·2) 9·7% (1·5) 9·8% (2·1) 7·4% (2·0) 7·0% (2·3) 8·0% (1·3) 9·8% (2·2) 7·5% (1·4)
Data are mean (SD), n (%), or n/N (%). MET=metabolic equivalents.
Table 1: Characteristics of the study participants at baseline by region and overall
4 www.thelancet.com Published online August 29, 2017 http://dx.doi.org/10.1016/S0140-6736(17)32252-3
Articles
Role of the funding sources were responsible for the decision to submit for
The funders and sponsors had no role in the design publication.
and conduct of the study; in the collection, analysis,
and interpretation of the data; in the preparation, Results
review, or approval of the manuscript; or in the decision During a median follow-up of 7·4 years (IQR 5·3–9·3),
to submit the manuscript for publication. MD, AM, XZ, 5796 individuals died and 4784 had a major cardiovascular
SR, SIB, SSA, and SY had full access to the data and disease event (2143 myocardial infarctions and 2234 strokes).
Incidence (per 1000 person-years; 95% CI) Hazard ratio (95% CI) ptrend
Quintile 1 Quintile 2 Quintile 3 Quintile 4 Quintile 5 Quintile 2 vs Quintile 3 vs Quintile 4 vs Quintile 5 vs
quintile 1 quintile 1 quintile 1 quintile 1
Percentage energy from carbohydrate
Median (IQR) 46·4% 54·6% 60·8% 67·7% 77·2% ·· ·· ·· ·· ··
(42·6–49·0) (52·9–56·2) (59·3–62·3) (65·7–69·7) (74·4–80·7)
Total mortality 4·1 4·2 4·5 4·9 7·2 1·07 1·06 1·17 1·28 0·0001
(3·8–4·3) (3·9–4·5) (4·2–4·8) (4·6–5·2) (6·9–7·5) (0·96–1·20) (0·94–1·19) (1·03–1·32) (1·12–1·46)
Major cardiovascular disease 3·9 4·2 4·2 4·6 5·1 1·00 1·02 1·08 1·01 0·62
(3·6–4·2) (3·9–4·5) (3·9–4·5) (4·3–4·8) (4·8–5·4) (0·90–1·12) (0·91–1·14) (0·96–1·22) (0·88–1·15)
Myocardial infarction 2·0 2·2 2·0 1·8 2·1 0·93 0·92 0·99 0·90 0·40
(1·8–2·2) (2·0–2·4) (1·8–2·2) (1·6–2·0) (1·9–2·3) (0·80–1·09) (0·78–1·09) (0·83–1·18) (0·73–1·10)
Stroke 1·4 1·6 1·8 2·4 2·7 1·03 1·09 1·21 1·11 0·10
(1·3–1·6) (1·4–1·7) (1·6–2·0) (2·2–2·6) (2·5–2·9) (0·86–1·22) (0·91–1·31) (1·01–1·45) (0·92–1·35)
Cardiovascular disease mortality 1·3 1·6 1·4 1·3 1·7 1·18 1·02 1·11 1·13 0·50
(1·1–1·4) (1·4–1·7) (1·3–1·6) (1·2–1·5) (1·5–1·9) (0·97–1·43) (0·83–1·26) (0·88–1·38) (0·89–1·44)
Non-cardiovascular disease 2·5 2·3 2·7 3·2 5·1 1·00 1·09 1·22 1·36 <0·0001
mortality (2·3–2·7) (2·1–2·5) (2·5–2·9) (3·0–3·5) (4·8–5·4) (0·87–1·15) (0·94–1·27) (1·05–1·42) (1·16–1·60)
Percentage energy from total fat
Median (IQR) 10·6% 18·0% 24·2% 29·1% 35·3% ·· ·· ·· ·· ··
(8·1–12·6) (16·3–19·7) (22·8–25·5) (27·9–30·3) (33·3–38·3)
Total mortality 6·7 5·1 4·6 4·3 4·1 0·90 0·81 0·80 0·77 <0·0001
(6·4–7·0) (4·7–5·4) (4·3–5·0) (4·0–4·6) (3·9–4·4) (0·82–0·98) (0·73–0·90) (0·71–0·90) (0·67–0·87)
Major cardiovascular disease 5·3 4·3 4·2 4·0 4·1 1·01 1·01 0·95 0·95 0·33
(5·0–5·6) (4·0–4·6) (3·9–4·5) (3·8–4·3) (3·8–4·4) (0·92–1·11) (0·90–1·13) (0·84–1·07) (0·83–1·08)
Myocardial infarction 2·1 1·6 2·0 2·0 2·3 1·02 1·08 0·97 1·12 0·40
(1·9–2·3) (1·4–1·8) (1·8–2·2) (1·8–2·2) (2·1–2·6) (0·87–1·20) (0·90–1·29) (0·80–1·18) (0·92–1·37)
Stroke 3·0 2·3 1·6 1·6 1·3 1·05 0·91 0·95 0·82 0·05
(2·7–3·2) (2·1–2·6) (1·5–1·8) (1·4–1·8) (1·2–1·5) (0·93–1·19) (0·78–1·06) (0·79–1·13) (0·68–1·00)
Cardiovascular disease mortality 1·6 1·3 1·5 1·4 1·5 0·89 0·92 0·88 0·92 0·50
(1·4–1·8) (1·2–1·5) (1·3–1·6) (1·3–1·6) (1·3–1·7) (0·74–1·06) (0·75–1·12) (0·70–1·10) (0·72–1·16)
Non-cardiovascular disease 4·7 3·4 2·9 2·6 2·3 0·91 0·78 0·78 0·70 <0·0001
mortality (4·4–5·0) (3·1–3·6) (2·6–3·1) (2·3–2·8) (2·1–2·5) (0·82–1·01) (0·69–0·89) (0·67–0·90) (0·60–0·82)
Percentage energy from total protein
Median (IQR) 10·8% 13·1% 15·0% 16·9% 19·7% ·· ·· ·· ·· ··
(9·9–11·5) (12·6–13·6) (14·5–15·5) (16·4–17·4) (18·8–21·4)
Total mortality 8·5 5·4 3·7 3·2 3·6 1·05 0·92 0·85 0·88 0·0030
(8·1–8·9) (5·1–5·7) (3·5–4·0) (2·9–3·4) (3·3–3·9) (0·96–1·15) (0·82–1·03) (0·75–0·96) (0·77–1·00)
Major cardiovascular disease 5·0 4·6 4·4 4·2 3·7 1·02 1·08 1·09 0·96 0·86
(4·7–5·3) (4·3–4·9) (4·1–4·7) (3·9–4·5) (3·5–4·0) (0·91–1·13) (0·96–1·22) (0·97–1·24) (0·84–1·10)
Myocardial infarction 2·8 2·0 1·7 1·7 1·7 1·04 1·01 1·11 1·02 0·67
(2·5–3·0) (1·8–2·2) (1·5–1·9) (1·5–1·9) (1·5–1·9) (0·89–1·20) (0·85–1·20) (0·92–1·33) (0·83–1·24)
Stroke 1·8 2·2 2·4 2·1 1·6 1·01 1·14 1·11 0·90 0·47
(1·6–2·0) (2·0–2·4) (2·1–2·6) (1·9–2·3) (1·4–1·8) (0·86–1·19) (0·96–1·36) (0·92–1·33) (0·74–1·09)
Cardiovascular disease mortality 2·4 1·7 1·0 0·9 1·1 1·09 0·89 0·92 0·90 0·26
(2·2–2·6) (1·5–1·9) (0·9–1·2) (0·8–1·1) (0·9–1·2) (0·93–1·29) (0·73–1·10) (0·74–1·16) (0·71–1·15)
Non-cardiovascular disease 5·5 3·3 2·5 2·0 2·3 1·02 0·92 0·79 0·85 0·0022
mortality (5·2–5·8) (3·1–3·6) (2·2–2·7) (1·8–2·2) (2·1–2·5) (0·91–1·15) (0·80–1·05) (0·68–0·93) (0·73–0·99)
Hazard ratios and 95% CIs are adjusted for age, sex, education, waist-to-hip ratio, smoking, physical activity, diabetes, urban or rural location, and energy intake. Centre was also included as a random effect and
frailty models were used. Major cardiovascular disease=fatal cardiovascular disease+myocardial infarction+stroke+heart failure.
Table 2: Association between percentage energy from macronutrients and clinical outcomes (n=135 335)
www.thelancet.com Published online August 29, 2017 http://dx.doi.org/10.1016/S0140-6736(17)32252-3 5
Articles
1649 died due to cardiovascular disease and 3809 died due by respiratory diseases. In Africa, infectious disease was the
to non-cardiovascular disease. There were 338 deaths due to first and respiratory disease was the second most common
injury, which were not included in non-cardiovascular cause of non-cardiovascular disease mortality.
disease mortality because these were considered to be The characteristics of participants and data on macro
unlikely to be associated with diet. Among non- nutrient intake are presented in table 1.
cardiovascular disease mortality, in all regions except Africa, Carbohydrate intake was higher in China, south Asia, and
the most common cause of mortality was cancer followed Africa compared with other regions. In south Asia about
Incidence (per 1000 person-years; 95% CI) Hazard ratio (95% CI) ptrend
Quintile 1 Quintile 2 Quintile 3 Quintile 4 Quintile 5 Quintile 2 vs Quintile 3 vs Quintile 4 vs· Quintile 5 vs
quintile 1 quintile 1 quintile 1 quintile 1
Percentage energy from saturated fatty acids
Median (IQR) 2·8% 4·9% 7·1% 9·5% 13·2% ·· ·· ·· ·· ··
(2·0–3·4) (4·4–5·5) (6·5–7·7) (8·9–10·2) (11·9–15·1)
Total mortality 7·1 5·2 4·3 3·9 4·4 0·96 0·92 0·85 0·86 0·0088
(6·7–7·4) (4·9–5·5) (4·0–4·6) (3·6–4·2) (4·1–4·7) (0·88–1·05) (0·83–1·02) (0·75–0·95) (0·76–0·99)
Major cardiovascular disease 5·2 4·7 4·1 3·9 4·1 1·13 1·06 1·03 0·95 0·49
(4·9–5·5) (4·4–5·1) (3·8–4·4) (3·6–4·2) (3·8–4·4) (1·02–1·25) (0·95–1·18) (0·91–1·17) (0·83–1·10)
Myocardial infarction 2·1 1·8 1·7 1·9 2·5 1·28 1·20 1·16 1·17 0·40
(1·9–2·3) (1·6–2·0) (1·5–1·9) (1·7–2·1) (2·3–2·7) (1·08–1·51) (1·00–1·44) (0·95–1·41) (0·94–1·45)
Stroke 2·7 2·6 1·9 1·5 1·3 1·10 1·01 0·93 0·79 0·0498
(2·5–2·9) (2·3–2·8) (1·7–2·1) (1·4–1·7) (1·1–1·4) (0·97–1·25) (0·87–1·17) (0·78–1·11) (0·64–0·98)
Cardiovascular disease mortality 1·7 1·5 1·3 1·4 1·4 1·04 0·95 0·99 0·83 0·20
(1·6–1·9) (1·4–1·7) (1·1–1·4) (1·2–1·5) (1·2–1·6) (0·87–1·24) (0·78–1·17) (0·79–1·23) (0·65–1·07)
Non-cardiovascular disease 4·9 3·4 2·8 2·3 2·6 0·94 0·91 0·78 0·86 0·0108
mortality (4·6–5·2) (3·1–3·6) (2·5–3·0) (2·1–2·5) (2·4–2·8) (0·84–1·04) (0·81–1·03) (0·68–0·91) (0·73–1·01)
Percentage energy from monounsaturated fatty acids
Median (IQR) 3·4% 5·4% 7·3% 9·5% 12·5% ·· ·· ·· ·· ··
(2·4–4·0) (5·0–5·9) (6·8–7·8) (8·9–10·1) (11·5–13·8)
Total mortality 7·5 5·6 4·4 3·7 3·7 1·02 0·91 0·81 0·81 <0·0001
(7·2–7·9) (5·3–5·9) (4·1–4·7) (3·4–4·0) (3·4–3·9) (0·93–1·11) (0·82–1·00) (0·72–0·91) (0·71–0·92)
Major cardiovascular disease 5·2 4·6 4·5 3·9 3·8 1·04 1·06 1·02 0·95 0·54
(4·9–5·5) (4·3–4·9) (4·2–4·8) (3·6–4·2) (3·6–4·1) (0·94–1·15) (0·95–1·18) (0·90–1·15) (0·84–1·09)
Myocardial infarction 2·4 2·0 1·9 1·8 1·9 1·09 1·13 1·04 1·12 0·40
(2·2–2·7) (1·8–2·2) (1·7–2·1) (1·6–2·0) (1·7–2·1) (0·93–1·28) (0·95–1·34) (0·86–1·25) (0·92–1·38)
Stroke 2·5 2·3 2·1 1·6 1·5 1·03 1·00 0·99 0·85 0·10
(2·3–2·7) (2·1–2·5) (1·9–2·3) (1·5–1·8) (1·3–1·6) (0·90–1·18) (0·86–1·16) (0·83–1·17) (0·70–1·03)
Cardiovascular disease mortality 1·9 1·7 1·4 1·3 1·1 1·07 0·98 0·90 0·85 0·10
(1·7–2·1) (1·5–1·8) (1·3–1·6) (1·1–1·4) (0·9–1·2) (0·90–1·26) (0·81–1·18) (0·73–1·12) (0·66–1·09)
Non-cardiovascular disease 5·2 3·5 2·6 2·2 2·4 1·00 0·86 0·77 0·79 0·0003
mortality (4·9–5·5) (3·3–3·8) (2·4–2·8) (2·0–2·4) (2·1–2·6) (0·90–1·11) (0·76–0·97) (0·67–0·89) (0·68–0·93)
Percentage energy from polyunsaturated fatty acids
Median (IQR) 2·1% 3·3% 4·4% 5·7% 8·5% ·· ·· ·· ·· ··
(1·6–2·5) (3·1–3·6) (4·1–4·7) (5·4–6·2) (7·5–10·4)
Total mortality 5·8 4·8 4·6 5·0 4·9 0·92 0·87 0·85 0·80 <0·0001
(5·5–6·2) (4·5–5·1) (4·3–4·9) (4·6–5·3) (4·6–5·2) (0·84–1·01) (0·79–0·96) (0·77–0·94) (0·71–0·89)
Major cardiovascular disease 5·4 3·9 4·0 4·2 4·7 1·01 0·99 0·97 1·01 0·94
(5·1–5·8) (3·6–4·2) (3·7–4·3) (3·9–4·5) (4·4–5·0) (0·91–1·11) (0·89–1·10) (0·87–1·09) (0·90–1·14)
Myocardial infarction 2·2 1·6 1·7 2·0 2·7 1·02 1·05 0·98 1·12 0·40
(2·0–2·4) (1·4–1·8) (1·6–1·9) (1·8–2·2) (2·4–2·9) (0·86–1·21) (0·88–1·25) (0·82–1·17) (0·93–1·34)
Stroke 3·0 1·9 1·7 1·7 1·6 0·96 0·94 0·95 0·92 0·30
(2·8–3·2) (1·7–2·1) (1·6–1·9) (1·5–1·9) (1·5–1·8) (0·84–1·09) (0·81–1·08) (0·81–1·11) (0·78–1·09)
Cardiovascular disease mortality 1·5 1·3 1·3 1·4 1·9 0·99 0·88 0·81 0·94 0·20
(1·3–1·6) (1·1–1·5) (1·2–1·5) (1·2–1·6) (1·7–2·1) (0·82–1·19) (0·72–1·07) (0·67–0·99) (0·76–1·15)
Non-cardiovascular disease 4·0 3·2 3·0 3·2 2·6 0·90 0·86 0·88 0·75 0·0002
mortality (3·7–4·3) (3·0–3·5) (2·7–3·2) (3·0–3·5) (2·4–2·8) (0·80–1·00) (0·76–0·96) (0·78–0·99) (0·65–0·86)
Hazard ratios and 95% CIs are adjusted for age, sex, education, waist-to-hip ratio, smoking, physical activity, diabetes, urban or rural location, and energy intake. Centre was also included as a random effect and
frailty models were used. Major cardiovascular disease=fatal cardiovascular disease+myocardial infarction+stroke+heart failure.
Table 3: Association between percentage energy from types of different fat and clinical outcomes (n=135 335)
6 www.thelancet.com Published online August 29, 2017 http://dx.doi.org/10.1016/S0140-6736(17)32252-3
Articles
Total mortality Total mortality Total mortality Total mortality Total mortality
1·8
1·5
Relative risk (95% CI)
1·2
0·9
0·6
0·3
Major cardiovascular disease Major cardiovascular disease Major cardiovascular disease Major cardiovascular disease Major cardiovascular disease
1·5
1·2
Relative risk (95% CI)
0·9
0·6
0·3
0 5 10 15 20 25 30 35 40 45 0 2 4 6 8 10 12 14 16 18 0 2 4 6 8 10 12 14 16 18 0 2 4 6 8 10 12 14 40 50 60 70 80 90
Energy from total Energy from saturated Energy from monounsaturated Energy from polyunsaturated Energy from carbohydrate
fat (%) fatty acids (%) fatty acids (%) fatty acids (%) (%)
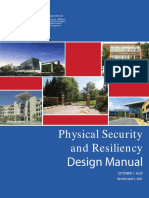
Figure 1: Association between estimated percentage energy from nutrients and total mortality and major cardiovascular disease (n=135 335)
Adjusted for age, sex, education, waist-to-hip ratio, smoking, physical activity, diabetes, urban or rural location, centre, geographical regions, and energy intake.
Major cardiovascular disease=fatal cardiovascular disease+myocardial infarction+stroke+heart failure.
65% of the population consume at least 60% of energy from 0·77–1·00]; ptrend=0·0030) and non-cardiovascular disease
carbohydrate and 33% consume at least 70% of energy mortality (HR 0·85 [0·73–0·99]; ptrend=0·0022; table 2).
from carbohydrate, and in China the corresponding Animal protein intake was associated with lower
percentages are 77% and 43% (appendix p 33). The highest risk of total mortality and no significant association
amount of fat consumed was in North America and Europe, was observed between plant protein and risk of total
Middle East, and southeast Asia. Intake of protein was mortality.
highest in South America and southeast Asia. In comparisons between quintile 5 and quintile 1, a
Tables 2 and 3 show nutrient intake and risk of total higher intake of saturated fatty acids was inversely
mortality and cardiovascular disease events. Higher associated with risk of total mortality (HR 0·86 [95% CI
carbohydrate intake was associated with higher risk of 0·76–0·99]; ptrend=0·0088), stroke (HR 0·79 [0·64–0·98];
total mortality (quintile 5 vs quintile 1, HR 1·28 [95% CI ptrend=0·0498), and non-cardiovascular disease mortality
1·12–1·46]; ptrend=0·0001) and non-cardiovascular disease (HR 0·86 [0·73–1·01]; ptrend=0·0108; table 3). Higher
mortality (quintile 5 vs quintile 1, HR 1·36 [1·16–1·60]; saturated fatty acid intake was not associated with
ptrend<0·0001), after multivariable adjustment for co major cardiovascular disease, myocardial infarction, or
variates (table 2). No significant associations between cardiovascular disease mortality. Similarly, mono
carbohydrate intake and major cardiovascular disease, unsaturated fatty acid intake was associated with lower
myocardial infarction, stroke, and cardiovascular disease risk of total mortality (HR 0·81 [95% CI 0·71–0·92];
mortality were recorded (table 2). ptrend<0·0001), a non-significant trend for lower risk of
In comparisons between quintile 5 and quintile 1, total stroke (HR 0·85 [0·70–1·03]; ptrend=0·10), and lower risk
fat intake was associated with lower risks of total of non-cardiovascular disease mortality (HR 0·79
mortality (HR 0·77 [95% CI 0·67–0·87]; ptrend<0·0001), [0·68–0·92]; ptrend=0·0003). Intake of polyunsaturated
stroke (HR 0·82 [0·68–1·00]; ptrend=0·0562), and non- fatty acids was associated with lower risk of total mortality
cardiovascular disease mortality (HR 0·70 [0·60–0·82]; (HR 0·80 [95% CI 0·71–0·89]; ptrend<0·0001) and non-
ptrend<0·0001). No significant associations between total cardiovascular disease mortality (HR 0·75 [0·65–0·86];
fat intake and major cardiovascular disease, myocardial ptrend=0·0002). Intakes of monounsaturated fatty acids
infarction, and cardiovascular disease mortality were and polyunsaturated fatty acids were not significantly
found. Similarly, total protein intake was inversely associated with major cardiovascular disease, myocardial
associated with risks of total mortality (HR 0·88 [95% CI infarction, and cardiovascular disease mortality.
www.thelancet.com Published online August 29, 2017 http://dx.doi.org/10.1016/S0140-6736(17)32252-3 7
Articles
A B
Percentage energy from carbohydrate HR (95% CI) p trend Percentage energy from total fat HR (95% CI) p trend
Asian regions
Q2 vs Q1 0·92 (0·81–1·05) 0·98 (0·89–1·09)
Q3 vs Q1 0·94 (0·82–1·07) 0·87 (0·77–0·97)
Q4 vs Q1 1·03 (0·90–1·19) 0·84 (0·73–0·96)
Q5 vs Q1 1·09 (0·94–1·26) 0·0644 0·85 (0·74–0·99) 0·0078
Non-Asian regions
Q2 vs Q1 1·10 (0·93–1·31) 0·99 (0·83–1·19)
Q3 vs Q1 1·10 (0·92–1·32) 0·83 (0·68–1·01)
Q4 vs Q1 1·31 (1·08–1·59) 0·82 (0·66–1·01)
Q5 vs Q1 1·31 (1·05–1·63) 0·0061 0·81 (0·66–0·99) 0·0124
0·6 1 1·5 2·0 0·6 1 1·5 2·0
Hazard ratio Hazard ratio
Energy from carbohydrate (%; median [IQR]) Energy from total fat (%; median [IQR])
Q1 Q2 Q3 Q4 Q5 Q1 Q2 Q3 Q4 Q5
Asian region 50·4 58·8 64·9 71·4 79·4 Asian region 8·7 14·5 20·5 26·5 33·5
(46·5–52·9) (57·1–60·3) (63·3–66·5) (69·7–73·3) (77·2–82·2) (6·8–10·3) (13·1–16·0) (18·9–22·1) (25·1–27·9) (31·2–36·9)
Non-Asian region 43·0 50·2 55·3 60·6 69·5 Non-Asian region 17·3 23·7 27·9 31·6 36·9
(39·5–45·3) (48·8–51·5) (54·1–56·6) (59·2–62·3) (66·4–73·6) (14·6–19·3) (22·4–24·9) (27·0–28·9) (30·7–32·6) (35·2–39·6)
C D
Percentage energy from saturated fatty acids Percentage energy from monounsaturated fatty acids
Asian regions
Q2 vs Q1 0·94 (0·84–1·04) 0·98 (0·88–1·08)
Q3 vs Q1 0·86 (0·76–0·96) 1·01 (0·90–1·13)
Q4 vs Q1 0·88 (0·78–1·00) 0·89 (0·79–1·01)
Q5 vs Q1 0·88 (0·76–1·03) 0·0244 0·83 (0·72–0·96) 0·0122
Non-Asian regions
Q2 vs Q1 0·87 (0·73–1·05) 0·94 (0·78–1·13)
Q3 vs Q1 0·82 (0·67–1·00) 0·81 (0·66–0·99)
Q4 vs Q1 0·92 (0·76–1·13) 0·85 (0·69–1·04)
Q5 vs Q1 0·80 (0·65–1·00) 0·1488 0·74 (0·60–0·92) 0·0065
0·6 1 1·5 2·0 0·6 1 1·5 2·0
Hazard ratio Hazard ratio
Energy from saturated fatty acids (%; median [IQR]) Energy from total monounsaturated fatty acid (%; median [IQR])
Q1 Q2 Q3 Q4 Q5 Q1 Q2 Q3 Q4 Q5
Asian region 2·3 3·9 5·5 7·7 12·1 Asian region 2·7 4·5 5·9 7·5 10·5
(1·6–2·8) (3·6–4·3) (5·0–6·0) (7·0–8·4) (10·5–14·3) (2·0–3·3) (4·2–4·9) (5·5–6·2) (7·0–8·1) (9·5–12·0)
Non-Asian region 5·1 7·4 9·2 11·0 14·1 Non-Asian region 5·5 8·0 9·7 11·4 13·8
(4·0–5·8) (7·0–7·9) (8·8–9·6) (10·5–11·6) (13·1–15·9) (4·5–6·3) (7·5–8·4) (9·3–10·1) (11·0–11·9) (13·0–15·0)
E
Percentage energy from polyunsaturated fatty acids
Asian regions
Q2 vs Q1 0·88 (0·79–0·98)
Q3 vs Q1 0·93 (0·83–1·04)
Q4 vs Q1 0·85 (0·75–0·95)
Q5 vs Q1 0·79 (0·69–0·90) 0·0012
Non-Asian regions
Q2 vs Q1 1·00 (0·85–1·19)
Q3 vs Q1 1·00 (0·84–1·20)
Q4 vs Q1 0·92 (0·76–1·12)
Q5 vs Q1 0·96 (0·77–1·19) 0·4564
0·6 1 1·5 2·0
Hazard ratio
Energy from polyunsaturated fatty acids (%; median [IQR])
Q1 Q2 Q3 Q4 Q5
Asian region 1·7 2·8 4·0 5·6 9·2
(1·4–2·0) (2·6–3·1) (3·7–4·3) (5·1–6·1) (7·8–11·5)
Non-Asian region 3·0 4·0 4·8 5·9 7·9
(2·7–3·3) (3·8–4·2) (4·6–5·1) (5·6–6·3) (7·2–8·9)
Figure 2: Associations between (A) carbohydrate, (B) total fat, (C) saturated fatty acids, (D) monounsaturated fatty acids, and (E) polyunsaturated fatty acids
with risk of total mortality in Asia and other regions
Hazard ratios (HRs) and 95% CIs are adjusted for age, sex, education, waist-to-hip ratio, smoking, physical activity, diabetes, urban or rural location, and energy
intake. Centre was also included as a random effect and frailty models were used (p for heterogeneity >0·2 for total fat and >0·5 for carbohydrate, saturated fatty
acids, monounsaturated fatty acids, and polyunsaturated fatty acids). Q1–Q5=quintiles 1–5.
Restricted multivariable cubic spline plots for total outcomes are shown in figure 1 and the appendix
mortality and major cardiovascular disease and other (pp 20, 21). Multivariable splines for total fats and subtypes
8 www.thelancet.com Published online August 29, 2017 http://dx.doi.org/10.1016/S0140-6736(17)32252-3
Articles
showed non-linear, decreasing trends in total mortality A
and major cardiovascular disease outcomes with in Carbohydrate replaced by HR (95% CI)
creasing nutrients. However, multivariable splines for Total mortality
carbohydrate had a non-linear increasing trend in risks of Saturated fatty acids 0·97 (0·90–1·04)
Monounsaturated fatty acids 0·97 (0·88–1·08)
total mortality and major cardiovascular disease (figure 1) Polyunsaturated fatty acids 0·89 (0·82–0·97)
and non-cardiovascular disease mortality (appendix p 21). Protein 0·96 (0·90–1·02)
The rise appeared to occur among those who consumed
Major cardiovascular disease
more than 60% (mid estimate from the spline) when Saturated fatty acids 0·95 (0·89–1·04)
energy intake from carbohydrate exceeded 70% energy Monounsaturated fatty acids 1·00 (0·90–1·11)
Polyunsaturated fatty acids 1·01 (0·94–1·02)
(where the lower CI is above a HR of 1). Protein 0·99 (0·93–1·06)
We investigated the influence of socioeconomic status
and poverty using four different measures of socio B
economic status to adjust in the analysis of the associ Carbohydrate replaced by HR (95% CI)
ations between different nutrient intakes and total Myocardial infarction
mortality and cardiovascular disease events. These were Saturated fatty acids 1·03 (0·91–1·15)
Monounsaturated fatty acids 0·98 (0·84–1·14)
household wealth, household income, education, and Polyunsaturated fatty acids 1·06 (0·95–1·19)
economic level of the country subdivided by urban and Protein 0·98 (0·89–1·08)
rural locations. When we included education in the Stroke
models, the estimates of association were robust. Saturated fatty acids 0·80 (0·69–0·93)
Additionally, we adjusted for study centre as a random Monounsaturated fatty acids 1·14 (0·96–1·35)
Polyunsaturated fatty acids 0·97 (0·86–1·10)
effect which takes into account socioeconomic factors Protein 1·00 (0·90–1·10)
and clustering by community. When we reanalysed the
data using household income, household wealth, or C
economic level of the country our results were unchanged Carbohydrate replaced by HR (95% CI)
(appendix p 34). Cardiovascular disease mortality
Saturated fatty acids 0·88 (0·76–1·00)
Higher carbohydrate intake was associated with higher 1·03 (0·85–1·26)
Monounsaturated fatty acids
risk of total mortality in both Asian countries and non- Polyunsaturated fatty acids 1·04 (0·90–1·20)
Asian countries (figure 2A). Conversely, higher intake of Protein 0·97 (0·86–1·10)
total fat and individual types of fat were each associated Non-cardiovascular disease mortality
with lower total mortality risk in Asian countries and Saturated fatty acids 1·00 (0·92–1·10)
Monounsaturated fatty acids 0·97 (0·84–1·10)
non-Asian countries (figure 2B–E). Polyunsaturated fatty acids 0·84 (0·76–0·94)
Isocaloric (5% of energy) replacement of carbohydrate Protein 0·96 (0·88–1·03)
with polyunsaturated acids was associated with an 0·6 1 1·5
Hazard ratio
11% lower risk of mortality (HR 0·89 [95% CI 0·82–0·97]),
whereas replacement of carbohydrate with saturated fatty Figure 3: Risk of clinical outcomes associated with isocaloric (5% of energy) replacement of carbohydrate
with other nutrients (n=135 335)
acids, monounsaturated acids, or protein was not
Hazard ratios (HRs) and 95% CIs are adjusted for age, sex, education, waist-to-hip ratio, smoking, physical activity,
significantly associated with risk of total mortality. diabetes, urban or rural location, and energy intake. Centre was also included as a random effect and frailty models
Replacement of carbohydrate with different types of fat or were used. Major cardiovascular disease=fatal cardiovascular disease+myocardial infarction+stroke+heart failure.
with protein was not significantly associated with major
cardiovascular disease. Replacement of carbohydrate with Furthermore, higher intakes of individual types of fat
saturated fatty acids was associated with a 20% lower risk were associated with lower total mortality, non-
of stroke (HR 0·80 [95% CI 0·69–0·93]). No significant cardiovascular disease mortality, and stroke risk and
associations with stroke risk were found for replacement were not associated with risk of major cardiovascular
of carbohydrate with other fats and protein. Replacement disease events, myocardial infarction, or cardiovascular
of carbohydrate with polyunsaturated fatty acids was disease mortality. Our findings do not support the
associated with 16% lower risk of non-cardiovascular current recommendation to limit total fat intake to less
disease mortality (HR 0·84 [95% CI 0·76–0·94]; than 30% of energy and saturated fat intake to less than
figure 3A–C). 10% of energy. Individuals with high carbohydrate intake
might benefit from a reduction in carbohydrate intake
Discussion and increase in the consumption of fats.
In this large prospective cohort study from 18 countries For decades, dietary guidelines have focused on
in five continents, we found that high carbohydrate reducing total fat and saturated fatty acid intake, based
intake (more than about 60% of energy) was associated on the presumption that replacing saturated fatty acids
with an adverse impact on total mortality and non- with carbohydrate and unsaturated fats will lower LDL
cardiovascular disease mortality. By contrast, higher fat cholesterol and should therefore reduce cardiovascular
intake was associated with lower risk of total mortality, disease events. This focus is largely based on selective
non-cardiovascular disease mortality, and stroke. emphasis on some observational and clinical data,
www.thelancet.com Published online August 29, 2017 http://dx.doi.org/10.1016/S0140-6736(17)32252-3 9
Articles
despite the existence of several randomised trials and studies showed that replacement of fat with carbohydrate
observational studies that do not support these was not associated with lower risk of coronary heart
conclusions.9,35–37 Moreover, many studies that report disease and a pooled analysis of two large cohort studies
higher risk of coronary heart disease deaths with higher (the Health Professionals Follow up and the Nurses’
saturated fatty acid intake were from North American Health Study)46 showed an inverse association between
and European populations (with relatively high intakes of total fat and total mortality. Furthermore, higher glycaemic
total and saturated fats) where in the past cardiovascular load was shown to be associated with a higher risk of
disease was the major cause of deaths38 and their ischaemic stroke in the Nurses’ Health Study.47 Our
applicability to other populations is uncertain. findings indicate that limiting total fat consumption is
In our study more than half of the participants unlikely to improve health in populations, and a total fat
(52%) consumed a high carbohydrate diet (at least intake of about 35% of energy with concomitant lowering
60% of energy) and about a quarter derive more than 70% of carbohydrate intake might lower risk of total mortality.
of their energy from carbohydrate. This value is higher For individual fats, we found an inverse association
than most previous studies done in North America and between saturated fatty acid intake, total mortality, non-
Europe (appendix p 33). Furthermore, our study cardiovascular disease mortality, and stroke risk without
population represented a broad range of carbohydrate any evidence of an increase in major cardiovascular
intake (mean intake of 46–77% of energy). This might disease, myocardial infarction, and cardiovascular disease
explain the stronger association between carbohydrate mortality. Our spline showed a non-linear association
intake and total mortality in our study compared with between saturated fatty acid intake and outcomes and this
previous studies, which generally included participants suggests that the nature of the relationship is more
with lower mean consumption of carbohydrate and a complex than previously assumed and the risks might
relatively narrower range of carbohydrate intake (35–56% depend on the amount of nutrient consumed. This is the
of energy).39–41 Moreover, in our study most participants first large study to describe the association between low
from low-income and middle-income countries level saturated fatty acid intake (eg, <7% of energy) and
consumed a very high carbohydrate diet (at least total mortality and cardiovascular disease events. Two large
60% of energy), especially from refined sources (such as prospective cohort studies (the Health Professionals
white rice and white bread), which have been shown to be Follow up and the Nurses’ Health Study) did not find
associated with increased risk of total mortality and significant associations between saturated fatty acid intake
cardiovascular events.42 Therefore, recommending and risk of cardiovascular disease when replacement
lowering carbohydrate might be particularly applicable to nutrients were not taken into account.38,39,48,49 Randomised
such settings if replacement foods from fats and protein controlled trials of saturated fatty acid reduction (replaced
are available and affordable. It is also noteworthy that the by polyunsaturated fatty acids) have also not shown a
spline plots showed a non-linear increasing trend in total statistically significant impact on total mortality.9,35–37 Unlike
mortality with a carbohydrate intake and the rise seems to previous studies from North American and European
occur among those who consumed more than 60% of countries, our study covers a much broader range of
energy from carbohydrate (ie, based on the midpoint of saturated fatty acid intake including a large number of
the estimate, with the lower CI showing an HR >0·1 people in the lower range of intake (ie, 50% of participants
when more than 70% of energy came from carbohydrates). consumed less than 7% of energy and 75% of participants
Additionally, higher carbohydrate intakes increase some consumed less than 10% of energy from saturated fatty
forms of dyslipidaemia (ie, higher triglycerides and lower acids compared with 50% of participants with greater than
HDL cholesterol), apolipoprotein B (ApoB)-to- 10% of energy in studies of North American and European
apolipoprotein A1 (ApoA1) ratios and increased small countries). The larger number of people (75%) with lower
dense LDL (the most atherogenic particles)43,44 and saturated fatty acids consumption in PURE allows us to
increased blood pressure45 (see Mente and colleagues45). examine the associations of low saturated fatty acids with
However, the absence of association between low total mortality and cardiovascular disease events. Our
carbohydrate intake (eg, <50% of energy) and health findings of an inverse association between saturated fatty
outcomes does not provide support for very low acid intake and risk of stroke are consistent with some
carbohydrate diets. Importantly, a certain amount of previous cohort studies.50 Collectively, the available data9 do
carbohydrate is necessary to meet short-term energy not support the recommendation to limit saturated fatty
demands during physical activity and so moderate intakes acids to less than 10% of intake and that a very low intake
(eg, 50–55% of energy) are likely to be more appropriate (ie, below about 7% of energy) might even be harmful.
than either very high or very low carbohydrate intakes. We found an inverse association between mono
A high carbohydrate diet is usually accompanied by a unsaturated fatty acid intake and total mortality.
low fat intake. Our findings show a higher risk of total Consistent with our findings, two large cohort studies of
mortality, non-cardiovascular disease mortality, and stroke the Health Professionals Follow up and the Nurses’
by lower fat consumption. The health benefit of replacing Health Study showed lower total mortality by higher
total fat with carbohydrate has been debated. Previous monounsaturated fatty acid intake.46 Furthermore, our
10 www.thelancet.com Published online August 29, 2017 http://dx.doi.org/10.1016/S0140-6736(17)32252-3
Articles
findings are consistent with randomised trials of the direct comparison of nutrients and foods within each
Mediterranean diet that have shown reduced risk of total region included in the study and standardised methods to
mortality and cardiovascular disease among those collect and adjudicate events. However, our study had
consuming higher amounts of olive oil and nuts.51 Higher some limitations. First, we used FFQs to estimate
polyunsaturated fatty acid intake was associated with participants’ dietary intake which is not a measure of
lower total mortality rates and a modest lower risk of absolute intake, but is suited for classifying individuals
stroke. This finding is consistent with the lower total into intake categories and is the most commonly used
mortality among US men and women (the Health approach for assessing intake in epidemiological studies.
Professionals Follow up and the Nurses’ Health Study) Measurement error in reporting might lead to random
and Japanese men,52 as well as a meta-analysis of errors that could dilute real associations between nutrients
randomised clinical trials.53 Extensive adjustment for and clinical events. Second, dietary intakes were measured
socioeconomic status using four different approaches only at baseline, and it is possible that dietary changes
(education, household income, household wealth, and might have occurred during the follow-up period. Even if
income level of the country, with subdivision by rural and major dietary changes occurred after the baseline
urban location) did not alter our results. Despite this, it is assessment, they probably would have weakened the
possible that high consumption of carbohydrate and low observed associations. Third, there is potential for social
consumption of animal products might simply reflect desirability bias and individuals who are health conscious
lower incomes; residual confounding as a potential might also adopt other healthy lifestyles. However, if this
reason for our results cannot be completely excluded. were the case, we would not expect to see different
In our replacement analyses, the strongest association associations for the different outcomes. Fourth, as with
on total mortality was observed when carbohydrate was any observational cohort study, observed associations
replaced with polyunsaturated fatty acids, which is might be in part due to residual confounding (eg,
consistent with the pooled analyses of the Health differences in the ability to afford fats and animal proteins,
Professionals Follow up and the Nurses’ Health Study.46 which are more expensive than carbohydrates) despite
We found a lower risk of stroke when carbohydrate was extensive adjustment for known confounding factors.
replaced with saturated fatty acids, which is consistent Furthermore, while high-carbohydrate and low-fat diets
with previous work showing that refined carbohydrate might be a proxy for poverty or access to health care, all of
intake is associated with increased risk of stroke.7,47 our models adjusted for education and study centre (which
Mente and colleagues45 relate the intake of total fat, tracks with country income and urban or rural location)
types of fat, and carbohydrate to blood lipids and observed and would be expected to account for differences in
patterns of associations that were consistent with socioeconomic factors across intake categories. Additional
previous studies (eg, higher intakes of saturated fatty analyses adjusting for other measures of socioeconomic
acids are associated with higher LDL cholesterol, but also status (household wealth or income) did not alter the
with higher HDL cholesterol, lower triglycerides, lower results. Despite this, it is possible that high consumption
total cholesterol-to-HDL cholesterol ratio, and lower of carbohydrate and low consumption of animal products
ApoB-to-ApoA1 ratio). By contrast, increased carbohydrate might reflect lower incomes and residual confounding of
intake is associated with lower LDL cholesterol but also our results cannot be completely excluded. We were unable
with lower HDL cholesterol and higher triglycerides, to quantify separately the types of carbohydrate (refined vs
total cholesterol-to-HDL cholesterol ratio, and ApoB-to- whole grains) consumed. However, carbohydrate
ApoA1 ratio. The latter is particularly noteworthy as consumption in low-income and middle-income countries
ApoB-to-ApoA1 ratio is the strongest lipid predictor of is mainly from refined sources. Fifth, we were unable to
myocardial infarction and ischaemic strokes; this might measure trans-fat intake which might affect our results,
provide a mechanistic explanation for the higher risk of especially our replacement analyses. Lastly, our FFQ
events seen with high carbohydrate intake and the assessed polyunsaturated fatty acid intake mainly from
generally lower risk of cardiovascular disease with greater foods, rather than from vegetable oils, which might have
saturated fatty acid intake. The lipid findings not only different health effects than those observed in our study.
confirm the validity of the FFQs that we used in the In conclusion, we found that a high carbohydrate
PURE study, but also show that nutrients have varying intake was associated with an adverse impact on total
effects on different lipid fractions. This suggests that mortality, whereas fats including saturated and
predicting the net clinical effect based on considering unsaturated fatty acids were associated with lower risk of
only the effects of nutrient intake on LDL cholesterol is total mortality and stroke. We did not observe any
not reliable in projecting the effects of diet on detrimental effect of fat intakes on cardiovascular disease
cardiovascular disease events or on total mortality. events. Global dietary guidelines should be reconsidered
Our study is the first to our knowledge that used country- in light of the consistency of findings from the present
specific FFQs and nutrient databases in a large number of study, with the conclusions from meta-analyses of other
individuals from countries in diverse regions with varying observational studies8,10,54 and the results of recent
food habits. The standardised dietary method enabled a randomised controlled trials.36
www.thelancet.com Published online August 29, 2017 http://dx.doi.org/10.1016/S0140-6736(17)32252-3 11
Articles
Contributors 4 Puska P. Fat and heart disease: yes we can make a change—the case
MD coordinated the entire nutrition component of PURE, wrote the of North Karelia (Finland). Ann Nutr Metab 2009; 54 (suppl 1): 33–38.
analysis plans, and had the primary responsibility for writing the paper. 5 O’Donnell MJ, Chin SL, Rangarajan S, et al. Global and regional
SY designed and supervised the PURE study, interpreted the data, and effects of potentially modifiable risk factors associated with acute
reviewed and commented on all drafts. AM reviewed and commented on stroke in 32 countries (INTERSTROKE): a case-control study. Lancet
the data analysis and drafts. XZ did the analysis and reviewed and 2016; 388: 761–75.
commented on drafts. SSA reviewed and commented on the data analysis 6 Yusuf S, Hawken S, Ounpuu S, et al. Effect of potentially modifiable
and drafts. SIB reviewed and commented on the data analysis. risk factors associated with myocardial infarction in 52 countries (the
SR coordinated the worldwide study and reviewed and commented on INTERHEART study): case-control study. Lancet 2004; 364: 937–52.
drafts. All other authors coordinated the study in their respective 7 Siri-Tarino PW, Chiu S, Bergeron N, Krauss RM. Saturated fats
countries and provided comments on drafts of the manuscript. versus polyunsaturated fats versus carbohydrate for cardiovascular
disease prevention and treatment. Annu Rev Nutr 2015; 35: 517–43.
Declaration of interests
8 de Souza RJ, Mente A, Maroleanu A, et al. Intake of saturated and
We declare no competing interests. trans unsaturated fatty acids and risk of all cause mortality,
Acknowledgments cardiovascular disease, and type 2 diabetes: systematic review and
We are grateful to Russell de Souza who provided valuable feedback meta-analysis of observational studies. BMJ 2015; 351: h3978.
throughout the preparation of the manuscript. Our sincere thanks also go 9 Hooper L, Martin N, Abdelhamid A, Davey SG. Reduction in
to Dipika Desai who critically reviewed the nutrient database data. SY is saturated fat intake for cardiovascular disease.
Cochrane Database Syst Rev 2015; 6: CD011737.
supported by the Heart and Stroke Foundation/Marion W Burke Chair in
Cardiovascular Disease. The PURE Study is an investigator-initiated study 10 Siri-Tarino PW, Sun Q, Hu FB, Krauss RM. Meta-analysis of
prospective cohort studies evaluating the association of saturated fat
that is funded by the Population Health Research Institute, the Canadian
with cardiovascular disease. Am J Clin Nutr 2010; 91: 535–46.
Institutes of Health Research (CIHR), Heart and Stroke Foundation of
11 Grasgruber P, Sebera M, Hrazdira E, Hrebickova S, Cacek J.
Ontario, support from CIHR’s Strategy for Patient Oriented Research,
Food consumption and the actual statistics of cardiovascular diseases:
through the Ontario SPOR Support Unit, as well as the Ontario Ministry
an epidemiological comparison of 42 European countries.
of Health and Long-Term Care and through unrestricted grants from Food Nutr Res 2016; 60: 31694.
several pharmaceutical companies (with major contributions from 12 Praagman J, Beulens JW, Alssema M, et al. The association between
AstraZeneca [Canada], Sanofi-Aventis [France and Canada], Boehringer dietary saturated fatty acids and ischemic heart disease depends on
Ingelheim [Germany and Canada], Servier, and GlaxoSmithKline), and the type and source of fatty acid in the European Prospective
additional contributions from Novartis and King Pharma and from various Investigation into Cancer and Nutrition—Netherlands cohort.
national or local organisations in participating countries. These include: Am J Clin Nutr 2016; 103: 356–65.
Argentina: Fundacion ECLA; Bangladesh: Independent University, 13 Praagman J, de Jonge EA, Kiefte-de Jong JC, et al. Dietary saturated
Bangladesh and Mitra and Associates; Brazil: Unilever Health Institute, fatty acids and coronary heart disease risk in a Dutch middle-aged
Brazil; Canada: Public Health Agency of Canada and Champlain and elderly population. Arterioscler Thromb Vasc Biol 2016;
Cardiovascular Disease Prevention Network; Chile: Universidad de la 36: 2011–18.
Frontera; China: National Center for Cardiovascular Diseases; Colombia: 14 Mente A, O’Donnell MJ, Rangarajan S, et al. Association of urinary
Colciencias (grant number 6566-04-18062); India: Indian Council of sodium and potassium excretion with blood pressure. N Engl J Med
Medical Research; Malaysia: Ministry of Science, Technology and 2014; 371: 601–11.
Innovation of Malaysia (grant numbers 100-IRDC/BIOTEK 15 O’Donnell M, Mente A, Yusuf S. Sodium and cardiovascular disease.
16/6/21[13/2007] and 07-05-IFN-BPH 010), Ministry of Higher Education of N Engl J Med 2014; 371: 2137–38.
Malaysia (grant number 600-RMI/LRGS/5/3[2/2011]), Universiti Teknologi 16 Yusuf S, Islam S, Chow CK, et al. Use of secondary prevention drugs
MARA, Universiti Kebangsaan Malaysia (UKM-Hejim-Komuniti-15-2010); for cardiovascular disease in the community in high-income,
occupied Palestinian territory: the UN Relief and Works Agency for middle-income, and low-income countries (the PURE Study):
a prospective epidemiological survey. Lancet 2011; 378: 1231–43.
Palestine Refugees in the Near East (UNRWA), International Development
Research Centre, Canada; Poland: Polish Ministry of Science and Higher 17 Miller V, Mente A, Dehghan M, et al. Fruit, vegetable, and legume
intake, and cardiovascular disease and deaths in 18 countries
Education (grant number 290/W-PURE/2008/0), Wroclaw Medical
(Prospective Urban Rural Epidemiology [PURE]): a prospective cohort
University; South Africa: The North-West University, SANPAD (SA and
study. Lancet 2017; published online Aug 29. http://dx.doi.org/10.1016/
Netherlands Programme for Alternative Development), National Research S0140-6736(17)32253-5.
Foundation, Medical Research Council of South Africa, The South Africa
18 Corsi DJ, Subramanian SV, Chow CK, et al. Prospective Urban Rural
Sugar Association, Faculty of Community and Health Sciences; Sweden: Epidemiology (PURE) study: baseline characteristics of the household
grants from the Swedish State under the Agreement concerning research sample and comparative analyses with national data in 17 countries.
and education of doctors, the Swedish Heart and Lung Foundation, the Am Heart J 2013; 166: 636–46.
Swedish Research Council, the Swedish Council for Health, Working Life 19 Craig CL, Marshall AL, Sjostrom M, et al. International physical
and Welfare, King Gustaf V’s and Queen Victoria Freemasons Foundation, activity questionnaire: 12-country reliability and validity.
AFA Insurance, Swedish Council for Working Life and Social Research, Med Sci Sports Exerc 2003; 35: 1381–95.
Swedish Research Council for Environment, Agricultural Sciences and 20 Bharathi AV, Kurpad AV, Thomas T, Yusuf S, Saraswathi G, Vaz M.
Spatial Planning, grant from the Swedish State under Development of food frequency questionnaires and a nutrient
(LäkarUtbildningsAvtalet) Agreement, grant from the Västra Götaland database for the Prospective Urban and Rural Epidemiological
Region; Turkey: Metabolic Syndrome Society, AstraZeneca, Turkey, (PURE) pilot study in South India: methodological issues.
Sanofi Aventis, Turkey; United Arab Emirates: Asia Pac J Clin Nutr 2008; 17: 178–85.
Sheikh Hamdan Bin Rashid Al Maktoum Award for Medical Sciences, 21 Dehghan M, Al HN, Yusufali A, Nusrath F, Yusuf S, Merchant AT.
Dubai Health Authority, Dubai. Development of a semi-quantitative food frequency questionnaire for
use in United Arab Emirates and Kuwait based on local foods. Nutr J
References 2005; 4: 18.
1 Yusuf S, Rangarajan S, Teo K, et al. Cardiovascular risk and events 22 Dehghan M, Al-Hamad N, McMillan CR, Prakash P, Merchant AT.
in 17 low-, middle-, and high-income countries. N Engl J Med 2014; Comparison of a semi-quantitative food frequency questionnaire with
371: 818–27. 24-hour dietary recalls to assess dietary intake of adult Kuwaitis.
2 WHO. World Health Organization healthy diet fact sheet number Saudi Med J 2009; 30: 159–61.
394, 2017. www.who.int/mediacentre/factsheets/fs394/en/ (accessed 23 Dehghan M, Lopez JP, Duenas R, et al. Development and validation
Aug 19, 2017). of a quantitative food frequency questionnaire among rural- and
3 Keys A, Aravanis C, Blackburn H, et al. A multivariate analysis of urban-dwelling adults in Colombia. J Nutr Educ Behav 2012;
death and coronary heart disease. Cambridge, MA: Harvard 44: 609–13.
University Press, 1980.
12 www.thelancet.com Published online August 29, 2017 http://dx.doi.org/10.1016/S0140-6736(17)32252-3
Articles
24 Dehghan M, Ilow R, Zatonska K, et al. Development, reproducibility 40 Burger KN, Beulens JW, Boer JM, Spijkerman AM, van der AD.
and validity of the food frequency questionnaire in the Poland arm of Dietary glycemic load and glycemic index and risk of coronary
the Prospective Urban and Rural Epidemiological (PURE) study. heart disease and stroke in Dutch men and women:
J Hum Nutr Diet 2012; 25: 225–32. the EPIC-MORGEN study. PLoS One 2011; 6: e25955.
25 Dehghan M, del CS, Zhang X, et al. Validation of a semi-quantitative 41 Oh K, Hu FB, Cho E, et al. Carbohydrate intake, glycemic index,
food frequency questionnaire for Argentinean adults. PLoS One 2012; glycemic load, and dietary fiber in relation to risk of stroke in
7: e37958. women. Am J Epidemiol 2005; 161: 161–69.
26 Dehghan M, Martinez S, Zhang X, et al. Relative validity of an FFQ to 42 Fan J, Song Y, Wang Y, Hui R, Zhang W. Dietary glycemic index,
estimate daily food and nutrient intakes for Chilean adults. glycemic load, and risk of coronary heart disease, stroke, and stroke
Public Health Nutr 2013; 16: 1782–88. mortality: a systematic review with meta-analysis. PLoS One 2012;
27 Dehghan M, Mente A, Teo KK, et al. Relationship between healthy 7: e52182.
diet and risk of cardiovascular disease among patients on drug 43 Hoogeveen RC, Gaubatz JW, Sun W, et al. Small dense low-density
therapies for secondary prevention: a prospective cohort study of lipoprotein-cholesterol concentrations predict risk for coronary heart
31 546 high-risk individuals from 40 countries. Circulation 2012; disease: the Atherosclerosis Risk In Communities (ARIC) study.
126: 2705–12. Arterioscler Thromb Vasc Biol 2014; 34: 1069–77.
28 Gunes FE, Imeryuz N, Akalin A, et al. Development and validation 44 Parish S, Offer A, Clarke R, et al. Lipids and lipoproteins and risk of
of a semi-quantitative food frequency questionnaire to assess different vascular events in the MRC/BHF Heart Protection Study.
dietary intake in Turkish adults. J Pak Med Assoc 2015; 65: 756–63. Circulation 2012; 125: 2469–78.
29 Iqbal R, Ajayan K, Bharathi AV, et al. Refinement and validation of 45 Mente A, Dehghan M, Rangarajan S, et al. Association of
an FFQ developed to estimate macro- and micronutrient intakes in dietary nutrients with blood lipids and blood pressure in
a south Indian population. Public Health Nutr 2009; 12: 12–18. 18 countries: a cross-sectional analysis from the PURE study.
30 Mahajan R, Malik M, Bharathi AV, et al. Reproducibility and Lancet Diabetes Endocrinol 2017; published online Aug 29.
validity of a quantitative food frequency questionnaire in an urban http://dx.doi.org/10.1016/S2213-8587(17)30283-8.
and rural area of northern India. Natl Med J India 2013; 26: 266–72. 46 Wang DD, Li Y, Chiuve SE, et al. Association of specific dietary fats
31 Merchant AT, Dehghan M. Food composition database with total and cause-specific mortality. JAMA Intern Med 2016;
development for between country comparisons. Nutr J 2006; 5: 2. 176: 1134–45.
32 Mani I, Kurpad AV. Fats and fatty acids in Indian diets: time for 47 Yu E, Rimm E, Qi L, Rexrode K, et al. Diet, lifestyle, biomarkers,
serious introspection. Indian J Med Res 2016; 144: 507–14. genetic factors, and risk of cardiovascular disease in the Nurses’
Health Studies. Am J Public Health 2016; 106: 1616–23.
33 Yu D, Shu XO, Li H, et al. Dietary carbohydrate, refined grains,
glycemic load, and risk of coronary heart disease in Chinese adults. 48 Hu FB, Stampfer MJ, Manson JE, et al. Dietary fat intake and the risk
Am J Epidemiol 2013; 178: 1542–49. of coronary heart disease in women. N Engl J Med 1997; 337: 1491–99.
34 Hu FB, Stampfer MJ, Rimm E, et al. Dietary fat and coronary heart 49 Li Y, Hruby A, Bernstein AM, et al. Saturated fats compared with
disease: a comparison of approaches for adjusting for total energy unsaturated fats and sources of carbohydrate in relation to risk of
intake and modeling repeated dietary measurements. coronary heart disease: a prospective cohort study. J Am Coll Cardiol
Am J Epidemiol 1999; 149: 531–40. 2015; 66: 1538–48.
35 Hamley S. The effect of replacing saturated fat with mostly n-6 50 Yamagishi K, Iso H, Kokubo Y, et al. Dietary intake of saturated fatty
polyunsaturated fat on coronary heart disease: a meta-analysis of acids and incident stroke and coronary heart disease in Japanese
randomised controlled trials. Nutr J 2017; 16: 30. communities: the JPHC Study. Eur Heart J 2013; 34: 1225–32.
36 Ramsden CE, Zamora D, Majchrzak-Hong S, et al. Re-evaluation of 51 Guasch-Ferre M, Babio N, Martinez-Gonzalez MA, et al. Dietary fat
the traditional diet-heart hypothesis: analysis of recovered data intake and risk of cardiovascular disease and all-cause mortality in a
from Minnesota Coronary Experiment (1968–73). BMJ 2016; population at high risk of cardiovascular disease. Am J Clin Nutr 2015;
353: i1246. 102: 1563–73.
37 Schwingshackl L, Hoffmann G. Dietary fatty acids in the secondary 52 Nagata C, Nakamura K, Wada K, et al. Total fat intake is associated
prevention of coronary heart disease: a systematic review, with decreased mortality in Japanese men but not in women. J Nutr
meta-analysis and meta-regression. BMJ Open 2014; 4: e004487. 2012; 142: 1713–19.
38 Hu FB, Stampfer MJ, Manson JE, et al. Dietary saturated fats and 53 Mozaffarian D, Micha R, Wallace S. Effects on coronary heart disease
their food sources in relation to the risk of coronary heart disease of increasing polyunsaturated fat in place of saturated fat: a systematic
in women. Am J Clin Nutr 1999; 70: 1001–08. review and meta-analysis of randomized controlled trials. PLoS Med
2010; 7: e1000252.
39 Ascherio A, Rimm EB, Giovannucci EL, Spiegelman D,
Stampfer M, Willett WC. Dietary fat and risk of coronary heart 54 Jakobsen MU, O’Reilly EJ, Heitmann BL, et al. Major types of dietary
disease in men: cohort follow up study in the United States. BMJ fat and risk of coronary heart disease: a pooled analysis of 11 cohort
1996; 313: 84–90. studies. Am J Clin Nutr 2009; 89: 1425–32.
www.thelancet.com Published online August 29, 2017 http://dx.doi.org/10.1016/S0140-6736(17)32252-3 13
Comment
PURE study challenges the definition of a healthy diet:
but key questions remain
The relationships between diet, cardiovascular disease, question, the PURE team needs to complete a thorough Published Online
August 29, 2017
and death are topics of major public health importance, analysis relating intakes of different animal products http://dx.doi.org/10.1016/
and subjects of great controversy.1,2 In European and to mortality. S0140-6736(17)32241-9
North American countries, the most enduring and Micronutrient malnutrition is an important problem in See Online/Articles
http://dx.doi.org/10.1016/
consistent diet advice is to restrict saturated fatty acids, many of the countries included in PURE. Animal products S0140-6736(17)32252-3 and
by replacing animal fats with vegetable oils and complex are rich sources of zinc, bioavailable iron, vitamin K2, and http://dx.doi.org/10.1016/
S0140-6736(17)32253-5
carbohydrates (and more recently whole grains).1,3 In vitamin B12, which might be suboptimal in populations
The Lancet, Mahshid Dehghan and colleagues4 echo consuming high carbohydrate diets. Therefore, one
the views of a growing number of scientists by stating potential explanation for the PURE results is that
that advice to restrict saturated fatty acids “is largely nutrient-dense meats corrected one or more nutrient
based on selective emphasis on some observational and deficiencies. Since the PURE study collected blood for
clinical data, despite the existence of several randomised lipoprotein analyses,5 this potential role of micronutrient
trials and observational studies that do not support deficiency in PURE could be investigated further.
these conclusions”. This lack of definitive evidence has Which carbohydrates are associated with increased
left clinicians, scientists, and the public uncertain about mortality? Dehghan and colleagues4 report that high
the best foods to advise and to eat.2 intake of total carbohydrates was associated with
Dehghan and colleagues4 add to this uncertainty increased mortality. In a concurrent Lancet Article,6
by publishing the initial results of the Prospective the PURE group reports that intakes of fruits, legumes,
Urban Rural Epidemiology (PURE) study, an ambitious and raw vegetables (three major carbohydrate sources)
undertaking involving over 200 investigators who were associated with lower mortality. This discrepancy
collected data on more than 135 000 individuals from suggests that processed carbohydrates, including
18 countries across five continents for an average of added sugars and refined grains, are likely driving this
7·4 years. As the largest prospective observational study association. In a future paper, the PURE group should
to assess the association of nutrients (estimated by food report associations between added sugars, refined
frequency questionnaires) with cardiovascular disease grains, whole grains, and mortality.
and mortality in low-income and middle-income Is PURE less confounded by conscientiousness than
populations, the PURE findings make an important observational studies done in European and North
contribution to the field. The PURE team report that
higher intakes of fats (including saturated fatty acids,
monounsaturated fatty acids, and total polyunsaturated
fatty acids) and animal protein were each associated
with lower mortality, whereas carbohydrate intake
was associated with increased mortality.4 Here we
provide context and highlight questions that need to be
answered to move the field forward.
Do meats and dairy reduce mortality? Animal products
(including beef, lamb, and dairy) are the major sources of
UniversalImagesGroup/Contributor/Getty
saturated fatty acids and monounsaturated fatty acids
in most populations studied in PURE. Since saturated
fatty acids, monounsaturated fatty acids, and animal
protein were all inversely associated with mortality,
is the real finding simply that meat and dairy intakes
were associated with increased survival? To answer this
www.thelancet.com Published online August 29, 2017 http://dx.doi.org/10.1016/S0140-6736(17)32241-9 1
Comment
American countries? Conscientiousness is among the *Christopher E Ramsden, Anthony F Domenichiello
best predictors of longevity.7 For example, in a Japanese Laboratory of Clinical Investigation, National Institute on Aging,
National Institutes of Health, Baltimore, MD, USA (CER, AFD); and
population, highly and moderately conscientious
Intramural Program of the National Institute on Alcohol Abuse and
individuals had 54% and 50% lower mortality, Alcoholism, National Institutes of Health, Bethesda, MD, USA (CER)
respectively, compared with the least conscientious chris.ramsden@nih.gov
tertile.8 Conscientious individuals exhibit numerous We declare no competing interests.
health-related behaviours ranging from adherence 1 Sacks FM, Lichtenstein AH, Wu JHY, et al. Dietary fats and cardiovascular
disease: a presidential advisory from the American Heart Association.
to physicians’ recommendations and medication Circulation 2017; 136: e1–23.
regimens,9 to better sleep habits,10 to less alcohol 2 Nissen SE. US dietary guidelines: an evidence-free zone. Ann Intern Med 2016;
164: 558–59.
and substance misuse.11 Importantly, conscientious 3 US Department of Health and Human Services, US Department of
individuals tend to eat more recommended foods and Agriculture. 2015–2020 Dietary guidelines for Americans, 8th edn.
December, 2015. http://health.gov/dietaryguidelines/2015/guidelines/
fewer restricted foods.12 Since individuals in European (accessed Aug 9, 2017).
and North American populations have, for many 4 Dehghan M, Mente A, Zhang X, et al, on behalf of the Prospective Urban Rural
Epidemiology (PURE) study investigators. Associations of fats and
decades, received influential diet recommendations, carbohydrate intake with cardiovascular disease and mortality in 18 countries
from five continents (PURE): a prospective cohort study. Lancet 2017;
protective associations attributed to nutrients in published online Aug 29. http://dx.doi.org/10.1016/S0140-6736(17)32252-3.
studies of these populations are likely confounded by 5 Mente A, Dehghan M, Rangarajan S, et al. Association of dietary nutrients
with blood lipids and blood pressure in 18 countries: a cross-sectional
numerous other healthy behaviours. Because many analysis from the PURE study. Lancet Diabetes Endocrinol 2017; published
of the populations included in PURE are less exposed online Aug 29. http://dx.doi.org/10.1016/S0140-6736(17)32252-3.
6 Miller V, Mente A, Dehghan M, et al. Fruit, vegetable, and legume intake, and
to influential diet recommendations, the present cardiovascular disease and deaths in 18 countries (Prospective Urban Rural
Epidemiology [PURE]): a prospective cohort study. Lancet 2017; published
findings are perhaps less likely to be confounded by online Aug 29. http://dx.doi.org/10.1016/S0140-6736(17)32253-5.
conscientiousness. 7 Terracciano A, Lockenhoff CE, Zonderman AB, Ferrucci L, Costa PT Jr.
Personality predictors of longevity: activity, emotional stability,
The PURE study is an impressive undertaking that will and conscientiousness. Psychosom Med 2008; 70: 621–27.
contribute to public health for years to come. Initial PURE 8 Iwasa H, Masui Y, Gondo Y, Inagaki H, Kawaai C, Suzuki T. Personality and
all-cause mortality among older adults dwelling in a Japanese community:
findings challenge conventional diet–disease tenets a five-year population-based prospective cohort study.
Am J Geriatr Psychiatry 2008; 16: 399–405.
that are largely based on observational associations in
9 Hill PL, Roberts BW. The role of adherence in the relationship between
European and North American populations, adding to conscientiousness and perceived health. Health Psychol 2011; 30: 797–804.
the uncertainty about what constitutes a healthy diet. 10 Duggan KA, Friedman HS, McDevitt EA, Mednick SC. Personality and
healthy sleep: the importance of conscientiousness and neuroticism.
This uncertainty is likely to prevail until well designed PLoS One 2014; 9: e90628.
11 Terracciano A, Löckenhoff CE, Crum RM, Bienvenu OJ, Costa PT Jr. Five-factor
randomised controlled trials are done. Until then, the model personality profiles of drug users. BMC Psychiatry 2008; 11: 22.
best medicine for the nutrition field is a healthy dose 12 Keller C, Siegrist M. Does personality influence eating styles and food
choices? Direct and indirect effects. Appetite 2015; 84: 128–38.
of humility.
2 www.thelancet.com Published online August 29, 2017 http://dx.doi.org/10.1016/S0140-6736(17)32241-9
View publication stats
You might also like
- Diagnosis and Management of Hepatic Encephalopathy: A Case-based GuideFrom EverandDiagnosis and Management of Hepatic Encephalopathy: A Case-based GuideJasmohan S. BajajNo ratings yet
- Study PUREDocument13 pagesStudy PURESara MoreiraNo ratings yet
- Complementary and Alternative Medical Lab Testing Part 3: CardiologyFrom EverandComplementary and Alternative Medical Lab Testing Part 3: CardiologyRating: 1 out of 5 stars1/5 (1)
- Pi Is 0140673617322523Document13 pagesPi Is 0140673617322523Jefferson MorenoNo ratings yet
- Vegetarian Diet, Seventh Day Adventists and Risk of CardiovascularDocument7 pagesVegetarian Diet, Seventh Day Adventists and Risk of CardiovascularJohn SammutNo ratings yet
- Smyth Et Al., 2015 (KEEMPAT)Document10 pagesSmyth Et Al., 2015 (KEEMPAT)shofiNo ratings yet
- Modifible Risk FactorDocument14 pagesModifible Risk FactorCristofher SitanggangNo ratings yet
- Articulo ECVDocument13 pagesArticulo ECVMiguel OchoaNo ratings yet
- Nihms866890 UPLOAD 3Document21 pagesNihms866890 UPLOAD 3Peter GardinerNo ratings yet
- Actividad FísicaDocument12 pagesActividad FísicaDaniel Felipe OrtizNo ratings yet
- Fasting Lipid Profile in Acute Ischemic Stroke Patients Who Are Already On Lipid-Lowering DrugsDocument7 pagesFasting Lipid Profile in Acute Ischemic Stroke Patients Who Are Already On Lipid-Lowering DrugsPir Mudassar Ali ShahNo ratings yet
- Meta-Analysis in Research On Nutrition: To The EditorDocument2 pagesMeta-Analysis in Research On Nutrition: To The EditorLUISNo ratings yet
- Association of Dietary Fatty Acids With Coronary RiskDocument17 pagesAssociation of Dietary Fatty Acids With Coronary Riskubiktrash1492No ratings yet
- Cardiovascular and Metabolic Effects of Metformin in Patients With Type 1 Diabetes (REMOVAL) - A Double-Blind, Randomised, Placebo-Controlled TrialDocument13 pagesCardiovascular and Metabolic Effects of Metformin in Patients With Type 1 Diabetes (REMOVAL) - A Double-Blind, Randomised, Placebo-Controlled TrialRoberto López Mata100% (1)
- BMJ m513 FullDocument13 pagesBMJ m513 FullEduard Antonio Maury SintjagoNo ratings yet
- REWIND TrialDocument10 pagesREWIND Trialhenry hernandezNo ratings yet
- Maturitas: SciencedirectDocument6 pagesMaturitas: SciencedirectDaniel QuirogaNo ratings yet
- Ioi70171 2461 2468Document8 pagesIoi70171 2461 2468jimmyneutron1337No ratings yet
- Egg Consumption BMJDocument14 pagesEgg Consumption BMJLasiaf AlaskaNo ratings yet
- Fish Consumption & Risk of Cardiovascular Disease and Mortality From 58 CountriesDocument19 pagesFish Consumption & Risk of Cardiovascular Disease and Mortality From 58 CountriesSY LodhiNo ratings yet
- Cardiorespiratory Fitness As A Quantitative Predictor of All-Cause Mortality and Cardiovascular Events in Healthy Men and WomenDocument12 pagesCardiorespiratory Fitness As A Quantitative Predictor of All-Cause Mortality and Cardiovascular Events in Healthy Men and WomenNoah GabrielNo ratings yet
- Art Beneficios Del Huevo PDFDocument13 pagesArt Beneficios Del Huevo PDFAldaveLuisNo ratings yet
- Genetic Risk, Adherence To A Healthy Lifestyle, and Coronary DiseaseDocument10 pagesGenetic Risk, Adherence To A Healthy Lifestyle, and Coronary DiseaseNurul Falah KalokoNo ratings yet
- 6.vol5 Issue2 2017 MS 15392Document4 pages6.vol5 Issue2 2017 MS 15392iamsleepless007No ratings yet
- Work Stress and Risk of Death in Men and Women With and Without Cardiometabolic Disease: A Multicohort StudyDocument9 pagesWork Stress and Risk of Death in Men and Women With and Without Cardiometabolic Disease: A Multicohort StudyRaúl AñariNo ratings yet
- Zhuang2019 PDFDocument26 pagesZhuang2019 PDFkamila rodriguezNo ratings yet
- Role of Dyslipidemia in Stroke and Comparison of Lipid Profile in Ischemic and Hemorrhagic Stroke - A Case Control StudyDocument5 pagesRole of Dyslipidemia in Stroke and Comparison of Lipid Profile in Ischemic and Hemorrhagic Stroke - A Case Control StudyValentina TjandraNo ratings yet
- RefaratDocument8 pagesRefaratGrace SesaNo ratings yet
- No Se Encuentra Asociación Entre El Huevo y Enfermedad Cardiovascular o Alteración de Lípidos o Mayor MortalidadDocument9 pagesNo Se Encuentra Asociación Entre El Huevo y Enfermedad Cardiovascular o Alteración de Lípidos o Mayor MortalidadFranco TormoNo ratings yet
- Urinary Sodium Excretion, Blood Pressure, Cardiovascular Disease, and Mortality: A Community-Level Prospective Epidemiological Cohort StudyDocument11 pagesUrinary Sodium Excretion, Blood Pressure, Cardiovascular Disease, and Mortality: A Community-Level Prospective Epidemiological Cohort StudyRobertoNo ratings yet
- 2020 Vegan Diet CVDDocument12 pages2020 Vegan Diet CVDMariNo ratings yet
- Vegetarian Dietary Patterns and Mortality in Adventist Health Study 2Document9 pagesVegetarian Dietary Patterns and Mortality in Adventist Health Study 2Diana PrietoNo ratings yet
- nejmoa tremendo!!!Document14 pagesnejmoa tremendo!!!miguelalmenarezNo ratings yet
- Nihms 1020972Document11 pagesNihms 1020972Carlos Alfredo Pedroza MosqueraNo ratings yet
- The Triglyceride Paradox in Stroke Survivors: A Prospective StudyDocument8 pagesThe Triglyceride Paradox in Stroke Survivors: A Prospective StudyRay HannaNo ratings yet
- Hope 4 Lancet 2019Document12 pagesHope 4 Lancet 2019Marco Cordova RosellNo ratings yet
- Articles: BackgroundDocument9 pagesArticles: BackgroundRirin OktavianiNo ratings yet
- Journal Homepage: - : IntroductionDocument5 pagesJournal Homepage: - : IntroductionIJAR JOURNALNo ratings yet
- Am J Clin Nutr 2010 Chiuve Ajcn.110.002253Document8 pagesAm J Clin Nutr 2010 Chiuve Ajcn.110.002253Sex & Gender Women's Health CollaborativeNo ratings yet
- PIIS2214109X18302420Document10 pagesPIIS2214109X18302420Made ChinaNo ratings yet
- Environment InternationalDocument8 pagesEnvironment InternationalBella Kusuma DewiNo ratings yet
- Ioi110027 555 563Document9 pagesIoi110027 555 563Nika AbashidzeNo ratings yet
- Jamainternal Del Pozo Cruz 2022 Oi 220055 1667324433.60094Document10 pagesJamainternal Del Pozo Cruz 2022 Oi 220055 1667324433.60094nikolaiNo ratings yet
- Blood Pressure Lowering and Risk of New Type 2 DiabetesDocument8 pagesBlood Pressure Lowering and Risk of New Type 2 DiabetesFanny Isabel Rubio CampaNo ratings yet
- Metanalise Desfechos CVDocument9 pagesMetanalise Desfechos CVChristian OliveiraNo ratings yet
- E298 FullDocument16 pagesE298 FullThia SanjayaNo ratings yet
- PureDocument2 pagesPureHumberto Tapia EscalanteNo ratings yet
- Jamacardiology Aung 2018 Oi 170076Document10 pagesJamacardiology Aung 2018 Oi 170076jimmyneutron1337No ratings yet
- Egg Consumption in Relation To Cardiovascular Disease and Mortality: The Physicians' Health StudyDocument6 pagesEgg Consumption in Relation To Cardiovascular Disease and Mortality: The Physicians' Health Studykrazyj123No ratings yet
- Serum C Reactive Protein in The Prediction of Cardiovascular Diseases: Overview of The Latest Clinical Studies and Public Health PracticeDocument18 pagesSerum C Reactive Protein in The Prediction of Cardiovascular Diseases: Overview of The Latest Clinical Studies and Public Health PracticeVirginia ZagorniiNo ratings yet
- NIH Public Access: Type 2 Diabetes Mellitus and Hypertension: An UpdateDocument21 pagesNIH Public Access: Type 2 Diabetes Mellitus and Hypertension: An Updateyongky amaloNo ratings yet
- NIH Public Access: Author ManuscriptDocument10 pagesNIH Public Access: Author ManuscriptPaul AndreasNo ratings yet
- Dietary in Ammatory Potential and Risk of Cardiovascular Disease Among Men and Women in The U.SDocument13 pagesDietary in Ammatory Potential and Risk of Cardiovascular Disease Among Men and Women in The U.SRoxana CristeaNo ratings yet
- Metabolic Syndrome and Risk of Mortality in Middle-Aged Versus Elderly Individuals: The Nord-Trøndelag Health Study (HUNT)Document8 pagesMetabolic Syndrome and Risk of Mortality in Middle-Aged Versus Elderly Individuals: The Nord-Trøndelag Health Study (HUNT)Eriekafebriayana RNo ratings yet
- Faktor Risiko Pasien Stroke Yang Dirawat Di Ruang Neuro Rsu Bangil Kabupaten PasuruanDocument17 pagesFaktor Risiko Pasien Stroke Yang Dirawat Di Ruang Neuro Rsu Bangil Kabupaten PasuruanNona Suci rahayuNo ratings yet
- 215 FullDocument7 pages215 FullCésar Gonzalvo DíazNo ratings yet
- Sex Differences in High-Intensity StatinUse Following Myocardial InfarctionDocument9 pagesSex Differences in High-Intensity StatinUse Following Myocardial InfarctionjoNo ratings yet
- Meta Statin Induce DMDocument8 pagesMeta Statin Induce DMErvan ZuhriNo ratings yet
- Cancer TreatmentsDocument15 pagesCancer TreatmentsPatrisha KerrNo ratings yet
- Adherence To Cardiovascular Therapy: A Meta-Analysis of Prevalence and Clinical ConsequencesDocument9 pagesAdherence To Cardiovascular Therapy: A Meta-Analysis of Prevalence and Clinical Consequencesdaniela NeculmanNo ratings yet
- General Topics: Anesthesia, Analgesia, and Sedation of Small MammalsDocument23 pagesGeneral Topics: Anesthesia, Analgesia, and Sedation of Small Mammalsdoja catNo ratings yet
- Beck Youth InventoryDocument2 pagesBeck Youth InventoryHina Abbas Khan37% (30)
- Continual Improvement ProcedureDocument6 pagesContinual Improvement ProcedureRonald Sarillana100% (1)
- Research Paper On Noise PollutionDocument8 pagesResearch Paper On Noise Pollutionhmpquasif100% (1)
- Experiment 1 - Differential Count ImportanceDocument5 pagesExperiment 1 - Differential Count ImportanceIra ReyNo ratings yet
- DNHS SHS Exam in PE and Health 11 (Midterm Exam SY 2017-2018) Answer SheetDocument2 pagesDNHS SHS Exam in PE and Health 11 (Midterm Exam SY 2017-2018) Answer SheetArangote Glenn92% (91)
- DR Joe S Freedom From AngerDocument128 pagesDR Joe S Freedom From AngerTouhidul IslamNo ratings yet
- SMETA 6.1 Measurement Criteria PDFDocument96 pagesSMETA 6.1 Measurement Criteria PDFTuấn Mai vănNo ratings yet
- Adime 2Document13 pagesAdime 2api-496164982No ratings yet
- 4TH Year Stuide Guide Community MedicineDocument30 pages4TH Year Stuide Guide Community MedicineMohammad Jibran KhanNo ratings yet
- Annotated BibliographyDocument20 pagesAnnotated BibliographyautumnemilymaddyNo ratings yet
- Soap Note Example 3Document11 pagesSoap Note Example 3LorrieNo ratings yet
- Cancer and Its Easy Treatment in Homeopathy - Bashir Mahmud ElliasDocument5 pagesCancer and Its Easy Treatment in Homeopathy - Bashir Mahmud ElliasBashir Mahmud ElliasNo ratings yet
- Revised - Ie18 Final UpdatedDocument120 pagesRevised - Ie18 Final UpdatedLUCAS AndrewsNo ratings yet
- Requirements Checklist for Infrastructure Project PlansDocument6 pagesRequirements Checklist for Infrastructure Project PlansNheiljanmark Cayetano0% (1)
- Ecl SW Iso45001Document92 pagesEcl SW Iso45001Meghanath LalemmaNo ratings yet
- DM PhysecDocument237 pagesDM PhysecnormoNo ratings yet
- Healthy Eating Habits GuidelineDocument30 pagesHealthy Eating Habits GuidelineSuhanidah MyNo ratings yet
- Adaptive Community for Continuity of EducationDocument2 pagesAdaptive Community for Continuity of EducationAina Gail LontocNo ratings yet
- Week 4 English 9: Judging The Validity of The Evidence From A TextDocument4 pagesWeek 4 English 9: Judging The Validity of The Evidence From A TextMaria Carmela ArellanoNo ratings yet
- PSM PagewiseQuestions (Park 25th)Document12 pagesPSM PagewiseQuestions (Park 25th)JENNIFER JOHN MBBS2020No ratings yet
- Effectiveness of Mesotherapy On Body Contouring: BackgroundDocument7 pagesEffectiveness of Mesotherapy On Body Contouring: BackgroundNita Dewi NNo ratings yet
- Worksheet For Respiration Low AnswersDocument2 pagesWorksheet For Respiration Low AnswersIcs 2022No ratings yet
- Project ConceptDocument11 pagesProject Conceptokware brianNo ratings yet
- 3 Month Study Plan For CSS Exam PreparationDocument1 page3 Month Study Plan For CSS Exam PreparationDanish AliNo ratings yet
- Schemes of Government of Rajasthan in HealthDocument67 pagesSchemes of Government of Rajasthan in HealthKamal ShuklaNo ratings yet
- IDIP ER July 2012 - Unit IBDocument12 pagesIDIP ER July 2012 - Unit IBVusalNo ratings yet
- HMEF5063 Guidance and Counseling - Caug16 (Bookmark) PDFDocument188 pagesHMEF5063 Guidance and Counseling - Caug16 (Bookmark) PDFMarilyn Richard100% (1)
- Bahan Kuliah MHM Beginning BioethicsDocument80 pagesBahan Kuliah MHM Beginning BioethicsKlarasita WibowoNo ratings yet
- E.Coli Essay FINAL PDFDocument8 pagesE.Coli Essay FINAL PDFSaraturituriNo ratings yet
- Sugar Crush: How to Reduce Inflammation, Reverse Nerve Damage, and Reclaim Good HealthFrom EverandSugar Crush: How to Reduce Inflammation, Reverse Nerve Damage, and Reclaim Good HealthRating: 4 out of 5 stars4/5 (6)
- Summary of Mary Claire Haver's The Galveston DietFrom EverandSummary of Mary Claire Haver's The Galveston DietRating: 5 out of 5 stars5/5 (1)
- Forever Strong: A New, Science-Based Strategy for Aging WellFrom EverandForever Strong: A New, Science-Based Strategy for Aging WellNo ratings yet
- The Diabetes Code: Prevent and Reverse Type 2 Diabetes NaturallyFrom EverandThe Diabetes Code: Prevent and Reverse Type 2 Diabetes NaturallyRating: 5 out of 5 stars5/5 (1)
- The Arm: Inside the Billion-Dollar Mystery of the Most Valuable Commodity in SportsFrom EverandThe Arm: Inside the Billion-Dollar Mystery of the Most Valuable Commodity in SportsRating: 4 out of 5 stars4/5 (49)
- Keto Friendly Recipes: Easy Keto For Busy PeopleFrom EverandKeto Friendly Recipes: Easy Keto For Busy PeopleRating: 3.5 out of 5 stars3.5/5 (2)
- Summary: Fast Like a Girl: A Woman’s Guide to Using the Healing Power of Fasting to Burn Fat, Boost Energy, and Balance Hormones: Key Takeaways, Summary and AnalysisFrom EverandSummary: Fast Like a Girl: A Woman’s Guide to Using the Healing Power of Fasting to Burn Fat, Boost Energy, and Balance Hormones: Key Takeaways, Summary and AnalysisRating: 3 out of 5 stars3/5 (2)
- Body Love Every Day: Choose Your Life-Changing 21-Day Path to Food FreedomFrom EverandBody Love Every Day: Choose Your Life-Changing 21-Day Path to Food FreedomRating: 4 out of 5 stars4/5 (1)
- Secrets From the Eating Lab: The Science of Weight Loss, the Myth of Willpower, and Why You Should Never Diet AgainFrom EverandSecrets From the Eating Lab: The Science of Weight Loss, the Myth of Willpower, and Why You Should Never Diet AgainRating: 3.5 out of 5 stars3.5/5 (38)
- The Food Lover's Cleanse: 140 Delicious, Nourishing Recipes That Will Tempt You Back into Healthful EatingFrom EverandThe Food Lover's Cleanse: 140 Delicious, Nourishing Recipes That Will Tempt You Back into Healthful EatingRating: 4 out of 5 stars4/5 (3)
- Metabolism Revolution: Lose 14 Pounds in 14 Days and Keep It Off for LifeFrom EverandMetabolism Revolution: Lose 14 Pounds in 14 Days and Keep It Off for LifeNo ratings yet
- Happy Gut: The Cleansing Program to Help You Lose Weight, Gain Energy, and Eliminate PainFrom EverandHappy Gut: The Cleansing Program to Help You Lose Weight, Gain Energy, and Eliminate PainRating: 3.5 out of 5 stars3.5/5 (6)
- The Beck Diet Solution Weight Loss Workbook: The 6-Week Plan to Train Your Brain to Think Like a Thin PersonFrom EverandThe Beck Diet Solution Weight Loss Workbook: The 6-Week Plan to Train Your Brain to Think Like a Thin PersonRating: 3.5 out of 5 stars3.5/5 (33)
- Allen Carr's Easy Way for Women to Lose Weight: The original Easyway methodFrom EverandAllen Carr's Easy Way for Women to Lose Weight: The original Easyway methodRating: 4.5 out of 5 stars4.5/5 (18)
- How Not to Die by Michael Greger MD, Gene Stone - Book Summary: Discover the Foods Scientifically Proven to Prevent and Reverse DiseaseFrom EverandHow Not to Die by Michael Greger MD, Gene Stone - Book Summary: Discover the Foods Scientifically Proven to Prevent and Reverse DiseaseRating: 4.5 out of 5 stars4.5/5 (83)
- Eat to Lose, Eat to Win: Your Grab-n-Go Action Plan for a Slimmer, Healthier YouFrom EverandEat to Lose, Eat to Win: Your Grab-n-Go Action Plan for a Slimmer, Healthier YouNo ratings yet
- Instant Loss On a Budget: Super-Affordable Recipes for the Health-Conscious CookFrom EverandInstant Loss On a Budget: Super-Affordable Recipes for the Health-Conscious CookRating: 3.5 out of 5 stars3.5/5 (2)
- The Diet Trap Solution: Train Your Brain to Lose Weight and Keep It Off for GoodFrom EverandThe Diet Trap Solution: Train Your Brain to Lose Weight and Keep It Off for GoodNo ratings yet
- Find Your Path: Honor Your Body, Fuel Your Soul, and Get Strong with the Fit52 LifeFrom EverandFind Your Path: Honor Your Body, Fuel Your Soul, and Get Strong with the Fit52 LifeRating: 4 out of 5 stars4/5 (3)
- The Whole Body Reset: Your Weight-Loss Plan for a Flat Belly, Optimum Health & a Body You'll Love at Midlife and BeyondFrom EverandThe Whole Body Reset: Your Weight-Loss Plan for a Flat Belly, Optimum Health & a Body You'll Love at Midlife and BeyondRating: 4.5 out of 5 stars4.5/5 (28)
- The Body Book: The Law of Hunger, the Science of Strength, and Other Ways to Love Your Amazing BodyFrom EverandThe Body Book: The Law of Hunger, the Science of Strength, and Other Ways to Love Your Amazing BodyNo ratings yet
- Grit & Grace: Train the Mind, Train the Body, Own Your LifeFrom EverandGrit & Grace: Train the Mind, Train the Body, Own Your LifeRating: 4 out of 5 stars4/5 (3)
- Foods That Cause You to Lose Weight: The Negative Calorie EffectFrom EverandFoods That Cause You to Lose Weight: The Negative Calorie EffectRating: 3 out of 5 stars3/5 (5)
- The Fast800 Diet: Discover the Ideal Fasting Formula to Shed Pounds, Fight Disease, and Boost Your Overall HealthFrom EverandThe Fast800 Diet: Discover the Ideal Fasting Formula to Shed Pounds, Fight Disease, and Boost Your Overall HealthRating: 5 out of 5 stars5/5 (37)
- Glucose Revolution: The Life-Changing Power of Balancing Your Blood SugarFrom EverandGlucose Revolution: The Life-Changing Power of Balancing Your Blood SugarRating: 5 out of 5 stars5/5 (349)
- How to Be Well: The 6 Keys to a Happy and Healthy LifeFrom EverandHow to Be Well: The 6 Keys to a Happy and Healthy LifeRating: 5 out of 5 stars5/5 (1)
- The Candida Cure: The 90-Day Program to Balance Your Gut, Beat Candida, and Restore Vibrant HealthFrom EverandThe Candida Cure: The 90-Day Program to Balance Your Gut, Beat Candida, and Restore Vibrant HealthNo ratings yet
- Hungry for Change: Ditch the Diets, Conquer the Cravings, and Eat Your Way to Lifelong HealthFrom EverandHungry for Change: Ditch the Diets, Conquer the Cravings, and Eat Your Way to Lifelong HealthRating: 4 out of 5 stars4/5 (7)