You might also like
- Management of Fungal Infections in MCS and Cardiothoracic Organ Transplant Recipients: ISHLT Monograph Series (Volume 12)From EverandManagement of Fungal Infections in MCS and Cardiothoracic Organ Transplant Recipients: ISHLT Monograph Series (Volume 12)No ratings yet
- Association Between The Choice of IV Crystalloid and In-Hospital Mortality Among Critically Ill Adults With SepsisDocument7 pagesAssociation Between The Choice of IV Crystalloid and In-Hospital Mortality Among Critically Ill Adults With SepsisbernardoNo ratings yet
- Tsuyuki 2002Document7 pagesTsuyuki 2002Basilharbi HammadNo ratings yet
- Medication Adherence and Blood Pressure Control Among Hypertensive Patients With Coexisting Long-Term Conditions in Primary Care SettingsDocument10 pagesMedication Adherence and Blood Pressure Control Among Hypertensive Patients With Coexisting Long-Term Conditions in Primary Care SettingsmadhurocksktmNo ratings yet
- Digital Commons@Becker Digital Commons@BeckerDocument15 pagesDigital Commons@Becker Digital Commons@Beckerre septian IlhamsyahNo ratings yet
- Milrinone As Compared With Dobutamine in The Treatment of Cardiogenic ShockDocument10 pagesMilrinone As Compared With Dobutamine in The Treatment of Cardiogenic ShockCarlos Alberto Holguin PalaciosNo ratings yet
- Artigo 2Document13 pagesArtigo 2Paulo TononNo ratings yet
- New England Journal Medicine: The ofDocument14 pagesNew England Journal Medicine: The ofFajar PramaduNo ratings yet
- PIONEERstudy 2016Document12 pagesPIONEERstudy 2016Jose Enrique Valecillos MorenoNo ratings yet
- DM 2Document8 pagesDM 2Roberto AlexiNo ratings yet
- 2009hetrase CCMDocument12 pages2009hetrase CCMgiseladelarosa2006No ratings yet
- New England Journal Medicine: The ofDocument14 pagesNew England Journal Medicine: The ofIMNo ratings yet
- J Jacc 2022 11 005Document11 pagesJ Jacc 2022 11 005MadeNo ratings yet
- Milri Vs DobutaDocument10 pagesMilri Vs DobutaEliana Lopez BaronNo ratings yet
- Nejmoa 2026141Document14 pagesNejmoa 2026141Matheus FelipeNo ratings yet
- Fphar 13 946415Document11 pagesFphar 13 946415Yulian 53No ratings yet
- 10.1016@S0140 67361932317 7Document11 pages10.1016@S0140 67361932317 7DaviSalmissonNo ratings yet
- JHH 20168Document8 pagesJHH 20168Anonymous bgcWQhRNo ratings yet
- LeaderDocument12 pagesLeaderMoeez AkramNo ratings yet
- Nihms866890 UPLOAD 3Document21 pagesNihms866890 UPLOAD 3Peter GardinerNo ratings yet
- Healthcare SpendingDocument20 pagesHealthcare Spendingmikeb92556No ratings yet
- Jama Janiaud 2021 Oi 210019 1614276859.07656Document11 pagesJama Janiaud 2021 Oi 210019 1614276859.07656JulioRobertoHernandezJuarezNo ratings yet
- Jurnal RhinoDocument7 pagesJurnal RhinoElvienNo ratings yet
- Nej Mo A 2208415Document11 pagesNej Mo A 2208415Nelson Da VegaNo ratings yet
- Epidemiology of Resistant Hypertension in Canada - 2Document7 pagesEpidemiology of Resistant Hypertension in Canada - 2ehaffejeeNo ratings yet
- Management Arteriosclerosis and ClaudicationDocument41 pagesManagement Arteriosclerosis and ClaudicationLuqman AlwiNo ratings yet
- 2005 Whitcomb CDM Hyperglycemia ICUDocument6 pages2005 Whitcomb CDM Hyperglycemia ICUHema ThiyaguNo ratings yet
- 793 FullDocument9 pages793 FullDENNYNo ratings yet
- PrincipalDocument8 pagesPrincipalNorlando RuizNo ratings yet
- Sprint HtaDocument10 pagesSprint HtaMedicina CUENo ratings yet
- Diabetes TratamientoDocument16 pagesDiabetes TratamientoCamilita BrolloNo ratings yet
- ADHD Medications and Risk of Serious Cardiovascular Events in Young and Middle-Aged AdultsDocument11 pagesADHD Medications and Risk of Serious Cardiovascular Events in Young and Middle-Aged AdultsGary KatzNo ratings yet
- Vitamin DDocument12 pagesVitamin DLia NadaNo ratings yet
- Ioi70171 2461 2468Document8 pagesIoi70171 2461 2468jimmyneutron1337No ratings yet
- Ada Cvd-Renalcompendium Fin-WebDocument32 pagesAda Cvd-Renalcompendium Fin-WebJoseph Antonio Apaza GómezNo ratings yet
- Stress Reduction in The Secondary Prevention of Cardiovascular DiseaseDocument10 pagesStress Reduction in The Secondary Prevention of Cardiovascular DiseaseNeilermindNo ratings yet
- Antipyretic Therapy in Critically Ill Septic Patients - A Systematic Review and Meta-AnalysisDocument8 pagesAntipyretic Therapy in Critically Ill Septic Patients - A Systematic Review and Meta-AnalysisKrutarth PatelNo ratings yet
- Perka - Uji BE - Draf 6 Nov 2017Document11 pagesPerka - Uji BE - Draf 6 Nov 2017Rizqi AdistraNo ratings yet
- Dietary in Ammatory Potential and Risk of Cardiovascular Disease Among Men and Women in The U.SDocument13 pagesDietary in Ammatory Potential and Risk of Cardiovascular Disease Among Men and Women in The U.SRoxana CristeaNo ratings yet
- Antihypertensive Drug Class Interactions and Risk For Incident Diabetes: A Nested Case - Control StudyDocument9 pagesAntihypertensive Drug Class Interactions and Risk For Incident Diabetes: A Nested Case - Control StudylalaNo ratings yet
- Fluido Therapy - Sepsis Jama Zampieri 2023 RV 230010 1686240954.61353Document14 pagesFluido Therapy - Sepsis Jama Zampieri 2023 RV 230010 1686240954.61353VictorMéndezNo ratings yet
- CourageDocument14 pagesCourageSuryaNo ratings yet
- White NEJM Examine Sep13Document9 pagesWhite NEJM Examine Sep13Kamalia LayalNo ratings yet
- White NEJM Examine Sep13Document9 pagesWhite NEJM Examine Sep13Kamalia LayalNo ratings yet
- 10 1001@jama 2020 10044Document11 pages10 1001@jama 2020 10044Rodrigo Ehécatl Torres NevárezNo ratings yet
- Genética Clínica 2Document10 pagesGenética Clínica 2Victor MarquesNo ratings yet
- 2008-Predictive Validity of A Medication Adherence Measure in An Outpatient Setting PDFDocument7 pages2008-Predictive Validity of A Medication Adherence Measure in An Outpatient Setting PDFRizki RomadhonNo ratings yet
- Pci On Infark MyocardDocument10 pagesPci On Infark MyocardDinny Novia WNo ratings yet
- 1 s2.0 S1053077021008405 MainDocument13 pages1 s2.0 S1053077021008405 Maindiogofc123No ratings yet
- Journal Pmed 1003501Document28 pagesJournal Pmed 1003501Abi HinojosaNo ratings yet
- Proton Pump Inhibitor Use and The Risk of Chronic Kidney DiseaseDocument9 pagesProton Pump Inhibitor Use and The Risk of Chronic Kidney DiseaseDita IndahNo ratings yet
- Testing For Primary Hyperaldosteronism and MRA TX Annals 2020Document10 pagesTesting For Primary Hyperaldosteronism and MRA TX Annals 2020Miri PravdaNo ratings yet
- On MedDocument10 pagesOn MedShimily LiangNo ratings yet
- Genetic Risk, Adherence To A Healthy Lifestyle, and Coronary DiseaseDocument10 pagesGenetic Risk, Adherence To A Healthy Lifestyle, and Coronary DiseaseNurul Falah KalokoNo ratings yet
- DM - JamaDocument8 pagesDM - JamaMalisa LukmanNo ratings yet
- Blood Pressure Lowering and Risk of New Type 2 DiabetesDocument8 pagesBlood Pressure Lowering and Risk of New Type 2 DiabetesFanny Isabel Rubio CampaNo ratings yet
- #1 - Jurnal Terapi Komplementer Untuk Penyakit JantungDocument13 pages#1 - Jurnal Terapi Komplementer Untuk Penyakit Jantungshella1selinaNo ratings yet
- Efficacy and Safety of Chinese Herbal Medicine Xiao Yao San in 2019 PhytomeDocument13 pagesEfficacy and Safety of Chinese Herbal Medicine Xiao Yao San in 2019 PhytomeJamila IthaiaNo ratings yet
- VasculitisDocument12 pagesVasculitisMaite OrellanaNo ratings yet
- Lixisenatide in Patients With Type 2 Diabetes and Acute Coronary SyndromeDocument11 pagesLixisenatide in Patients With Type 2 Diabetes and Acute Coronary SyndromeAndi Soraya PurnamandaNo ratings yet
- SK716 Pengintegrasian Mekanisme Nilai Karbon (English)Document13 pagesSK716 Pengintegrasian Mekanisme Nilai Karbon (English)Isti HanifahNo ratings yet
- Experiment# 3 Projectile Motion (Tasks 3 and 4)Document18 pagesExperiment# 3 Projectile Motion (Tasks 3 and 4)Hafiz MuhammadNo ratings yet
- Mohair FiberDocument33 pagesMohair FiberMuhammad Ahsan AftabNo ratings yet
- Deks Olje ArticleDocument5 pagesDeks Olje ArticleTomMacNaughtonNo ratings yet
- Unit 4 Early HumansDocument8 pagesUnit 4 Early HumansSepfira ReztikaNo ratings yet
- Tables in National Plumbing CodeDocument4 pagesTables in National Plumbing CodeMartin GragasinNo ratings yet
- Mobile Network Optimization MapDocument1 pageMobile Network Optimization MapShahzad Farooq100% (1)
- Recycle ProgramDocument2 pagesRecycle ProgramKaps BlazeNo ratings yet
- Fire and Blast in The Future OffshoreDocument45 pagesFire and Blast in The Future OffshoredrgNo ratings yet
- General Biology 1: Go Fast, or Slow Down?Document23 pagesGeneral Biology 1: Go Fast, or Slow Down?Mikhael OiraNo ratings yet
- Treatment of Headaches in The ED With Lower Cervical Intramuscular Bupivacaine Injections: A 1-Year Retrospective Review of 417 PatientsDocument9 pagesTreatment of Headaches in The ED With Lower Cervical Intramuscular Bupivacaine Injections: A 1-Year Retrospective Review of 417 PatientsLarry B. Mellick, MDNo ratings yet
- A Review: HPLC Method Development and Validation: November 2015Document7 pagesA Review: HPLC Method Development and Validation: November 2015R Abdillah AkbarNo ratings yet
- Circuit Diagram:: Experiment No: 3 Title: Characteristics of Filament Lamp ObjectivesDocument2 pagesCircuit Diagram:: Experiment No: 3 Title: Characteristics of Filament Lamp ObjectivesAsrar Hussain BhatNo ratings yet
- General ALT Model For Step Stress TestDocument12 pagesGeneral ALT Model For Step Stress TestAnshul NautiyalNo ratings yet
- Midwifery All Year ProgramDocument3 pagesMidwifery All Year Programfiraol mokonnenNo ratings yet
- Fs 1100 Flame Simulator Data Sheet en Us 584524Document4 pagesFs 1100 Flame Simulator Data Sheet en Us 584524Rildon Valqui CiezaNo ratings yet
- Mitsubishi Motors: Service ManualDocument29 pagesMitsubishi Motors: Service ManualCristobalNo ratings yet
- CaseStudy AmtrakDocument14 pagesCaseStudy Amtraksnob_kNo ratings yet
- CHS-WWW - Polsteel. TUBOS METALICOS PDFDocument3 pagesCHS-WWW - Polsteel. TUBOS METALICOS PDFEduardo TorreNo ratings yet
- HydrotherapyDocument52 pagesHydrotherapyMpt Sports100% (1)
- Saej401v002 PDFDocument6 pagesSaej401v002 PDFLuis LujanoNo ratings yet
- Memories of HomeDocument14 pagesMemories of HomeMary Francis Edmer SayconNo ratings yet
- Shock Classification and PathophysiologyDocument40 pagesShock Classification and PathophysiologyErick Anca100% (2)
- Detailed Lesson Plan in General MathematicsDocument6 pagesDetailed Lesson Plan in General MathematicsAira Jane Irarum78% (18)
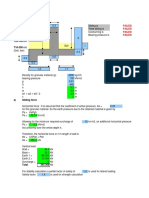
- Sliding, Overturning, Bearing Pressure and Bending Reinforcement Calculations for Retaining WallDocument4 pagesSliding, Overturning, Bearing Pressure and Bending Reinforcement Calculations for Retaining WallAbdul Aziz Julkarnain ZulkifliNo ratings yet
- z1875 Caton (BMJ) Electric Currents of The BrainDocument23 pagesz1875 Caton (BMJ) Electric Currents of The BrainUnholy VladNo ratings yet
- Lista de Precios Tones y Staleks 01.04Document3 pagesLista de Precios Tones y Staleks 01.04Maria T. OliverosNo ratings yet
- Simulation of bitumen upgrading processes modelling and optimisationDocument6 pagesSimulation of bitumen upgrading processes modelling and optimisationDonato MontroneNo ratings yet
- Cse Reviewer - MathDocument58 pagesCse Reviewer - MathLyne LerinNo ratings yet
- IGCSE Biology 4325 2H Mark SchemeDocument14 pagesIGCSE Biology 4325 2H Mark SchememuhajireenNo ratings yet
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (14)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 3.5 out of 5 stars3.5/5 (2)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 5 out of 5 stars5/5 (4)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 5 out of 5 stars5/5 (5)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsFrom EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo ratings yet
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (327)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 3.5 out of 5 stars3.5/5 (33)
- Daniel Kahneman's "Thinking Fast and Slow": A Macat AnalysisFrom EverandDaniel Kahneman's "Thinking Fast and Slow": A Macat AnalysisRating: 3.5 out of 5 stars3.5/5 (130)
- Summary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisFrom EverandSummary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisRating: 5 out of 5 stars5/5 (3)