Professional Documents
Culture Documents
Hope 4 Lancet 2019
Uploaded by
Marco Cordova RosellCopyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Hope 4 Lancet 2019
Uploaded by
Marco Cordova RosellCopyright:
Available Formats
Articles
A community-based comprehensive intervention to
reduce cardiovascular risk in hypertension (HOPE 4):
a cluster-randomised controlled trial
Jon-David Schwalm, Tara McCready, Patricio Lopez-Jaramillo, Khalid Yusoff, Amir Attaran, Pablo Lamelas, Paul A Camacho, Fadhlina Majid,
Shrikant I Bangdiwala, Lehana Thabane, Shofiqul Islam, Martin McKee, Salim Yusuf
Summary
Background Hypertension is the leading cause of cardiovascular disease globally. Despite proven benefits, hypertension Published Online
control is poor. We hypothesised that a comprehensive approach to lowering blood pressure and other risk factors, September 2, 2019
http://dx.doi.org/10.1016/
informed by detailed analysis of local barriers, would be superior to usual care in individuals with poorly controlled or
S0140-6736(19)31949-X
newly diagnosed hypertension. We tested whether a model of care involving non-physician health workers (NPHWs),
See Online/Comment
primary care physicians, family, and the provision of effective medications, could substantially reduce cardiovascular http://dx.doi.org/10.1016/
disease risk. S0140-6736(19)31995-6
Population Health Research
Methods HOPE 4 was an open, community-based, cluster-randomised controlled trial involving 1371 individuals with Institute, McMaster University
new or poorly controlled hypertension from 30 communities (defined as townships) in Colombia and Malaysia. and Hamilton Health Sciences,
Hamilton, ON, Canada
16 communities were randomly assigned to control (usual care, n=727), and 14 (n=644) to the intervention. After (J-D Schwalm MD,
community screening, the intervention included treatment of cardiovascular disease risk factors by NPHWs using T McCready PhD, P Lamelas MSc,
tablet computer-based simplified management algorithms and counselling programmes; free antihypertensive and Prof S I Bangdiwala PhD,
S Islam PhD, Prof S Yusuf DPhil);
statin medications recommended by NPHWs but supervised by physicians; and support from a family member or
Research Institute, Fundación
friend (treatment supporter) to improve adherence to medications and healthy behaviours. The primary outcome was Oftalmológica de Santander,
the change in Framingham Risk Score 10-year cardiovascular disease risk estimate at 12 months between intervention Floridablanca, Colombia
and control participants. The HOPE 4 trial is registered at ClinicalTrials.gov, NCT01826019. (Prof P Lopez-Jaramillo PhD,
P A Camacho MD); Masira
Institute, Medical School,
Findings All communities completed 12-month follow-up (data on 97% of living participants, n=1299). The reduction Universidad de Santander,
in Framingham Risk Score for 10-year cardiovascular disease risk was –6·40% (95% CI 8·00 to –4·80) in the control Bucaramanga, Colombia
group and –11·17% (–12·88 to –9·47) in the intervention group, with a difference of change of –4·78% (95% CI (Prof P Lopez-Jaramillo);
Faculty of Medicine, Universiti
–7·11 to –2·44, p<0·0001). There was an absolute 11·45 mm Hg (95% CI –14·94 to –7·97) greater reduction in
Teknologi MARA, Selayang,
systolic blood pressure, and a 0·41 mmol/L (95% CI –0·60 to –0·23) reduction in LDL with the intervention group Selangor, Malaysia
(both p<0·0001). Change in blood pressure control status (<140 mm Hg) was 69% in the intervention group versus (Prof K Yusoff MBBS,
30% in the control group (p<0·0001). There were no safety concerns with the intervention. F Majid BSc); Faculty of Medicine
and Health Sciences, UCSI,
Kuala Lumpur, Malaysia
Interpretation A comprehensive model of care led by NPHWs, involving primary care physicians and family that was (Prof K Yusoff); Faculty of Law
informed by local context, substantially improved blood pressure control and cardiovascular disease risk. This strategy (Prof A Attaran DPhil),
is effective, pragmatic, and has the potential to substantially reduce cardiovascular disease compared with current and Faculty of Medicine
(Prof A Attaran), University of
strategies that are typically physician based. Ottawa, Ottawa, ON, Canada;
Medical School, Universidad
Funding Canadian Institutes of Health Research; Grand Challenges Canada; Ontario SPOR Support Unit and the Autónoma de Bucaramanga,
Ontario Ministry of Health and Long-Term Care; Boehringer Ingelheim; Department of Management of Bucaramanga, Colombia
(P A Camacho); Department of
Non-Communicable Diseases, WHO; and Population Health Research Institute. Health Research Methods,
Evidence and Impact, McMaster
Copyright © 2019 Elsevier Ltd. All rights reserved. University Faculty of Health
Sciences, Hamilton, ON, Canada
(Prof S I Bangdiwala,
Introduction countries at all levels of development that many people Prof L Thabane PhD, Prof S Yusuf);
Cardiovascular disease is the most common cause of with hypertension are unaware of it, or are untreated and Department of Health
death globally, and hypertension the most common risk or uncontrolled.4 Consequently, fewer than 20% of Services Research and Policy,
factor for cardiovascular disease.1 In theory, there is no individuals with hypertension have their blood pressure London School of Hygiene &
Tropical Medicine, London, UK
reason why the goal of reducing cardiovascular disease controlled. Similarly, despite compelling evidence of the (Prof M McKee DSc)
mortality by 30% by 2030, agreed to by the governments benefits of statins in those with hypertension, uptake is Correspondence to:
of the world,2 should not be met. Effective, inexpensive extremely low in most parts of the world.5 Dr Jon-David Schwalm,
medicines to reduce risk factors have been available for This problem shares similarities with HIV a decade ago: Population Health Research
many years.3 The challenge we face is how to identify treatment was available, but people in need were often Institute, McMaster University
and Hamilton Health Sciences,
those who might benefit from treatment, and ensure that unable to benefit. The global health community responded Hamilton, ON, L8L 2X2 Canada
they are treated. We now have extensive information from by investing in health system strengthening, seeking to schwalj@mcmaster.ca
www.thelancet.com Published online September 2, 2019 http://dx.doi.org/10.1016/S0140-6736(19)31949-X 1
Articles
Research in context
Evidence before this study and Malaysia led to the development of an intervention
Hypertension is the leading cause of cardiovascular disease, with comprising of modification of health behaviours and initiation
the majority of the burden in low-income and middle-income of free combination antihypertensive drugs plus statins,
countries. The HOPE 4 programme was initiated in 2013, by non-physician health workers guided by a tablet
to address the burden of cardiovascular risk and hypertension. computer-based decision support system, supervised by
Initial phases of the programme included systematic reviews physicians, and involving an individual’s family or friends to
and mixed methods analysis to inform the design of the HOPE 4 promote adherence.
intervention components to be tested in a cluster randomised
Added value of this study
controlled trial. We systematically searched electronic databases
The HOPE 4 study shows that a comprehensive model of care
including MEDLINE, Embase, Global Health, LILACS, Africa-Wide
that is informed by strategies to overcome country-specific
Information, IMSEAR, IMEMR, and WPRIM from inception until
barriers, resulted in a substantial reduction in cardiovascular
May 8, 2013, to identify barriers to appropriate hypertension
disease risk and improved blood pressure control.
control at the patient, health-care provider, and health-system
level. No limits were applied with respect to language. Implications of all the available evidence
Controlled vocabulary, keywords (MeSH terms) and free-text Adoption of the HOPE 4 strategy could substantially enhance
terms were identified for each domain of our health systems reduction in cardiovascular disease risk in those with
framework which also focused on “hypertension’’, ‘‘barriers’’, hypertension, and in doing so help achieve the UN’s General
and ‘‘obstacles’’. No limits to study design were imposed. Assembly target that calls for a one-third reduction in
The barriers identified in the systematic review, coupled with premature cardiovascular disease mortality by 2030.
the findings of qualitative health-system appraisals in Colombia
create effective mechanisms to deliver treatment to those detailed health system assessment and barrier analysis in
who could benefit at low cost.6 So far, however, this each country,12,13 which used a combination of quantitative
approach has not been matched by those seeking to and qualitative research to identify the challenges that
reduce the preventable burden of cardiovascular disease. needed to be overcome in designing the intervention.
By drawing on the literature on health systems In this study, we tested the effectiveness of this compre
research, we can identify what such a response would hensive intervention in reducing cardiovascular disease
look like. First, it would address all of the building blocks risk among people with hypertension in two middle-
of health systems, and in particular the need for an income countries.
See Online for video appropriate workforce, access to affordable diagnostics A video abstract is available online.
and medicines, and evidence-based guidelines. Second,
it should be tailored to the national context, recognising Methods
that health systems are embedded within wider systems Study design and clusters
of governance, beliefs, and norms. The health outcomes The HOPE 4 study was a parallel-arm, cluster-random
prevention and evaluation 4 (HOPE 4) project is, to ised controlled trial done in 30 urban and rural
our knowledge, the first attempt to do this.7 Working in communities in Colombia (Fundación Oftalmológica de
two middle-income countries, Colombia and Malaysia, Santander) and Malaysia (Universiti Teknologi MARA).
we have developed, implemented, and evaluated, in a We have previously reported details for the study
cluster-randomised trial, a comprehensive model of care rationale, trial design, and methods.7 We have also
that takes full account of the local context. This innovative reported the results of the qualitative research that
package has been designed to address the constrained identified barriers and potential solutions to improving
resources affecting most countries based on systematic hypertension control, which were the basis for the
reviews of barriers to effective management of hyper development of the multifaceted intervention in the
tension.8,9 Thus, we used non-physician health workers HOPE 4 trial.8,9,12,13 After screening and enrolment in
(NPHWs) supported by physicians and, crucially, family each community was completed, community clusters
and community members; a simple combination of anti were randomly assigned to usual care or to participate
hypertensive drugs and a statin; and simplified guide in an active cardiovascular disease risk detection and
lines, delivered through a tablet computer (henceforth management programme facilitated by NPHWs for
called tablets). 12 months. The selection of study communities was
Many of these components have been separately informed by country-specific leads to ensure that they
evaluated in previous research, although with mixed were geographically separated. This separation was done
results.10,11 Our intervention is innovative in how, by taking to reduce contamination bias between clusters (ie,
a systems approach, it is more than the sum of its parts. participants from the control arm communities seeking
Importantly, our intervention is informed by an initial health care in the intervention arm communities). The
2 www.thelancet.com Published online September 2, 2019 http://dx.doi.org/10.1016/S0140-6736(19)31949-X
Articles
communities were rural and urban townships identified Procedures
by the local governments. The HOPE 4 study involved a multifaceted intervention
consisting of three core elements provided as a package:
Study population community screening, detection, treatment, and control
Screening to identify eligible participants in potential of cardiovascular disease risk factors by NPHWs (in
communities involved a combination of door-to-door collaboration with local physicians) guided by tablet-based
household screening and the use of community outreach simplified management algorithms, decision support,
centres or local events in public spaces. Eligible par and counselling programmes; provision of free locally
ticipants were aged at least 50 years, with at least one of available combination antihypertensive medications and
the following criteria: average systolic blood pressure a statin recommended by NPHWs, but supervised by local
(SBP) of at least 160 mm Hg recorded at one visit; average physicians; and support from a participant-nominated
SBP of 140–159 mm Hg recorded at one visit and treatment supporter (friend or family member) to improve
participant reported a diagnosis of hypertension or was adherence to medications and health behaviours.7–9,12,13,16
taking antihypertensive medication; average SBP of at The NPHWs did the initial screening, recruitment,
least 130 mm Hg recorded at one visit and participant and follow-up in both the intervention and control
reported a diagnosis of diabetes or was taking medications communities. No structured intervention was provided
for diabetes; did not meet earlier criteria, but had an in the control group, but they did receive existing
average SBP of 140–159 mm Hg recorded on two separate local cardiovascular disease health literature and were
visits, at least one day apart. recommended to see their local health-care provider as
Participants were ineligible if they refused consent, usual. The NPHWs in both the intervention and control
were concurrently participating in any other study or heart communities were a combination of newly hired and
health programme that would interfere with partici retrained community health workers and research staff.
pation in HOPE 4, had severe comorbid conditions with The NPHWs were paid for by the HOPE 4 study
life expectancy of less than 1 year, or had other serious with partial financial support from local governments.
conditions or factors likely to interfere with study The NPHWs were expected to have a minimum of a
participation or with their ability to complete the trial. secondary school diploma or equivalent. The 1-week
Before study initiation, the institutional review board or training curriculum, which was contextualised to each
independent ethics committee of participating institu country, has been previously published.17
tions approved the HOPE 4 protocol. Reporting in this Study medications included a generic single-pill
publication is consistent with the CONSORT statement.14 combination of two antihypertensives (at half or full
doses). Combinations included an angiotensin receptor
Randomisation and masking blocker or angiotensin converting enzyme inhibitor
A computer-generated, central randomisation system coupled with a diuretic or calcium channel blocker
(located at the Population Health Research Institute, (appendix p 2). A separate generic cholesterol-lowering See Online for appendix
Hamilton, ON, Canada), allocated communities (1:1) to agent (atorvastatin at 20 mg or rosuvastatin at 10 mg) was
either the intervention group or control group. Ran also provided (appendix p 2).7 These medications were
domisation was first stratified by country and then by also available in local pharmacies for about US$5–8 each
rural or urban location of the community. Each in Malaysia and $14–38 each in Colombia, per 1-month
community was randomly assigned after the entire supply. Both countries offer subsidies for medications
community was screened, and written consent was through the public health-care system. Following NPHW
obtained to avoid biases in the selection or volunteering recommendation, and medication prescription pro
of individuals within the intervention and control vided by the primary care physicians, medications were
communities. Participants, NPHWs, primary care physi dispensed either from pharmacies, by a professionally
cians, and local investigators were not masked to the trained pharmacist, or the physician’s office. NPHWs
study group allocation. Furthermore, lipids were analysed were responsible for delivering or arranging for
centrally within each country, without knowledge of participants to obtain the medications through home or
whether the samples were from participants in the local clinic visits, on the basis of participant preference
control or intervention communities. Blood pressure was and local context. Participants already taking cardio
measured as per the WHO STEPS protocol (ie, three vascular medication were reviewed by the NPHW and
separate readings, in which the last two were averaged) to supervising physician for transition (if appropriate) to
ensure consistency of recordings, and an automated the medications provided by the study. Study-associated
Omron monitor was used at each visit.15 These procedures medications were recommended, but not mandatory, as
avoid potential biases with respect to blood pressure part of the study protocol. These medications were
and lipid measurements. Variability was minimised by provided at no cost to the participant if they chose to
standardised NPHW curriculum training. Furthermore, use them. Participating NPHWs and physicians were
outcome assessments in the control and intervention provided with simplified medication management
groups were at similar timepoints. algorithms guiding their use by the study (appendix p 3).7
www.thelancet.com Published online September 2, 2019 http://dx.doi.org/10.1016/S0140-6736(19)31949-X 3
Articles
However, initiation or up-titration of antihypertensives
4904 individuals from 30 participating provided by the study was optional, and the ultimate
communities (clusters)* screened
for eligibility decisions about treatment in complex or uncertain cases
were left to the treating physician.
The NPHW visited participants in their home, or
3004 excluded
2938 did not meet study criteria
at a local clinic. At 6 months and 12 months after
66 undetermined† randomisation, the NPHW repeated study assessments
in all participants in both the intervention and control
communities and recorded the components of the
1900 eligible individuals identified
Framingham Risk Score (FRS).18 Fasting blood was
collected in participants at baseline and 12 months and
524 excluded analysed for total cholesterol, HDL, LDL, triglycerides,
509 refused consent
15 pre-randomisation deaths and glucose at a single core laboratory in each country
that was affiliated with the coordinating sites. Par
ticipants in communities randomly assigned to the
1376 participants enrolled intervention group had additional visits at baseline
(one with the NPHW and one with the local physician),
5 pre-randomisation deaths and at 1 month and 3 months after randomisation.
All participants were contacted (via telephone) at
10 months or 11 months after randomisation to confirm
1371 participants from 30 communities
randomly assigned availability for the 12-month visit. Data were collected
using study tablets, which had interactive data
validation measures.
727 participants from 16 communities 644 participants from 14 communities Outcomes
allocated to control* allocated to intervention*
The primary outcome was the mean difference in FRS
10-year cardiovascular disease risk estimate change
35 excluded because 12-month 37 excluded because 12-month from baseline to 12 months, between the intervention
data on risk factors not data on risk factors not and control groups.18 The FRS was chosen as the
available available
15 lost to follow-up 13 lost to follow-up and primary outcome because it is a validated risk score that
and refusals refusals considers several cardiovascular disease risk factors
15 post-randomisation 12 post-randomisation
deaths deaths
addressed by our intervention.19,20 Secondary outcomes
5 withdrawals 12 withdrawals included differences in the changes in SBP between
the intervention and control groups at 6 months and
12 months; differences in the changes in LDL, HDL,
692 participants with primary outcome 607 participants with primary outcome
at 12 months at 12 months total cholesterol, triglycerides, and glucose concen
trations at 12 months; proportion of participants
Figure 1: Trial profile with well controlled blood pressure at 6 months and
*Of the 30 participating communities, 15 were from Malaysia and 15 were from Colombia. For both countries, 12 months (SBP <140 mm Hg); and change in smoking
seven communities were randomly assigned to intervention and eight communities were randomly assigned to status at 6 months and 12 months. Tertiary outcomes
control. †These participants withdrew their consent form before the second screening. Eligibility could therefore
not be determined.
included change in INTERHEART Risk Score21 at
6 months and 12 months and Cholesterol Modifiable
Risk Score at 12 months; change in lifestyle modification
Control (n=727) Intervention (n=644)
(ie, exercise and diet, based on components of the
Age, years 65·8 (9·7) 65·1 (9·1) INTERHEART Risk Score); proportion of participants
Sex receiving two or more antihypertensive drugs and a
Female 395 (54%) 372 (58%) statin at 6 months and 12 months; and medication
Male 332 (46%) 272 (42%) adherence at 6 months and 12 months (adherence was
Education assessed using the Morisky Medication Adherence Scale
None, primary, or unknown 499 (69%) 446 (69%) 8 in participants actively taking antihypertensive drugs
Secondary or high school 201 (28%) 170 (26%) in both groups; appendix p 4).22 Medication adherence
Trade, college, or university 27 (4%) 28 (4%) was reinforced by NPHWs and treatment supporters as
Past medical history (self-reported) part of the study protocol.7 Safety outcomes were any
Current smoker 68 (9%) 50 (8%) serious adverse events reported in the intervention
Diabetes 270 (37%) 206 (32%) group and clinical events (death, myocardial infarction,
(Table 1 continues on next page) stroke, and cardio vascular-related hospitalisations) at
6 months and 12 months in both groups.
4 www.thelancet.com Published online September 2, 2019 http://dx.doi.org/10.1016/S0140-6736(19)31949-X
Articles
Statistical analysis
Control (n=727) Intervention (n=644)
The study planned to include 1200 participants (40 par
ticipants from each of the 30 communities; 600 in the (Continued from previous page)
intervention group and 600 in the control group). Based History of known hypertension 523 (72%) 485 (75%)
on findings from PURE study participants who met History of known hypertension and taking 441 (61%) 444 (69%)
antihypertensive medication
criteria for HOPE 4,5 we assumed a within-community
Atrial fibrillation 5 (1%) 12 (2%)
intraclass correlation coefficient of 0·05 for all outcomes,
Stroke 15 (2%) 15 (2%)
a baseline FRS of 24·7% (SD 15%), a mean SBP of
Myocardial infarction 30 (4%) 25 (4%)
160 mm Hg (SD 19), and a mean LDL of 3·58 mmol/L
Angina 19 (3%) 14 (2%)
(SD 1·09 mmol/L). Power was 80% to detect at least
a 3·0% absolute difference in the FRS, a 2·9 mm Hg Congestive heart failure 29 (4%) 29 (5%)
difference in blood pressure, and a 0·32 mmol/L dif Liver disease 2 (<1%) 8 (1%)
ference in LDL between the two randomised groups. Kidney disease 12 (2%) 18 (3%)
The analysis of both primary and secondary outcomes Baseline medication use
accounted for the clustering effect and used a mixed One antihypertensive 185 (25%) 205 (32%)
effects model considering community as a random Two antihypertensives 155 (21%) 154 (24%)
intercept effect. An intention-to-treat analysis was done.23 Three antihypertensives 82 (11%) 77 (12%)
Data at 12 months were available from 97% of participants Four or more antihypertensives 28 (4%) 22 (3%)
who were confirmed to be living. We used multiple Statin 195 (27%) 186 (29%)
imputation based on information recorded at baseline to Criteria for enrolment into the study
take into account the 3% missing data for the primary SBP ≥160 mm Hg at one visit 195 (27%) 175 (27%)
outcome as a sensitivity analysis. Two-sided tests at the SBP 140–159 mm Hg in one visit and previous diagnosis 315 (43%) 320 (50%)
0·05 level were considered to be statistically significant. of hypertension or use of antihypertensive medication
Final results are expressed as mean (95% CI) in each SBP ≥130 mm Hg in one visit and a diagnosis of diabetes 125 (17%) 73 (11%)
or use of medications for diabetes
group, and two-sided p values.
Did not meet above criteria but SBP of 140–159 mm Hg 92 (13%) 76 (12%)
The consistency of treatment effects on the primary recorded on two separate visits, at least one day apart
outcome were explored in predefined subgroups, Physical measurements
including sex, education, country, urban or rural com SBP, mm Hg 151·7 (15·6) 152·1 (15·4)
munity, and age younger or older than 65 years.7 We
DBP, mm Hg 85·3 (11·9) 84·7 (12·0)
tested whether the effects varied by subgroups using
Waist, cm 93·6 (11·6) 93·2 (10·8)
tests of interactions between subgroup variables and
Hip, cm 100·2 (10·5) 100·2 (10·4)
treatment group. All analyses were done using SAS,
Waist to hip ratio 0·94 (0·1) 0·93 (0·1)
version 9.2.
Body-mass index, kg/m² 27·7 (5·1) 28·3 (5·3)
Laboratory measures, mmol/L
Role of the funding source
Total cholesterol 5·4 (1·2) 5·4 (1·2)
The authors are solely responsible for the design and
LDL 3·4 (1·1) 3·3 (1·1)
conduct of this study, all study analyses, the drafting and
HDL 1·1 (0·4) 1·2 (0·4)
editing of the Article, and its final contents. The external
Triglycerides 2·0 (1·4) 2·0 (1·4)
funders had no role in the design, conduct, analyses, or
Glucose 6·8 (3·4) 6·5 (3·0)
interpretation of the results. SY, J-DS, SI, TM, PL, and
SIB had full access to the study data. SY and J-DS were Framingham Risk Score 10-year risk estimate
jointly responsible for the decision to submit the Article. 10-year risk estimate 35·5% (22·3) 32·6% (21·4)
<30% 371 (51%) 379 (59%)
Results 30–40% 121 (17%) 98 (15%)
Between 2014 and 2017, 4904 participants were screened ≥40% 235 (32%) 167 (26%)
from 30 communities in Colombia and Malaysia Data are mean (SD) or n (%). SBP=systolic blood pressure. DBP=diastolic blood pressure.
(15 each). All screening in Colombia was door to door,
whereas screening of most participants (n=2383, 88%) Table 1: Baseline characteristics of participants
in Malaysia was done at non-medical community events.
1900 people were invited to participate in the study, and analyses; thus, 1371 participants were included in the
1376 (72%) provided written informed consent. The final analysis. 16 communities (n=727) were randomly
proportion of eligible participants versus those enrolled assigned to the control group and 14 (n=644) were
was higher in Colombia (n=616, 86%) than Malaysia randomly assigned to the intervention group. Similar
(n=760, 60%). However, the results were clear, with a (low) numbers of deaths, withdrawals, and losses to
similar magnitude and statistical significance in both follow-up were noted in both groups. Both groups
countries. Five participants died before randomisation were followed for 12 months and all 30 clusters
of their community, and were not included in the completed follow-up. At study completion, 1299 (97% of
www.thelancet.com Published online September 2, 2019 http://dx.doi.org/10.1016/S0140-6736(19)31949-X 5
Articles
participants confirmed to be alive; n=692 control, n=607 simplified management algorithms on 2886 occasions
intervention) completed 12-month follow-up visits (93%).
(figure 1). There was high fidelity of the intervention imple
Baseline characteristics of the study participants mentation. Participants attended 2970 (94%) of the total
were generally similar between the randomised groups planned NPHW visits (n=3160) in the intervention
(table 1). However, there were more smokers (n=68, group. Additionally, a greater proportion of participants
9·4% vs n=50, 7·8%) and individuals with diabetes in the intervention group were taking two or more
(n=270, 37% vs n=206, 32%) in the control group. antihypertensive medications than the control group at
The intervention and control communities were well 6 months (n=451 [87%] vs n=317 [65%]; p<0·0001) and
balanced, with respect to mean age, population size, and 12 months (n=463 [84%] vs n=322 [65%]; p<0·0001).
access to primary and secondary medical facilities within A significantly higher proportion of statin use was
each community (table 2). The majority of participants reported in participants in the intervention group
(n=1008, 73·5%) had a history of hypertension and were than the control group at 6 months (n=506 [86%] vs
taking anti hypertensive medications, but their blood n=245 [36%]; p<0·0001) and 12 months (n=511 [84%] vs
pressure was not controlled. The remaining patients n=262 [38%]; p<0·0001). In the intervention group,
had newly diagnosed hypertension (table 1). The mean 346 (54%) participants and 314 (49%) participants were
duration of fasting before obtaining blood samples was taking the free study-associated combination antihyper
similar in both groups (control 9·7 h, SD 3·0); inter tensive and statin medication, respectively, at the first
vention 9·8 h (SD 2·9) follow-up visit. 156 (45%) participants taking the study-
NPHWs were found to be consistently accurate in their associated antihypertensives were on the high-dose
ability to identify cardiovascular risk (patient identified by combination at 1 year. 44 (7%) participants in the
NPHWs as having poorly controlled blood pressure and intervention group were taking the three-drug
medication was indicated) and recommend appropriate antihypertensive combination at any visit. Adherence to
therapies (antihypertensives and statin as per the study prescribed antihypertensives in the intervention group
algorithm) when compared with the assessment by local was higher than the control group at 6 months
primary care physicians. Of 3177 assessments in the (n=310 [56%] vs n=172 [35%]; p<0·0001) and 12 months
intervention group, there was a high proportion of (n=351 [61%] vs n=200 [40%]; p<0·0001). Treatment sup
agreement between the NPHWs and physicians on the porters were most commonly a spouse (n=228, 48%),
participants, cardiovascular risk (n=3129; 99%) and offspring (n=159, 34%), other family (n=51, 11%) or
identification of contraindications to antihypertensives another individual (n=34, 7%) and were present at 971
and statin (n=3123; 98%). Of 3116 assessments, the (74%) visits by the NPHWs in the intervention group.
NPHWs and physicians agreed on the need to initiate The reduction in FRS 10-year cardiovascular disease
antihypertensive and statin medications based on the risk was –6·40% (95% CI 8·00 to –4·80) in the control
group and –11·17% (–12·88 to –9·47) in the intervention
group, with a difference of change of –4·78% (95% CI
Control Intervention –7·11 to –2·44; p<0·0001; table 3). In the intervention
(n=16) (n=14) group, there was a 34·2% relative reduction in the FRS
Distance from the coordinating 68·4 (72·0) 68·3 (78·0) estimate compared with baseline. When considering an
centre, km
intention-to-treat analysis, using multiple imputation
Population of communities 56·9 (90·0) 58·3 (127·0)
to account for missing data at 12 months, the results
included, thousands
were unchanged (FRS at 12 months –6·29 vs –11·34;
Number of clinics 6·9 (8·4) 6·6 (8·2)
p<0·0001). When body-mass index was used in place of
Public clinics 2·1 (1·2) 1·9 (1·2)
missing HDL and total cholesterol values (7% of
Private clinics 9·4 (9·0) 9·4 (8·0)
participants) at 12 months, the results were also similar.
Number of hospitals 1·5 (1·2) 1·5 (1·4)
The effects on the primary outcome were consistent in
Public hospitals 1·0 (0·0) 1·1 (0·4)
all predefined subgroups (with statistically significant
Private hospitals 1·0 (1·6) 1·1 (1·3)
differences within both countries), with no evidence of
Tertiary care centres 0·3 (0·5) 0·5 (0·7)
heterogeneity of the effects of intervention (figure 2).
Specialist centres 0·1 (0·5) 0·1 (0·3)
Exploratory post-hoc subgroup analysis considering
Sex
baseline blood pressure, pre-existing hypertension,
Female 50·7% (3·2) 49·4% (2·4) diabetes, and smoking status showed consistent effects
Male 49·3% (4·6) 50·6% (2·3) on the primary outcome (appendix p 5).
Age ≥50 years in the population 25·9% (3·9) 23·3% (4·1) Most of the secondary outcomes showed reductions
Data are mean (SD). *Data from the Bureau of Statistics in Malaysia and the consistent with the primary outcome. There was a greater
Department of Statistics in Colombia. absolute reduction in SBP by 11·45 mm Hg (95% CI
–14·94 to –7·97; figure 3), by 0·45 mmol/L in total
Table 2: Characteristics of intervention and control communities*
cholesterol, and by 0·41 mmol/L (95% CI –0·60 to –0·23)
6 www.thelancet.com Published online September 2, 2019 http://dx.doi.org/10.1016/S0140-6736(19)31949-X
Articles
Baseline Change at 12 months from baseline* Difference in change Test between
between intervention intervention and
and control control† (p value)
Control (n=727) Intervention (n=644) Control (n=692) Intervention (n=607)
Mean Framingham Risk Score 10-year 35·47% (22·34) 32·63% (21·37) –6·40% (–8·00 to –4·80) –11·17% (–12·88 to –9·47) –4·78% (–7·11 to –2·44) <0·0001
risk estimate
Cholesterol modifiable risk score 12·39 (5·51) 11·85 (5·17) –1·64 (–2·26 to –1·02) –4·75 (–5·41 to –4·09) –3·11 (–4·01 to –2·20) <0·0001
Total cholesterol, mmol/L 5·37 (1·20) 5·35 (1·21) –0·23 (–0·35 to –0·12) –0·68 (–0·81 to –0·56) –0·45 (–0·62 to –0·28) <0·0001
LDL, mmol/L 3·38 (1·11) 3·34 (1·13) –0·19 (–0·32 to –0·06) –0·60 (–0·74 to –0·47) –0·41 (–0·60 to –0·23) <0·0001
Triglycerides, mmol/L 2·04 (1·42) 2·00 (1·41) 0·12 (0·01 to 0·23) 0·08 (–0·04 to 0·20) –0·04 (–0·20 to 0·13) 0·6413
HDL, mmol/L 1·14 (0·40) 1·19 (0·41) 0·07 (0·03 to 0·11) 0·04 (–0·01 to 0·08) –0·03 (–0·09 to 0·03) 0·3168
Glucose, mmol/L 6·77 (3·39) 6·51 (2·99) 0·21 (0·01 to 0·41) –0·04 (–0·25 to 0·17) –0·25 (–0·54 to 0·04) 0·0949
Data are mean (SD) or mean (95% CI). *The means and 95% CIs are for the within-person differences. †Test statistic and corresponding p value refers to the test of difference between intervention and control
groups at 12 months’ follow-up using generalised linear mixed effects models adjusting for baseline value, and including community as a random intercept effect to take into account the clustered
randomisation design.
Table 3: Outcomes at 12 months
N Mean (95% CI) pinteraction
Country
Colombia 690 –4·25 (–7·45 to –1·05)
0·74
Malaysia 545 –5·22 (–8·88 to –1·56)
Location
Urban 659 –4·74 (–8·26 to –1·22)
0·92
Rural 576 –4·83 (–7·99 to –1·66)
Sex
Female 688 –4·66 (–6·86 to –2·45)
0·72
Male 547 –5·08 (–8·25 to –1·91)
Age
Women ≤65 years or men ≤55 years 478 –3·80 (–6·30 to –1·30)
0·31
Women >65 years or men >55 years 757 –4·96 (–7·96 to –1·95)
Education
Primary or less 850 –4·52 (–7·23 to –1·81)
Secondary or higher 337 –5·05 (–8·58 to –1·52) 0·16
Trade, college, or university 48 –1·45 (–7·95 to 5·06)
Overall 1235 –4·78 (–7·11 to –2·44)
–10 –8 –6 –4 –2 0
Difference in mean (95% CI)
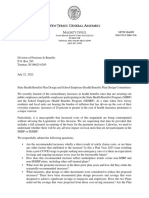
Figure 2: Differences in Framingham Risk Score for 10-year cardiovascular disease risk between intervention and control groups
in LDL at 12 months in the intervention compared with no significant differences in glucose concentrations,
the control group (p<0·0001; table 3). Furthermore, the HDL, smoking cessation rates, and weight between the
change in blood pressure control (<140 mm Hg) status two groups at 12 months (appendix p 7).
was more than double in the intervention group (69% vs 18 serious adverse events were reported in intervention
31%; p<0·0001) at 12 months. There was a trend to benefit participants who were taking study-associated medi
for most health behaviours in the intervention group, cations (644 participants). In all reported cases, the
resulting in a substantial reduction in the overall study-associated medication was identified to be unre
INTERHEART Risk Score at 6 months (–1·9 [SD 5·6] vs lated to the event and the medication was continued
–4·5 [SD 5·4]; p=0·0008) and 12 months (–2·2 [SD 5·8] vs in 17 of 18 (94%) events. There were no significant
4·8 [SD 5·4]; p<0·0001; table 4). In particular, there differences in deaths (n=12 [2·0%] vs n=15 [2·1%]),
were improvements in reports of physical activity and myocardial infarction (n=7 [1·2%] vs n=12 [1·7%]), stroke
dietary modifications (appendix p 7). However, there were (n=5 [0·8%] vs n=6 [0·9%]), their composite (n=23 [3·8%]
www.thelancet.com Published online September 2, 2019 http://dx.doi.org/10.1016/S0140-6736(19)31949-X 7
Articles
vs n=32 (4·6%)], or cardiovascular hospitalisations
A
4·0 Control
(n=35 [5·8%] vs n=27 [3·9%]) between the intervention
Intervention and control groups, respectively.
3·8
3·6 Discussion
LDL cholesterol (mmol/L)
3·4
A comprehensive, contextually appropriate model of care
resulted in a substantial reduction in cardiovascular
3·2
disease risk in two middle-income countries primarily
3·0 through improvements in blood pressure, LDL, and some
2·8 health behaviours. Other studies using NPHWs have
shown a modest increased uptake of antihypertensives
2·6
without translating into a reduction in blood pressure.24,25
0 We showed a large reduction in blood pressure and cardio
0 6 12
vascular disease risk, something significant for a
Visit (months)
Control Intervention Control Intervention
community-based intervention. We believe that a major
(N=636) (N=585) (N=636) (N=585) reason for its success was that our intervention package
Mean (95% CI) 3·38 3·34 3·21 2·75 explicitly targeted barriers identified through extensive
(3·30–3·46) (3·25–3·43) (3·13–3·28) (2·67–2·84)
health system appraisals, a step that is frequently omitted
B in developing complex interventions. These appraisals
160 Control pointed to a need for a comprehensive strategy, bringing
Intervention together elements tackling the main health systems
155
building blocks, in contrast with previous studies that have
Systolic blood pressure (mm Hg)
150 addressed only one or a few barriers. The strategy evaluated
145 here was an intervention led by NPHWs in conjunction
with primary care physicians and family, coupled with the
140
provision of free antihypertensives and a statin, as well as
135 strategies to improve adherence to medication and health
130 behaviours. It is a comprehensive and collaborative model
of care. The approach of door-to-door and community
125
event screening identified and led to the management of
0 individuals with previously undiagnosed hypertension
0 6 12
Visit (months) and uncontrolled hyper tension. To our knowledge, our
Control Intervention Control Intervention Control Intervention study is the only cluster-randomised controlled trial
(N=674) (N=602) (N=665) (N=587) (N=674) (N=602) of a comprehensive programme that addresses major
Mean (95% CI) 151·75 152·05 142·40 131·47 141·99 130·60 contextual barriers to cardiovascular risk detection,
(150·62– (150·88– (140·8– (130·1– (140·48– (129·35–
152·88) 153·25) 144·0) 132·9) 143·49) 131·83) treatment, and control in middle-income countries.
A recent systematic review of task sharing for the
Figure 3: Change in LDL and systolic blood pressure and over time in the intervention and control groups management of blood pressure in low-income and
Baseline Change at 6 months from baseline* Test between Change at 12 months from baseline* Test between
intervention intervention
and control and control at
at 6 months 12 months†
(p value) (p value)
Control Intervention Control Intervention Control Intervention
(n=727) (n=692) (n=674) (n=589) (n=692) (n=607)
SBP, mm Hg 151·8 (15·6) 152·1 (15·4) –9·0 (–11·4 to –6·7) –20·1 (–22·7 to –17·6) <0·0001 –9·7 (–12·1 to –7·3) –21·1 (–23·7 to –18·6) <0·0001
DBP, mm Hg 85·3 (11·9) 84·7 (12·0) –2·6 (–4·2 to –1·0) –6·1 ( –7·8 to –4·4) 0·0026 –2·9 (–4·4 to –1·4) –6·9 (–8·5 to –5·3) 0·0004
Controlled SBP <140 mm Hg 125 (17·2%) 74 (11·5%) 30·1 (25·6 to 34·7) 63·4 (59·2 to 67·6) <0·0001 30·4 (25·8 to 34·9) 68·9 (64·9 to 72·9) <0·0001
Controlled SBP <140 mm Hg 115 (15·8%) 68 (10·6%) 29·4 (24·9 to 33·9) 59·2 (54·9 to 63·5) <0·0001 28·4 (24·0 to 32·9) 64·8 (60·7 to 68·9) <0·0001
and DBP <90 mm Hg
INTERHEART Risk Score21 14·8 (6·1) 13·8 (5·3) –1·6 (–2·7 to –0·5) –4·4 (–5·6 to –3·2) 0·0008 –1·9 (–2·9 to –0·9) –4·9 (–5·9 to –3·8) <0·0001
Data are mean (SD) or n (%). SBP=systolic blood pressure. DBP=diastolic blood pressure. *The means and 95% CIs are for the within-person differences. †Test statistic and corresponding p value refers to the test
of difference between intervention and control groups at 12 month’s follow-up using generalised linear mixed effects models adjusting for baseline value, and including community as a random intercept effect
to take into account the clustered randomisation design.
Table 4: Secondary and tertiary outcomes at 6 and 12 months
8 www.thelancet.com Published online September 2, 2019 http://dx.doi.org/10.1016/S0140-6736(19)31949-X
Articles
middle-income countries reported reductions in SBP pressure or risk factors because they were not followed up
with a mean of 4·8 mm Hg (95% CI 3·6–6·1).26 The with pharmacological treatments.28,29 HOPE 4 overcomes
benefits varied depending on the type of NPHWs this by coupling community screening with a multifaceted
involved in the intervention.26 The best results were intervention, including the prescription and provision of
achieved with pharmacists (–8·1 mm Hg) as compared antihypertensive medications and statins, resulting in
with community health workers (–3·7 mm Hg) as the substantial reductions in cardiovascular disease risk.
NPHWs and when NPHWs were guided by a protocol or Furthermore, home visits by NPHWs helped to address
decision support.26 However, effects were limited by the common barriers to attending medical clinics.12,13 One-
NPHWs’ inability to prescribe effective medications or third of study participants reported that they had to travel
lack of availability of medications. This review noted that by taxi or use public transportation to attend physician
there is a need for further research assessing community- visits in the past. This time and expense, along with lost
based, collaborative models of care. The HOPE 4 inter wages, was identified as a barrier in the initial health
vention was informed by extensive previous work on system appraisals. The community-based component
barrier assessments and health system appraisals done of the intervention probably contributed to improved
in both Colombia and Malaysia to target barriers to adherence to medical follow-up, a necessity for optimal
cardiovascular risk reduction (appendix p 6).7–9,12,13 cardiovascular risk management.
The HOPE 4 study advances our understanding of how Fourth, the HOPE 4 intervention involved task sharing
NPHWs can be more effective in reducing cardiovascular in a collaborative model involving NPHWs, physicians,
disease risk in several ways. First, with proper training and family members, as recommended by WHO.30,31
and supervision, even individuals with minimal training This strategy addresses the health system barriers we
can learn to successfully use a tablet-based decision identified relating to physician shortages and policies
support system to diagnose and counsel individuals that limit the NPHWs’ ability to prescribe medications.
with respect to their cardiovascular disease risk.17 This By training NPHWs and supporting them with mobile-
is evidenced by the accuracy of the NPHWs’ risk health decision support to screen, diagnose cardiovascular
assessments and treatment recommendations when disease risk, and recommend effective medications, the
compared with the primary care physician. Furthermore, management of cardiovascular disease risk by local
the effect of the NPHW’s counselling of the participant physicians is made easier and more efficient.7 The
and treatment supporter is shown by the improvement in HOPE 4 approach to initiating combination antihyper
several health behaviours (captured in the INTERHEART tensive drugs requiring only one or two blood pressure
Risk Score) and the significant reductions in blood measurements (with simultaneous reductions in lipids
pressure and LDL in the intervention group. and other risk factors) resulted in a substantial reduction
Second, our study was an international cluster-ran in 10-year cardiovascular disease risk as compared with
domised controlled trial that showed success in urban the control group, and the change in blood pressure
and rural settings in two different countries and control was more than double in the intervention group.
continents, with widely varying health systems and Furthermore, this simplified approach limits the need
cultural backgrounds, which suggests our findings are for multiple medical visits, resulting in additional savings
widely applicable. Given that country-specific barrier beyond the cost-effective strategy of using NPHWs in
assessments informed the design of HOPE 4, such low-resource settings.11 These findings and experiences
approaches would need to be considered to tailor the might also be applicable to high-income countries, as
intervention in different settings. Furthermore, the the detection, treatment, and control of hypertension
intervention was effective in all subgroups, including and other cardiovascular disease risk factors is also
men and women, and those of different ages, with suboptimal in these settings.4
differing education levels, in both countries, and in rural Fifth, the HOPE 4 study overcame significant health
and urban communities. It should be noted that there system barriers relating to the cost and availability of
was a non-significant trend for the intervention to be less antihypertensive and statin medications in low-income
effective in participants with higher education; however, and middle-income countries by providing free locally
most HOPE 4 participants (69%, n=945) had low educa sourced medications to eligible participants in the
tion; such populations have higher risk of cardiovascular intervention group. It is well established that blood
disease.27 pressure control is better achieved using combinations
Third, our study used a community-based intervention; of low doses of antihypertensive agents, an approach
participants were recruited from their homes, community endorsed by several guidelines.32–35 Furthermore, single-
outreach centres, or events based within public spaces. pill combination antihypertensives have been recently
Unlike studies based in medical clinics, which only added to the WHO essential medicine list.36 Given
include those who seek medical help, our approach evidence supporting the use of statins in individuals with
overcomes the traditionally low detection of hypertension hypertension regardless of lipid concentrations, this
in the community. Previous efforts of systematic screening medication was also recommended and used in eligible
alone have had little additional effect in reducing blood participants.37–41 Higher proportions of combination
www.thelancet.com Published online September 2, 2019 http://dx.doi.org/10.1016/S0140-6736(19)31949-X 9
Articles
antihypertensive (89% vs 55%) and statin medications intervention and control groups, meaning that the
(89% vs 32%) were seen at 12 months in the intervention differences in cardiovascular disease risk reductions
group, showing the success of the intervention imple between the intervention and control groups we observed
mentation. Although free medication is an important are likely to be an underestimate of the full effects of
component of the intervention and might explain the our intervention strategy. Second, contamination was a
large effects on blood pressure reduction, it probably potential risk, but it was minimised by the cluster design
does not account for the full effect of the HOPE 4 strategy. because only the communities randomly assigned to the
Other studies have shown a benefit to task sharing with intervention had access to NPHW counselling (guided by
NPHWs despite medications being provided for free in the intervention tablet application only), management
both the intervention and control groups.42 algorithms (inter vention tablet application only), and
Finally, the HOPE 4 intervention actively involved the free study medications. In addition, communities were
participant’s family and friends as treatment supporters chosen with adequate geographical separation from each
in their management of cardiovascular disease risk. other. This approach was successful because we saw
The treatment supporters were encouraged to help the marked differences in reduction of blood pressure,
participants adhere to their medications and healthy lipids, and several other risk factors. Third, blinding was
behaviours between NPHW and physician visits. Such a not feasible in HOPE 4, which tested two strategies;
strategy has been shown to be effective at improving however, several steps were implemented to minimise or
medication adherence and mortality in patients with avoid potential biases. Masking outcome assessors or
HIV.16 Three-quarters of our intervention participants using a separate set of assessors to record risk factors
had their treatment supporter present during inter during follow-up was not feasible in a large study
vention visits, suggesting that they were actively engaged involving several communities. Substantial additional
in the participant’s management. Medication adherence resources would have been needed to hire, train, and
to antihypertensive drugs and statins was found to be oversee a second national team in each country, to do
better in the intervention group. Further supporting the duplicate visits at 6 months and 12 months, and to
role of treatment supporters and counselling from the develop separate streams of data collection processes and
NPHWs, there was a trend toward improvements in tablet software. Therefore our approach of ensuring that
several reported healthy behaviours (appendix p 7); the blood pressure recordings were from automated
however, there was no significant change in smoking devices and lipids were measured centrally without
rates, weight, or HDL at 12 months. knowledge of whether they were from intervention or
The HOPE 4 study was not designed to assess the control communities minimised biases in the most
safety of specific antihypertensive medications or statins practical manner possible for the two key outcomes of
used in the study; however, there was no excess in the trial. The extensive analyses undertaken to confirm
adverse events reported in the intervention group. that there was no bias in the blood pressure recorded in
All study-provided medications were purchased from HOPE 4 are reported in the appendix (p 8). Fourth,
approved, commercially available supplies within each surrogate outcomes were used in this study. There is
country, and are commonly used in clinical practice. good evidence to support improved clinical outcomes
NPHWs were found to accurately assess cardiovascular with the reductions in blood pressure and LDL shown in
disease risk, medication contraindications, and treatment this trial. To show a benefit in clinical events, a much
recommendations when compared with physicians. This larger and longer trial would be required. It was not the
supports the need to consider changes in regulations that goal of our study to examine the direct effect of our
would allow trained NPHWs to prescribe a limited intervention on clinical events but instead to develop and
number of commonly used drugs, such as safe anti test more effective implementation strategies to reduce
hypertensive drugs and statins.10 risk factors in those with hypertension. The ASCOT-LLA
Our study has some potential limitations. First, trial,37 the analysis of those with elevated blood pressure
participants in the control group were screened for in the HOPE 3 trial,38 and the results of the PolyIran
cardiovascular disease risk at baseline, had their blood trial43 indicate that substantial reductions in cardio
pressure assessed, and were provided with information vascular disease will occur from reducing both blood
about local cardiovascular disease health programmes pressure and lipids in individuals with elevated blood
and recommendations to see a health-care provider as pressure. Fifth, given the stratified randomisation by
appropriate. Therefore, our screening was an intervention country, there were an uneven number of clusters in the
in itself, because some participants in the control group intervention and control groups, leading to an imbalance
might have modified their behaviour after learning their of some characteristics. However, sensitivity analysis,
blood pressure was elevated, which could have led to adjusting for differences in baseline characteristics
more people in the control communities receiving including country, age, sex, education, baseline use of
treatment than would be the case in usual care. This antihypertensives, hypertension, diabetes, and smoking
modification might have reduced the real differences status did not significantly change the primary outcome.
in primary and secondary outcomes between the Finally, the single-pill combination antihypertensive and
10 www.thelancet.com Published online September 2, 2019 http://dx.doi.org/10.1016/S0140-6736(19)31949-X
Articles
statin medications were provided free to participants in proposed use of the data by a review committee created by leaders of the
the intervention group and were paid for as part of the study. This review will serve to ensure that patient privacy and rights,
and data and research integrity, can be maintained. Review criteria will
HOPE 4 study. Although some countries provide these include demonstrated competence in data security and analysis and data
medications at low or no cost, this is not the case in will be shared to achieve the objectives in the approved protocol only.
several other countries. We hope that the combined Individual participant data and a data dictionary will be made available,
effect of our results, in the context of the ASCOT-LLA,37 subject to requirements or restrictions from research ethics board or
institutional review boards, existing contracts or agreements,
HOPE 3,38 and PolyIran trial43 results, along with the and conditions set forth in participant consent forms. Data provided will
inclusion of combination antihypertensive drugs and be limited to data which underlies the results in the main publication.
statins in the Essential Medicines List will persuade after de-identification. The protocol and statistical analysis plan for
governments to provide such medicines at low or no cost analysis of the primary results will be shared. Data can be disclosed from
2 years after the main paper is published, plus 6 additional months for
to those with hypertension. This would overcome a key every year of study conduct, to a maximum of 7 years. Data will be made
barrier (cost and availability of medicines) to improved available through secure data transfer methods overseen by the
control of hypertension and reduction of cardiovascular Population Health Research Institute (PHRI), or by having analyses
disease. performed by the PHRI Department of Statistics, subject to capacity.
Each proposal must identify and provide funding to defray the costs of
A comprehensive model of care led by trained NPHWs data preparation, storage, transfer, and analysis for the organisation
with physicians and family members resulted in a sub incurring these costs.
stantial reduction in estimated cardiovascular dis ease Acknowledgments
risk, primarily through improvements in blood pressure, We thank our funders and partners at WHO for their collaboration on
LDL, medication adherence, and some health behaviours. the NPHW training curriculum at the onset of this project.
In addition, this study led to the detection of hypertension We acknowledge support from the following physicians in Malaysia and
Colombia: Ng Kien Keat, Khairul Shafiq Ibrahim, Adibah Hanim Ismail,
and consequent initiation of treatment in a significant Norhaslira Abdul Rahim, Noor Hasliza Hassan, Ruziaton binti Hasim,
number of individuals who otherwise were unlikely to Nor Anizah bt Muzaid, Sabariah Idris, Johanna Otero,
have been diagnosed or managed in the near future. The Jose Patricio López-López, Sandra Rueda-Quijano, and
Luz Maria Gomez-Peña. This work was supported by the Canadian
HOPE 4 strategy could help to attain the UN General
Institutes of Health Research (CIHR) and Grand Challenges Canada
Assembly Action Plan for a one-third reduction in (GCC), as part of the Global Alliance for Chronic Disease program
premature mortality from cardiovascular disease.44 On (CIHR grant number 120389; GCC grant numbers 0069–04 and
the basis of the substantial reductions in cardiovascular 0070–04); CIHR’s Strategy for Patient Oriented Research (SPOR),
through the Ontario SPOR Support Unit, as well as the Ontario Ministry
disease risk and the improvements in blood pressure
of Health and Long-Term Care; an unrestricted grant from Boehringer
control shown (as well as the additional benefits of Ingelheim; the Department of Management of non-communicable
community screening), this target is achievable if health diseases, WHO; the Santander Departmental Secretary of Health,
system strategies, such as the one evaluated here, are Bucaramanga, Colombia; and the Population Health Research Institute.
This research programme does not represent the official view of the
adapted to local contexts and then adopted.
Global Alliance for Chronic Diseases, WHO, or the governments of
Contributors Canada, Malaysia, or Colombia. No official support or endorsement of
SY designed and supervised the study and data analysis, interpreted this article by the Global Alliance for Chronic Diseases hypertension
the data, and reviewed and commented on all drafts of the Article. programme, WHO, or federal governments of participating countries is
J-DS helped to design and supervise the study, analysed data, led the intended or should be inferred.
writing of the analysis plan, and had the primary responsibility for
References
writing the Article. TM coordinated the study implementation globally,
1 Roth GA, Johnson C, Abajobir A, et al. Global, regional,
and reviewed and commented on all drafts of the Article. SI participated and national burden of cardiovascular diseases for 10 causes,
in writing the analysis plan, did the analysis, and reviewed and 1990 to 2015. J Am Coll Cardiol 2017; 70: 1–25.
commented on all drafts of the Article. MM designed the health systems 2 NCD Countdown 2030 Collaborators. NCD Countdown 2030:
barriers assessment, helped design the intervention package, reviewed worldwide trends in non-communicable disease mortality and
and commented on the data analysis and drafts of the Article. AA, PL, LT progress towards Sustainable Development Goal target 3.4.
and SIB reviewed and commented on the data analysis and drafts of the Lancet 2018; 392: 1072–88.
Article. All other authors implemented the study in their respective 3 Hoffmann R, Plug I, McKee M, et al. Innovations in medical care
countries and provided comments on drafts of the Article. and mortality trends from four circulatory diseases between 1970
and 2005. Eur J Public Health 2013; 23: 852–57.
Declaration of interests
4 Chow CK, Teo KK, Rangarajan S, et al. Prevalence, awareness,
J-DS, TM, PL, SIB, SI, and SY report that their institution received grants
treatment, and control of hypertension in rural and urban
from the Canadian Institutes of Health Research, Ontario Ministry of
communities in high-, middle-, and low-income countries.
Health and Long-Term Care, Boehringer Ingelheim, and the Department JAMA 2013; 310: 959–68.
of Management of Non-Communicable Disease, WHO, for the conduct of
5 Yusuf S, Islam S, Chow CK, et al. Use of secondary prevention
the study. PL-J and PAC report that their institution received unrestricted drugs for cardiovascular disease in the community in
grants from Grand Challenges Canada, and the Santander Departmental high-income, middle-income, and low-income countries
Secretary of Health, during the conduct of the study. KY and FM report (the PURE study): a prospective epidemiological survey. Lancet
that their institution received a grant from Grand Challenges Canada 2011; 378: 1231–43.
during the conduct of the study. MM reports that his institution received a 6 Balabanova D, McKee M, Mills A, Walt G, Haines A. What can
grant from the Canadian Institutes of Health Research. AA reports grants global health instutitions do to help strengthen health systems in
from Canadian Institutes of Health Research during the conduct of the low income countries? Health Res Policy Syst 2010; 8: 22.
study. LT declares no competing interests. 7 Schwalm JR, McCready T, Lamelas P, et al. Rationale and design of
a cluster randomized trial of a multifaceted intervention in people
Data sharing with hypertension: The Heart Outcomes Prevention and
The Population Health Research Institute has a formal data sharing Evaluation 4 (HOPE-4) study. Am Heart J 2018; 203: 57–66.
policy. Data will be disclosed only upon request and approval of the
www.thelancet.com Published online September 2, 2019 http://dx.doi.org/10.1016/S0140-6736(19)31949-X 11
Articles
8 Maimaris W, Paty J, Perel P, et al. The influence of health systems 27 Rosengren A, Smyth A, Rangarajan S, et al. Socioeconomic status
on hypertension awareness, treatment, and control: a systematic and risk of cardiovascular disease in 20 low-income, middle-income,
literature review. PLoS Med 2013; 10: e1001490. and high-income countries: the prospective urban rural
9 Khatib R, Schwalm JD, Yusuf S, et al. Patient and healthcare epidemiologic (PURE) study. Lancet Glob Health 2019; 7: e748–60.
provider barriers to hypertension awareness, treatment and follow 28 Krogsbøll LT, Jørgensen KJ, Grønhøj Larsen C, Gøtzsche PC.
up: a systematic review and meta-analysis of qualitative and General health checks in adults for reducing morbidity and
quantitative studies. PLoS One 2014; 9: e84238. mortality from disease: Cochrane systematic review and
10 Joshi R, Alim M, Kengne AP, et al. Task shifting for meta-analysis. BMJ 2012; 345: e7191.
non-communicable disease management in low and middle income 29 Jorgensen T, Jacobsen RK, Toft U, et al. Effect of screening and
countries—a systematic review. PLoS One 2014; 9: e103754. lifestyle counselling on incidence of ischaemic heart disease in
11 Gaziano T, Abrahams-Gessel S, Surka S, et al. Cardiovascular general population: Inter99 randomised trial. BMJ 2014; 348: g3617.
disease screening by community health workers can be cost-effective 30 Abegunde DO, Shengelia B, Luyten A, et al. Can non-physician
in low-resource countries. Health Aff 2015; 34: 1538–45. health-care workers assess and manage cardiovascular risk in
12 Legido-Quigley H, Lopez PAC, Balabanova D, et al. Patients’ primary care? Bull World Health Organ 2007; 85: 432–40.
knowledge, attitudes, behaviour and health care experiences on the 31 WHO. WHO CVD-risk management package for low- and
prevention, detection, management and control of hypertension in medium-resource settings. Geneva: World Health Organization,
Colombia: a qualitative study. PLoS One 2015; 10: e0122112. 2002.
13 Risso-Gill I, Balabanova D, Majid F, et al. Understanding the 32 López-Jaramillo P, Barbosa E, Molina DI, et al. Latin American
modifiable health systems barriers to hypertension management in consensus on management of hypertension in the patient with
Malaysia: a multi-method health systems appraisal approach. diabetes and the metabolic syndrome. J Hypertens 2019; 37: 1126–47.
BMC Health Serv Res 2015; 15: 254. 33 Mancia G, De Baker G, Dominiczak A, et al. 2007 Guidelines for the
14 Campbell MK, Piaggio G, Elbourne DR, Altman DG, management of arterial hypertension: The Task Force for the
CONSORT Group. Consort 2010 statement: extension to cluster Management of Arterial Hypertension of the European Society of
randomised trials. BMJ 2012; 345: e5661. Hypertension (ESH) and of the European Society of Cardiology
15 WHO. WHO STEPS surveillance manual: the WHO STEPwise (ESC). Eur Heart J 2007; 28: 1462–536.
approach to chronic disease risk factor surveillance. Geneva: 34 Chobanian AV, Bakris GL, Black HR, et al. Seventh report of the
World Health Organization, 2008. Joint National Committee on Prevention, Detection, Evaluation,
16 Nachega JB, Chaisson RE, Goliath R, et al. Randomized controlled and Treatment of High Blood Pressure. J Hypertens 2003; 42: 1206–52.
trial of trained patient-nominated treatment supporters providing 35 Malaysian Society of Hypertension. Working Group on Hypertension.
partial directly observed antiretroviral therapy. AIDS 2010; 24: 1273–80. Clinical Practice Guidelines—Management of Hypertension, 5th edn.
17 Khan M, Lamelas P, Musa H, et al. Development, testing, Malaysia: Malaysian Society of Hypertension, 2018.
and implementation of a training curriculum for nonphysician 36 WHO. World Health Organization model list of essential medicines,
health workers to reduce cardiovascular disease. Glob Heart 2018; 21st list, 2019. Geneva: World Health Organization, 2019.
13: 93–100. 37 Sever PS, Dahlöf B, Poulter NR, et al. Prevention of coronary and
18 D’Agostino RB Sr, Vasan RS, Pencina MJ, et al. General cardiovascular stroke events with atorvastatin in hypertensive patients who have
risk profile for use in primary care: the Framingham Heart Study. average or lower-than-average cholesterol concentrations,
Circulation 2008; 117: 743–53. in the Anglo-Scandinavian Cardiac Outcomes Trial—Lipid
19 Artigao-Rodenas LM, Carbayo-Herencia JA, Divison-Garrote JA, et al. Lowering Arm (ASCOT-LLA): a multicentre randomised controlled
Framingham risk score for prediction of cardiovascular diseases: trial. Lancet 2003; 361: 1149–58.
a population-based study from southern Europe. PLoS One 2013; 38 Yusuf S, Lonn E, Pais P, et al. Blood-pressure and cholesterol
8: e73529. lowering in persons without cardiovascular disease. N Engl J Med
20 Chia YC, Gray SY, Ching SM, et al. Validation of the Framingham 2016; 374: 2032–43.
general cardiovascular risk score in a multiethnic Asian 39 Lonn EM, Bosch J, López-Jaramillo P, et al. Blood-pressure lowering
population: a retrospective cohort study. BMJ Open 2015; in intermediate-risk persons without cardiovascular disease.
5: e007324. N Engl J Med 2016; 374: 2009–20.
21 Yusuf S, Hawken S, Ounpuu S, et al. Effect of potentially modifiable 40 Yusuf S, Bosch J, Dagenais G, et al. Cholesterol lowering in
risk factors associated with myocardial infarction in 52 countries intermediate-risk persons without cardiovascular disease.
(the INTERHEART study): case-control study. Lancet 2004; N Engl J Med 2016; 374: 2021–31.
364: 937–52. 41 Grundy SM, Stone NJ, Bailey AL, et al. 2018 AHA/ACC/AACVPR/
22 Morisky DE, Ang A, Krousel-Wood M, Ward HJ. Predictive validity AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA Guideline
of a medication aderence measure in an outpatient setting. on the Management of Blood Cholesterol. Circulation 2019;
J Clin Hypertens 2008; 10: 348–54. 139: e1082–143.
23 Schafer JL. Analysis of incomplete multivariate data. Boca Raton: 42 Ogedegbe G, Plange-Rhule J, Gyamfi J, et al. Health insurance
CRC Press, 1997. coverage with or without a nurse-led task shifting strategy for
24 Peiris D, Praveen D, Mogulluru K, et al. SMARThealth India: hypertension control: a pragmatic cluster randomized trial in
a stepped-wedge, cluster randomised controlled trial of a Ghana. PLoS Med 2018; 15: e1002561.
community health worker managed mobile health intervention for 43 Roshandel G, Khoshnia M, Poustchi H, et al. Effectiveness of
people assessed at high cardiovascular disease risk in rural India. Polypill for primary and secondary prevention of cardiovascular
PLoS One 2019; 14: e0213708. diseases: a pragmatic cluster randomized controlled trial.
25 Tian M, Ajay VS, Dunzhu D, et al. A cluster-randomized, SSRN 2019; published online June 24. https://ssrn.com/
controlled trial of a simplified multifaceted management program abstract=3408063 (preprint).
for individuals at high cardiovascular risk (simcard trial) in rural 44 Mamudu HM, Yang JS, Novotny TE. UN resolution on the
Tibet, China, and Haryana, India. Circulation 2015; 132: 815–24. prevention and control of non-communicable diseases:
26 Anand TN, Joseph LM, Geetha AV, Prabhakaran D, Jeemon P. an opportunity for global action. Glob Public Health 2011; 6: 347–53.
Task sharing with non-physician health-care workers for
management of blood pressure in low-income and middle-income
countries: a systematic review and meta-analysis. Lancet Glob Health
2019; 7: e761–67.
12 www.thelancet.com Published online September 2, 2019 http://dx.doi.org/10.1016/S0140-6736(19)31949-X
You might also like
- Laboratory Report: Method: Real Time PCRDocument1 pageLaboratory Report: Method: Real Time PCRVisnu SankarNo ratings yet
- 100 Days of Jessica Smith Rotation Using DVDsDocument4 pages100 Days of Jessica Smith Rotation Using DVDsAusra CrowderNo ratings yet
- Smyth Et Al., 2015 (KEEMPAT)Document10 pagesSmyth Et Al., 2015 (KEEMPAT)shofiNo ratings yet
- 10.1016@S0140 67361932317 7Document11 pages10.1016@S0140 67361932317 7DaviSalmissonNo ratings yet
- REWIND TrialDocument10 pagesREWIND Trialhenry hernandezNo ratings yet
- E47 FullDocument7 pagesE47 FullPaula1412No ratings yet
- Angelina Alphonce JohoDocument80 pagesAngelina Alphonce JohoMerlina WijayawatiNo ratings yet
- 15 UsePrescription PDFDocument14 pages15 UsePrescription PDFIJAERS JOURNALNo ratings yet
- Pedro Pallangyo Jakaya Kikwete Cardiac Institute, Tanzania: Archivos de MedicinaDocument2 pagesPedro Pallangyo Jakaya Kikwete Cardiac Institute, Tanzania: Archivos de MedicinaMai Nguyễn Thị NgọcNo ratings yet
- Clortalidona Vs HCLDocument10 pagesClortalidona Vs HCLdiana stefhany marin ramirezNo ratings yet
- Comparison of Medical Versus Surgical Management of Peritonsillar Abscess: A Retrospective Observational StudyDocument6 pagesComparison of Medical Versus Surgical Management of Peritonsillar Abscess: A Retrospective Observational Studycharoline gracetiani nataliaNo ratings yet
- Souza Et Al., 2016Document10 pagesSouza Et Al., 2016Ricardo Costa da SilvaNo ratings yet
- Nihms866890 UPLOAD 3Document21 pagesNihms866890 UPLOAD 3Peter GardinerNo ratings yet
- Meta Statin Induce DMDocument8 pagesMeta Statin Induce DMErvan ZuhriNo ratings yet
- TiroidesDocument289 pagesTiroidesJenny Narva RodriguezNo ratings yet
- ATA Thyroid PDFDocument133 pagesATA Thyroid PDFAlna Shelah IbañezNo ratings yet
- Ata-Thyroid Guidelines - 2015Document299 pagesAta-Thyroid Guidelines - 2015Jessica FranceNo ratings yet
- ATA Tiroides PDFDocument133 pagesATA Tiroides PDFGloria Pg MontzeNo ratings yet
- Thyroid Guideline ATADocument437 pagesThyroid Guideline ATABas FrietmanNo ratings yet
- Thy 2015 0020 PDFDocument271 pagesThy 2015 0020 PDFMade RusmanaNo ratings yet
- (2016.01) 2015 ATA Management Guidelines For Adult Patients With Thyroid Nodules and Differentiated Thyroid Cancer PDFDocument168 pages(2016.01) 2015 ATA Management Guidelines For Adult Patients With Thyroid Nodules and Differentiated Thyroid Cancer PDFfamp_carrijoNo ratings yet
- Improving Medication Safety: Development and Impact of A Multivariate Model-Based Strategy To Target High-Risk PatientsDocument13 pagesImproving Medication Safety: Development and Impact of A Multivariate Model-Based Strategy To Target High-Risk PatientstotoksaptantoNo ratings yet
- Prevalence, Awareness, Treatment, and Control of Hypertension in Rural and Urban Communities in High-, Middle-, and Low-Income CountriesDocument10 pagesPrevalence, Awareness, Treatment, and Control of Hypertension in Rural and Urban Communities in High-, Middle-, and Low-Income CountriesJaqueline OdairNo ratings yet
- On MedDocument10 pagesOn MedShimily LiangNo ratings yet
- Medication Adherence and Blood Pressure Control Among Hypertensive Patients With Coexisting Long-Term Conditions in Primary Care SettingsDocument10 pagesMedication Adherence and Blood Pressure Control Among Hypertensive Patients With Coexisting Long-Term Conditions in Primary Care SettingsmadhurocksktmNo ratings yet
- ST Gallen 1998Document8 pagesST Gallen 1998Nicola CrestiNo ratings yet
- Tsuyuki 2002Document7 pagesTsuyuki 2002Basilharbi HammadNo ratings yet
- Reducing Inappropriate Polypharmacy The Process of DeprescribingDocument8 pagesReducing Inappropriate Polypharmacy The Process of DeprescribingThiago SartiNo ratings yet
- Name of The Candidate and AddressDocument16 pagesName of The Candidate and AddressYash RamawatNo ratings yet
- A Pituitary Society Update To Acromegaly Management GuidelinesDocument13 pagesA Pituitary Society Update To Acromegaly Management Guidelinesyongky amaloNo ratings yet
- Ahmad 2018Document14 pagesAhmad 2018Cristopher OchoaNo ratings yet
- NcologistDocument7 pagesNcologistNafia TurariezaNo ratings yet
- Factors Associated With Acute and Late Dysphagia in The DAHANCA 6 7 Randomized Trial With Accelerated Radiotherapy For Head and Neck CancerDocument9 pagesFactors Associated With Acute and Late Dysphagia in The DAHANCA 6 7 Randomized Trial With Accelerated Radiotherapy For Head and Neck CancerNurul Afika LubisNo ratings yet
- Nejmoa 1606220Document10 pagesNejmoa 1606220Jay TiwariNo ratings yet
- GAVILA Et Al 2016 Evaluation and Management of Chemotherapy-InducedDocument14 pagesGAVILA Et Al 2016 Evaluation and Management of Chemotherapy-InducedKevin AdrianNo ratings yet
- Articles: BackgroundDocument13 pagesArticles: BackgroundDita Putri DamayantiNo ratings yet
- Pathology and Laboratory Medicine in Low-Income and Middle-Income Countries 1Document12 pagesPathology and Laboratory Medicine in Low-Income and Middle-Income Countries 1Abraham DiazNo ratings yet
- LeaderDocument12 pagesLeaderMoeez AkramNo ratings yet
- E2 Journal of Hypertension Vol 35, E-Supplement 3, November 2017Document1 pageE2 Journal of Hypertension Vol 35, E-Supplement 3, November 2017Sadam_fasterNo ratings yet
- MIMS Doctor August 2015 RGDocument48 pagesMIMS Doctor August 2015 RGDika MidbrainNo ratings yet
- Sys Rev TT of Intermittent ClaudicationDocument20 pagesSys Rev TT of Intermittent ClaudicationMaria PopNo ratings yet
- ADHD Medications and Risk of Serious Cardiovascular Events in Young and Middle-Aged AdultsDocument11 pagesADHD Medications and Risk of Serious Cardiovascular Events in Young and Middle-Aged AdultsGary KatzNo ratings yet
- Jco 2003 04Document8 pagesJco 2003 04fatimaramos31No ratings yet
- Prescription Patterns of Antihypertensives in A Community Health Centre in Mexico City: A Drug Utilization StudyDocument6 pagesPrescription Patterns of Antihypertensives in A Community Health Centre in Mexico City: A Drug Utilization StudyWendy Garduño SandovalNo ratings yet
- Predicting Adherence To Antiretroviral Therapy Among Pregnant Women in Guyana: Utility of The Health Belief ModelDocument10 pagesPredicting Adherence To Antiretroviral Therapy Among Pregnant Women in Guyana: Utility of The Health Belief ModelRiska Resty WasitaNo ratings yet
- EfrgergDocument10 pagesEfrgerglionfairwayNo ratings yet
- Research ArticleDocument6 pagesResearch ArticlesirawNo ratings yet
- Nejm ECA Data MonitoringDocument7 pagesNejm ECA Data MonitoringEdward ChavezNo ratings yet
- Mobile Health Technology For Atrial Fibrillation Management Integrating Decision Support, Education, and Patient Involvement: mAF App TrialDocument15 pagesMobile Health Technology For Atrial Fibrillation Management Integrating Decision Support, Education, and Patient Involvement: mAF App TrialPsycolo techNo ratings yet
- Users' Guides To The Medical Literature XIVDocument5 pagesUsers' Guides To The Medical Literature XIVFernandoFelixHernandezNo ratings yet
- Management of Fungal Infections in MCS and Cardiothoracic Organ Transplant Recipients: ISHLT Monograph Series (Volume 12)From EverandManagement of Fungal Infections in MCS and Cardiothoracic Organ Transplant Recipients: ISHLT Monograph Series (Volume 12)No ratings yet
- 3225 Adc 8713 eDocument34 pages3225 Adc 8713 eJuan Carlos Carbajal SilvaNo ratings yet
- Stress Ulcer, Gastritis, and Gastrointestinal Bleeding Prophylaxis in Critically Ill Pediatric Patients: A Systematic ReviewDocument9 pagesStress Ulcer, Gastritis, and Gastrointestinal Bleeding Prophylaxis in Critically Ill Pediatric Patients: A Systematic ReviewIkrima MuhdarmuhallyNo ratings yet
- 1 s2.0 S2452301116300700 Main 1Document11 pages1 s2.0 S2452301116300700 Main 1uiolNo ratings yet
- Right Care 2: SeriesDocument9 pagesRight Care 2: SeriesVirgilioNo ratings yet
- 17 Salluh Damluji DeliriumICU BMJ2015Document11 pages17 Salluh Damluji DeliriumICU BMJ2015DIANA CAROLINA OTALORA ALVAREZNo ratings yet
- JHH 20168Document8 pagesJHH 20168Anonymous bgcWQhRNo ratings yet
- PIIS2213260017304745Document10 pagesPIIS2213260017304745Juan Pablo CasanovaNo ratings yet
- The Clinical Outcomes and Predictive Factors For.24Document5 pagesThe Clinical Outcomes and Predictive Factors For.24KeziaNo ratings yet
- Nonpharmacological Interventions To Prevent DeliriumDocument12 pagesNonpharmacological Interventions To Prevent Deliriumjuan.pablo.castroNo ratings yet
- Hepatocellular Carcinoma: Translational Precision Medicine ApproachesFrom EverandHepatocellular Carcinoma: Translational Precision Medicine ApproachesYujin HoshidaNo ratings yet
- Plot No.7G, Ground Floor, Opp. Graphite India, Telerad RXDX Healthcare PVT LTDDocument4 pagesPlot No.7G, Ground Floor, Opp. Graphite India, Telerad RXDX Healthcare PVT LTDSanjay TripathiNo ratings yet
- Breast Cancer JournalDocument14 pagesBreast Cancer JournalYASSER ALATAWINo ratings yet
- Ccu Deparmental Operation PoliciesDocument7 pagesCcu Deparmental Operation PoliciesamalfarhanaNo ratings yet
- 'OET' SAMPLE READING NEW DR TANJIM OVEE 2020Document19 pages'OET' SAMPLE READING NEW DR TANJIM OVEE 2020AHMED TANJIMUL ISLAMNo ratings yet
- 8111 BDFFF 977 F 7 F 96612Document1 page8111 BDFFF 977 F 7 F 96612api-660790181No ratings yet
- Stillbirth Series OverviewDocument38 pagesStillbirth Series OverviewZaroon AhmedNo ratings yet
- 1 Introduction TraumaDocument14 pages1 Introduction TraumameirizameilyaniarmanNo ratings yet
- Eksistensi Pengobatan Tradisional Di Tellusiattinge: Andi Erwin AdiwijayaDocument9 pagesEksistensi Pengobatan Tradisional Di Tellusiattinge: Andi Erwin Adiwijayaala bariklanaNo ratings yet
- 201-300 Beded District Hospitals - MCIDocument97 pages201-300 Beded District Hospitals - MCIAaquib Mahfuz50% (2)
- Behavioral AssessmentDocument14 pagesBehavioral AssessmentGM TanNo ratings yet
- QUESTION # 1: Analyze Why Is It Important For Health Care Managers and Policy-Makers To Understand The Intricacies of The Health Care Delivery SystemDocument5 pagesQUESTION # 1: Analyze Why Is It Important For Health Care Managers and Policy-Makers To Understand The Intricacies of The Health Care Delivery SystemLenie ManayamNo ratings yet
- Ghana CNTDocument155 pagesGhana CNTRoy VermaNo ratings yet
- Orca Share Media1504048233006Document30 pagesOrca Share Media1504048233006Marietta O. GermanNo ratings yet
- DR Jay Davidson How Invisible Radiation Exposure Robs Your EnergyDocument6 pagesDR Jay Davidson How Invisible Radiation Exposure Robs Your EnergySkyla ReadNo ratings yet
- Case Study 2 NCPDocument1 pageCase Study 2 NCPJayson SamonteNo ratings yet
- Letter - State Employee Health BenefitsDocument2 pagesLetter - State Employee Health BenefitsWHYY NewsNo ratings yet
- Maklumat Vaksinasi: Vaccination DetailsDocument2 pagesMaklumat Vaksinasi: Vaccination DetailsCahaya MawaddahNo ratings yet
- German S3 Guidelines: Anal Abscess and Fistula (Second Revised Version)Document55 pagesGerman S3 Guidelines: Anal Abscess and Fistula (Second Revised Version)Bunga AmiliaNo ratings yet
- Water Material Safety Data Sheet: 1. ProductDocument7 pagesWater Material Safety Data Sheet: 1. ProductTeererai KaguraNo ratings yet
- 18 IAT StudentGuideDocument8 pages18 IAT StudentGuideDenySidiqMulyonoChtNo ratings yet
- Group 7 AssignmentDocument24 pagesGroup 7 AssignmentchangNo ratings yet
- 4 Effective Exercises For Bedridden Patients - Advanced TissueDocument4 pages4 Effective Exercises For Bedridden Patients - Advanced TissuevaishnaviNo ratings yet
- Menopause and HRT CounsellingDocument4 pagesMenopause and HRT CounsellingannagubbinsNo ratings yet
- Munchausen SyndromeDocument10 pagesMunchausen SyndromeGita PuspitasariNo ratings yet
- Preparing Chapter 8Document35 pagesPreparing Chapter 8Hawraa ShaalanNo ratings yet
- Work Stress Management Among Bank EmployeesDocument62 pagesWork Stress Management Among Bank EmployeesPrajjwal KanojiyaNo ratings yet
- Reasons Against Legalizing MarijuanaDocument1 pageReasons Against Legalizing MarijuanaJoana TrinidadNo ratings yet
- Rcpi Diploma in Dermatology BrochureDocument4 pagesRcpi Diploma in Dermatology BrochureNabila BaharNo ratings yet