You might also like
- Spinal Cord Injury: Presented By: Feliciano, Jenard R. Flores, Arliah Q. Gaspar, Danica VDocument79 pagesSpinal Cord Injury: Presented By: Feliciano, Jenard R. Flores, Arliah Q. Gaspar, Danica VPam RomeroNo ratings yet
- Nursing AssessmentDocument16 pagesNursing AssessmentJihan Novita100% (1)
- Neurology MnemonicsDocument2 pagesNeurology MnemonicsJan Taplin100% (1)
- Med Surg NursingDocument9 pagesMed Surg NursingNaomi Myrick100% (1)
- Nefertiti Lift BotoxDocument9 pagesNefertiti Lift BotoxAnamaria Zaccolo100% (2)
- (Original PDF) Sensation and Perception 10th Edition by E. Bruce GoldsteinDocument42 pages(Original PDF) Sensation and Perception 10th Edition by E. Bruce Goldsteinlynn.vaughan84887% (45)
- The Thalamus 2022Document642 pagesThe Thalamus 2022Eduardo RodriguezNo ratings yet
- Integrated Science Grade 10 Weeks 1-5 - Term 3Document52 pagesIntegrated Science Grade 10 Weeks 1-5 - Term 3Daniel DowdingNo ratings yet
- Neuroimaging in Acute StrokeDocument23 pagesNeuroimaging in Acute StrokeSnezana Mihajlovic100% (1)
- DX Intracranial Pressure PDFDocument8 pagesDX Intracranial Pressure PDFSherree HayesNo ratings yet
- Procedure On Lumber PunctureDocument8 pagesProcedure On Lumber PunctureDimpal ChoudharyNo ratings yet
- Examination of NoseDocument63 pagesExamination of NoseDr Sravya M VNo ratings yet
- Truebp Clinical Information LeafletDocument9 pagesTruebp Clinical Information LeafletRespicare ServiceIT MikeNo ratings yet
- SynopsisDocument14 pagesSynopsisAqeel AhmadNo ratings yet
- HypovolaemicShock FullReport PDFDocument58 pagesHypovolaemicShock FullReport PDFSandara ParkNo ratings yet
- Wang 2017Document9 pagesWang 2017Jefferson891127No ratings yet
- CVP Final 2021Document11 pagesCVP Final 2021Ahmed AshrafNo ratings yet
- NCM 118L/ 119L (Related Learning Experience) Day 3-ActivityDocument4 pagesNCM 118L/ 119L (Related Learning Experience) Day 3-ActivityNicole Villanueva, BSN - Level 3ANo ratings yet
- CVP MonitoringDocument4 pagesCVP Monitoringسانو روديلNo ratings yet
- Dias2020 Article ValueOfComputerizedShuntInfusiDocument13 pagesDias2020 Article ValueOfComputerizedShuntInfusiDespina Aphroditi LalouNo ratings yet
- Programmed Postoperative Physiotherapy May Improve Functional Outcomes in Pneumonectomy Patients of Rare Causes Case SeriesDocument7 pagesProgrammed Postoperative Physiotherapy May Improve Functional Outcomes in Pneumonectomy Patients of Rare Causes Case SeriesAtu KaushalNo ratings yet
- "Nag Dugo Akong Gums Kaduha" AsDocument3 pages"Nag Dugo Akong Gums Kaduha" AsKuro HanabusaNo ratings yet
- Chapter 14: Nervous System Alterations Sole: Introduction To Critical Care Nursing, 7th EditionDocument16 pagesChapter 14: Nervous System Alterations Sole: Introduction To Critical Care Nursing, 7th Editionnana BediakoNo ratings yet
- 林奕廷 - perioperative management of TSSDocument15 pages林奕廷 - perioperative management of TSS林奕廷No ratings yet
- Meta-Analysis To Assess The Effectiveness of Topically Used Vancomycin in Reducing Sternal Wound Infections After Cardiac SurgeryDocument19 pagesMeta-Analysis To Assess The Effectiveness of Topically Used Vancomycin in Reducing Sternal Wound Infections After Cardiac SurgeryWildor Samir Cubas LlalleNo ratings yet
- Ripit 2022Document2 pagesRipit 2022Zoran BuchevNo ratings yet
- Fifteen Years Experience With Finger Arterial Pressure MonitoringDocument12 pagesFifteen Years Experience With Finger Arterial Pressure MonitoringLevente BalázsNo ratings yet
- Synopsis DR ABCDocument8 pagesSynopsis DR ABCFiaz medicoNo ratings yet
- 1510493354article pdf1389454199Document6 pages1510493354article pdf1389454199Yolanda FitrianiNo ratings yet
- Lumbar PunctureDocument16 pagesLumbar Punctureaarti chandeNo ratings yet
- Lumbar PunctureDocument4 pagesLumbar PunctureJeann sumbillaNo ratings yet
- Mechanical Ventilation and Noninvasive Ventilatory SupportDocument30 pagesMechanical Ventilation and Noninvasive Ventilatory Supportdr.baselnassarNo ratings yet
- Efficacy Lidocaine Endoscopic Submucosal DissectionDocument7 pagesEfficacy Lidocaine Endoscopic Submucosal DissectionAnonymous lSWQIQNo ratings yet
- PVD Prep U. Chapter 27Document5 pagesPVD Prep U. Chapter 27Monica JubaneNo ratings yet
- Effect of Early Physiotherapy in Coronary Artery Bypass Graft Surgery: A CaseDocument4 pagesEffect of Early Physiotherapy in Coronary Artery Bypass Graft Surgery: A CaseFitratun NajizahNo ratings yet
- Intrathecal Antibiotic Administration Procedure (Paediatrics)Document9 pagesIntrathecal Antibiotic Administration Procedure (Paediatrics)Abu Azzam Al-HadiNo ratings yet
- Bloodpressure 2Document4 pagesBloodpressure 2Yousuf Azhar AlamiaNo ratings yet
- Answers, Rationales, and Test Taking Strategies: 2, 3. The Nurse Should Determine If The CliDocument13 pagesAnswers, Rationales, and Test Taking Strategies: 2, 3. The Nurse Should Determine If The CliNursyNurseNo ratings yet
- Fifteen Years Experience With Finger Arterial Pressure MonitoringDocument12 pagesFifteen Years Experience With Finger Arterial Pressure MonitoringJorge FranciscoNo ratings yet
- Measurement of BPDocument6 pagesMeasurement of BPNiko DagunoNo ratings yet
- Tiers IcpDocument12 pagesTiers IcpjheyfteeNo ratings yet
- Comparison of Modified Borg Scale and Visual Analog Scale Dyspnea Scores in Predicting Re-Intervention After Drainage of Malignant Pleural EffusionDocument8 pagesComparison of Modified Borg Scale and Visual Analog Scale Dyspnea Scores in Predicting Re-Intervention After Drainage of Malignant Pleural EffusionMukhlis HasNo ratings yet
- Sepsis Nursing Management in Emergency Care: By: Diah Retno Wulan, S.Kep., NS., M.KepDocument23 pagesSepsis Nursing Management in Emergency Care: By: Diah Retno Wulan, S.Kep., NS., M.KepTia AFNo ratings yet
- Guidelines For The Management of Intracerebral HaemorrhageDocument18 pagesGuidelines For The Management of Intracerebral Haemorrhagerebeca marityNo ratings yet
- Cuidados Neuromuscular 2017Document12 pagesCuidados Neuromuscular 2017Tami SchumacherNo ratings yet
- Role of Ultrasonographic Inferior Venacaval Assessment in Surgeries Conducted Under General Anaesthesia-A Prospective Observational StudyDocument6 pagesRole of Ultrasonographic Inferior Venacaval Assessment in Surgeries Conducted Under General Anaesthesia-A Prospective Observational StudyIJAR JOURNALNo ratings yet
- Factibilidad Ecografia Ocular Anestesio Chilenos 2019Document5 pagesFactibilidad Ecografia Ocular Anestesio Chilenos 2019GabriellaNo ratings yet
- LiverpoolIntra-Hospital Transfer of ICU PatientsDocument8 pagesLiverpoolIntra-Hospital Transfer of ICU PatientsInnas DoankNo ratings yet
- Impact of Continuous Non-Invasive Blood Pressure Monitoring On Hemodynamic Fluctuation During General Anesthesia: A Randomized Controlled StudyDocument9 pagesImpact of Continuous Non-Invasive Blood Pressure Monitoring On Hemodynamic Fluctuation During General Anesthesia: A Randomized Controlled StudyShovie Thalia MirandaNo ratings yet
- 22 - Dengue Hemorrhagic FeverDocument7 pages22 - Dengue Hemorrhagic FeverMark Denver FranciscoNo ratings yet
- A 21 Year Old Female, 50 KG, Was Scheduled For Excision of Left Breast Mass. VS Are As Follows: BP 100/70, PR 75/min, RR 16/min, Temperature 37°CDocument4 pagesA 21 Year Old Female, 50 KG, Was Scheduled For Excision of Left Breast Mass. VS Are As Follows: BP 100/70, PR 75/min, RR 16/min, Temperature 37°CKat JolejoleNo ratings yet
- Journal Bedah SarafDocument4 pagesJournal Bedah SarafWisnuardhyHendrawardhanaNo ratings yet
- Laparoscopic Appendictomy DictationDocument3 pagesLaparoscopic Appendictomy DictationHassanNo ratings yet
- Surgical Management: SurgeryDocument5 pagesSurgical Management: SurgeryKarl Angelo MontanoNo ratings yet
- Welcome To All: Nursing StaffDocument67 pagesWelcome To All: Nursing StaffMukesh Choudhary JatNo ratings yet
- Dynamic Arterial Elastance To Predict Mean Arterial Pressure Decrease After Reduction of Vasopressor in Septic Shock PatientsDocument12 pagesDynamic Arterial Elastance To Predict Mean Arterial Pressure Decrease After Reduction of Vasopressor in Septic Shock PatientsAltair Monti TeslaNo ratings yet
- NCP 2 LRDR For PrintDocument2 pagesNCP 2 LRDR For PrintGeorge PandaNo ratings yet
- Carotid Sinus MassageDocument4 pagesCarotid Sinus MassageChalikias GeorgeNo ratings yet
- Paper 7, Corrado 2017Document8 pagesPaper 7, Corrado 2017NITIN SENTHILKUMARNo ratings yet
- Effect of Bladder Volume On Measured Intravesical Pressure: A Prospective Cohort StudyDocument6 pagesEffect of Bladder Volume On Measured Intravesical Pressure: A Prospective Cohort StudyJimmy Israel Rodríguez LópezNo ratings yet
- Case Stduy Med SurgDocument5 pagesCase Stduy Med SurgKevean Kimi LimNo ratings yet
- 10 Signos of VitalidadDocument7 pages10 Signos of VitalidadKarenNo ratings yet
- Effect of Intraoperative Dexmedetomidine On Post-Craniotomy PainDocument9 pagesEffect of Intraoperative Dexmedetomidine On Post-Craniotomy PainIva SantikaNo ratings yet
- TMP BF26Document4 pagesTMP BF26FrontiersNo ratings yet
- Acute/Critically Ill Patients in Hemodynamic Monitoring (Management)Document8 pagesAcute/Critically Ill Patients in Hemodynamic Monitoring (Management)Esmareldah Henry SirueNo ratings yet
- Implementing Ambulatory Blood Pressure Monitoring in Primary Care PracticeDocument7 pagesImplementing Ambulatory Blood Pressure Monitoring in Primary Care PracticeBrianNo ratings yet
- Patient Blood Management in Cardiac SurgeryFrom EverandPatient Blood Management in Cardiac SurgeryChristian von HeymannNo ratings yet
- 2022 - Epidemiologia - Sifilis VIH en Homosexuales HombresDocument25 pages2022 - Epidemiologia - Sifilis VIH en Homosexuales HombresEduardo RodriguezNo ratings yet
- 2021 - 07 - Encefalitis Autoinmune Post Vacuna SarsCov2Document3 pages2021 - 07 - Encefalitis Autoinmune Post Vacuna SarsCov2Eduardo RodriguezNo ratings yet
- 1 s2.0 S1341321X18304598 MainDocument3 pages1 s2.0 S1341321X18304598 MainEduardo RodriguezNo ratings yet
- Visual Function Classification System For Children With Cerebral Palsy - Development and Validation - Enhanced ReaderDocument8 pagesVisual Function Classification System For Children With Cerebral Palsy - Development and Validation - Enhanced ReaderEduardo RodriguezNo ratings yet
- 2017 - 12 - Encefalitis AutoinmuneDocument4 pages2017 - 12 - Encefalitis AutoinmuneEduardo RodriguezNo ratings yet
- Manual Ability Classification System For Children With Cerebral Palsy 4-18 YearsDocument2 pagesManual Ability Classification System For Children With Cerebral Palsy 4-18 YearsEduardo RodriguezNo ratings yet
- Dimauro 2017Document8 pagesDimauro 2017Eduardo RodriguezNo ratings yet
- Spondylodiscitis Severity Code: Scoring System For The Classification and Treatment of Non-Specific SpondylodiscitisDocument9 pagesSpondylodiscitis Severity Code: Scoring System For The Classification and Treatment of Non-Specific SpondylodiscitisEduardo RodriguezNo ratings yet
- Early, Accurate Diagnosis and Early Intervention in Cerebral Palsy: Advances in Diagnosis and TreatmentDocument12 pagesEarly, Accurate Diagnosis and Early Intervention in Cerebral Palsy: Advances in Diagnosis and TreatmentEduardo RodriguezNo ratings yet
- CP Terminology 2 Final Jun21Document2 pagesCP Terminology 2 Final Jun21Eduardo RodriguezNo ratings yet
- Chaturvedi 2013Document93 pagesChaturvedi 2013Eduardo RodriguezNo ratings yet
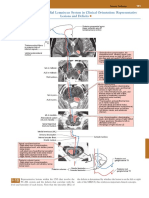
- Posterior Column-Medial Lemniscus System in Clinical Orientation: Representative Lesions and DeficitsDocument1 pagePosterior Column-Medial Lemniscus System in Clinical Orientation: Representative Lesions and DeficitsEduardo RodriguezNo ratings yet
- 2019 - Rol de La MITOCONDRIA Y PARKINSONDocument92 pages2019 - Rol de La MITOCONDRIA Y PARKINSONEduardo RodriguezNo ratings yet
- Historia de La NeurosonologiaDocument9 pagesHistoria de La NeurosonologiaEduardo RodriguezNo ratings yet
- 2018 - Rol de La MITOCONDRIA y HUNTINGTONDocument25 pages2018 - Rol de La MITOCONDRIA y HUNTINGTONEduardo RodriguezNo ratings yet
- Educación Medica en El PerûDocument6 pagesEducación Medica en El PerûEduardo RodriguezNo ratings yet
- Pioneos en NeurosonologiaDocument21 pagesPioneos en NeurosonologiaEduardo RodriguezNo ratings yet
- Artículo Seminario IVDocument22 pagesArtículo Seminario IVEduardo RodriguezNo ratings yet
- Iq AdolecenteDocument13 pagesIq AdolecenteEduardo RodriguezNo ratings yet
- Al-Sharify 2020 IOP Conf. Ser. Mater. Sci. Eng. 870 0120431Document11 pagesAl-Sharify 2020 IOP Conf. Ser. Mater. Sci. Eng. 870 0120431Hua Hidari YangNo ratings yet
- Transcranial Ultrasound Doppler Parameters in CereDocument7 pagesTranscranial Ultrasound Doppler Parameters in CereImin BuntaraNo ratings yet
- Mechanisms and Predisposing Factors For Sleep-Related Breathing Disorders in Children - UpToDateDocument30 pagesMechanisms and Predisposing Factors For Sleep-Related Breathing Disorders in Children - UpToDateTran Trang AnhNo ratings yet
- 23 Inguinofemoral, Iliac-Obturator, and Popliteal Lymphadenectomy For MelanomaDocument19 pages23 Inguinofemoral, Iliac-Obturator, and Popliteal Lymphadenectomy For MelanomajuanrangoneNo ratings yet
- Bio Class Xi Investigatory Project 2022Document16 pagesBio Class Xi Investigatory Project 2022SUSHNo ratings yet
- IP - 33 - 2020 - 8 Vol. 11 Issue 7 July 2020 IJPSR RE 3445Document15 pagesIP - 33 - 2020 - 8 Vol. 11 Issue 7 July 2020 IJPSR RE 3445OKANNo ratings yet
- 18.fibrinolytic (Thrombolytic) AgentsDocument42 pages18.fibrinolytic (Thrombolytic) AgentsAstha ShresthaNo ratings yet
- Sexual Reproduction in Humans: Chapter - I Reproduction SystemsDocument18 pagesSexual Reproduction in Humans: Chapter - I Reproduction Systemsrajendra110778No ratings yet
- KarthikeyanDocument110 pagesKarthikeyanHogea TimurNo ratings yet
- UNIT 1 Sleep & Rest-PatternDocument57 pagesUNIT 1 Sleep & Rest-Patternab tubeNo ratings yet
- Glaucoma: Direct Mechanical Theory - Suggests That HighDocument4 pagesGlaucoma: Direct Mechanical Theory - Suggests That HighMarissa AsimNo ratings yet
- Maxilary Sinus Graft ArunDocument181 pagesMaxilary Sinus Graft ArunJose Fernando Fragozo MendozaNo ratings yet
- M2 SURGERY - Liver - Dr. BaldovinoDocument30 pagesM2 SURGERY - Liver - Dr. Baldovinoqsd clinicNo ratings yet
- Unit 2 Study Guide Revised Jan 2018Document2 pagesUnit 2 Study Guide Revised Jan 2018Meghan PhillipsNo ratings yet
- Retinaldetachmentnew WORSDocument51 pagesRetinaldetachmentnew WORSMuthulakshmiNo ratings yet
- Astrocyte: Structure & FunctionDocument7 pagesAstrocyte: Structure & Functionمحمود الموسويNo ratings yet
- Dav Public School, Safilguda Subject-Science Worksheet Class-V/ Lesson-1 My BodyDocument3 pagesDav Public School, Safilguda Subject-Science Worksheet Class-V/ Lesson-1 My BodySanghamitra Biswa Dudul100% (2)
- Chapter 5 IntegumentaryDocument5 pagesChapter 5 IntegumentaryrenjiniNo ratings yet
- Aryan HatwarDocument15 pagesAryan HatwarAryan HatwarNo ratings yet
- Autismo y AutoinmunidadDocument50 pagesAutismo y AutoinmunidadPsicoterapia InfantilNo ratings yet
- Surgical Ii Case StudyDocument9 pagesSurgical Ii Case StudyRomuel PaparonNo ratings yet
- Space Infection - Theory ClassDocument264 pagesSpace Infection - Theory ClassMelese AbebeNo ratings yet
- ACVR and ECVDI Consensus Statement For The Standardization of The AbdominalDocument14 pagesACVR and ECVDI Consensus Statement For The Standardization of The AbdominalErick RamosNo ratings yet