You might also like
- 50 Landmark Papers in OmfsDocument313 pages50 Landmark Papers in OmfsNidhi Pandey67% (3)
- Livsey 2003Document6 pagesLivsey 2003Migue PerezNo ratings yet
- Yip Et Al 2015Document7 pagesYip Et Al 2015KasmiliawatyNo ratings yet
- 10b. Diagnosis Journal Review - Colorectal Cancer Screening NEJMDocument11 pages10b. Diagnosis Journal Review - Colorectal Cancer Screening NEJMPPDSNeurologiAgustus 2021No ratings yet
- Ijbs 24374Document8 pagesIjbs 24374Putri Tamara DasantosNo ratings yet
- Review: Ultrasound-Guided Percutaneous Core Needle Biopsy For The Diagnosis of Pancreatic DiseaseDocument10 pagesReview: Ultrasound-Guided Percutaneous Core Needle Biopsy For The Diagnosis of Pancreatic DiseaseElizabeth KezdamNo ratings yet
- Kapoor SchwannomaDocument7 pagesKapoor SchwannomaAna Clara Nunes SartoriNo ratings yet
- Nihms 472968Document14 pagesNihms 472968Charles MarloweNo ratings yet
- Original ArticleDocument7 pagesOriginal ArticleDain 2IronfootNo ratings yet
- Radiomics Analysis For The Prediction of Locoregional Recurrence of Locally Advanced Oropharyngeal Cancer and Hypopharyngeal CancerDocument9 pagesRadiomics Analysis For The Prediction of Locoregional Recurrence of Locally Advanced Oropharyngeal Cancer and Hypopharyngeal CancermeghrajpurkayasthaNo ratings yet
- Research: ArticleDocument4 pagesResearch: ArticleMuthu KumarNo ratings yet
- Hilton - Acquisition of Metastatic Tissue From Patients With Bone Metastases From Breast CancerDocument5 pagesHilton - Acquisition of Metastatic Tissue From Patients With Bone Metastases From Breast CancerOncology FatmawatiNo ratings yet
- 2021 PerincheriDocument8 pages2021 PerincheriRaluca-Maria SălcudeanNo ratings yet
- 1Document20 pages1aaasim93No ratings yet
- Rads - Usg - Breast Bi-RadsDocument3 pagesRads - Usg - Breast Bi-RadspriyaNo ratings yet
- Prognostic Significance of PINCH Signalling in Human Pancreatic Ductal AdenocarcinomaDocument7 pagesPrognostic Significance of PINCH Signalling in Human Pancreatic Ductal AdenocarcinomaLuis FuentesNo ratings yet
- Niar Tiroid UnlockedDocument11 pagesNiar Tiroid UnlockedNiarNo ratings yet
- Medi 95 E4797Document5 pagesMedi 95 E4797tika apriliaNo ratings yet
- Kim 2015Document9 pagesKim 2015Ke XuNo ratings yet
- 11 Preoperative - High - Neutrophil-Lymphocyte - Ratio - MayDocument8 pages11 Preoperative - High - Neutrophil-Lymphocyte - Ratio - MayBridia BogarNo ratings yet
- Clinical and Research Applications of A Brain Tumor Tissue Bank in The Age of Precision MedicineDocument12 pagesClinical and Research Applications of A Brain Tumor Tissue Bank in The Age of Precision MedicineSandra Milena Sanabria BarreraNo ratings yet
- Ni Hms 519602Document21 pagesNi Hms 519602Nur Rissa MaharanyNo ratings yet
- Ou 2016Document8 pagesOu 2016tami widiatul azahraNo ratings yet
- Thyroid Nodules Diagnostic Evaluation Based OnDocument20 pagesThyroid Nodules Diagnostic Evaluation Based Ondiaspalma.medNo ratings yet
- Research Article: The Bethesda System For Reporting Thyroid Cytopathology: A Cytohistological StudyDocument8 pagesResearch Article: The Bethesda System For Reporting Thyroid Cytopathology: A Cytohistological StudyAbdullah KhalilNo ratings yet
- 655506v1 Full PDFDocument36 pages655506v1 Full PDFgarrobosNo ratings yet
- Favorable Female NPCDocument6 pagesFavorable Female NPChi-lineNo ratings yet
- The Addition of Paclitaxel To Doxorubicin and Cisplatin and Cispalatin Volume Directed RadiationDocument21 pagesThe Addition of Paclitaxel To Doxorubicin and Cisplatin and Cispalatin Volume Directed RadiationGarsa GarnolNo ratings yet
- TIRADS2017Document9 pagesTIRADS2017Eliana RuizNo ratings yet
- Colen 2017Document7 pagesColen 2017yalocim666No ratings yet
- Ye 2013Document12 pagesYe 2013Mimsy Quiñones TafurNo ratings yet
- Impact of Extent of Lymphadenectomy On Survival After Radical Prostatectomy For Prostate CancerDocument5 pagesImpact of Extent of Lymphadenectomy On Survival After Radical Prostatectomy For Prostate CancerVinko GrubišićNo ratings yet
- Decision Making for Thyroid Nodule Diagnosis and ManagementDocument15 pagesDecision Making for Thyroid Nodule Diagnosis and ManagementFadi Al HajjiNo ratings yet
- 10.1016@s2468 12531930383 8 PDFDocument12 pages10.1016@s2468 12531930383 8 PDFShubham KeshriNo ratings yet
- Abstracts: Annals of OncologyDocument1 pageAbstracts: Annals of OncologyAsaikkutti AnnamalaiNo ratings yet
- VIP Fang and Shi 2019 Arch Pathol 2019Document11 pagesVIP Fang and Shi 2019 Arch Pathol 2019Jemma ArakelyanNo ratings yet
- Psa Persistentemente Elevado Post P RadicalDocument20 pagesPsa Persistentemente Elevado Post P RadicalBenjamin HuamanchauNo ratings yet
- Ayala2008 Cancer-Related Axonogenesis and Neurogenesis in Prostate CancerDocument11 pagesAyala2008 Cancer-Related Axonogenesis and Neurogenesis in Prostate CancerMariann DuzzNo ratings yet
- RRP Radical ProstatectomyDocument6 pagesRRP Radical ProstatectomybojanvuckovicNo ratings yet
- Atelektasis ParuDocument9 pagesAtelektasis ParuGigih PrakosoNo ratings yet
- Comparison of Serum Microseminoprotein-Beta (MSMB) With Total Prostate Specific Antigen (TPSA) in The Diagnosis of Prostate Cancer in African MenDocument7 pagesComparison of Serum Microseminoprotein-Beta (MSMB) With Total Prostate Specific Antigen (TPSA) in The Diagnosis of Prostate Cancer in African MenInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- ClinicalCharacteristicsAndProgrognostic AstrocytomaDocument12 pagesClinicalCharacteristicsAndProgrognostic AstrocytomaDesty PurnamasariNo ratings yet
- Precision Molecular Pathology of Prostate CancerFrom EverandPrecision Molecular Pathology of Prostate CancerBrian D. RobinsonNo ratings yet
- Research Article Prostatic Acid Phosphatase (PAP) Predicts Prostate Cancer Progress in A Population-Based Study: The Renewal of PAP?Document10 pagesResearch Article Prostatic Acid Phosphatase (PAP) Predicts Prostate Cancer Progress in A Population-Based Study: The Renewal of PAP?Jackkahuna LagunaNo ratings yet
- Tratamiento Esofago Cervical Lu, 2021Document9 pagesTratamiento Esofago Cervical Lu, 2021Carlos N. Rojas PuyolNo ratings yet
- Clinical Practice GuidelinesDocument3 pagesClinical Practice GuidelinesGd SuarantaNo ratings yet
- TheprostatepaperDocument12 pagesTheprostatepapermarlonkoesenNo ratings yet
- Prognostic Value of Immunohistochemistry-Based Subtyping Before and After Neoadjuvant Chemotherapy in Patients With Triple-Negative Breast CancerDocument9 pagesPrognostic Value of Immunohistochemistry-Based Subtyping Before and After Neoadjuvant Chemotherapy in Patients With Triple-Negative Breast Cancerwilliam.cardales03No ratings yet
- Tca 9 1453Document8 pagesTca 9 1453Pedro Gómez RNo ratings yet
- Cytogenetic Profile Predicts Prognosis of Patients With Clear Cell Renal Cell CarcinomaDocument8 pagesCytogenetic Profile Predicts Prognosis of Patients With Clear Cell Renal Cell CarcinomaRivan 21No ratings yet
- MainDocument8 pagesMainIoana CucuNo ratings yet
- Jurnal PrognosisDocument8 pagesJurnal PrognosisStella SulartoNo ratings yet
- Kju 49 781Document5 pagesKju 49 781estherin909No ratings yet
- Boelaert2006 PDFDocument7 pagesBoelaert2006 PDFgustianto hutama pNo ratings yet
- Koch 2009Document9 pagesKoch 2009Intan Kartika NursyahbaniNo ratings yet
- (2017) - Management and Prognosis of Ovarian Yolk Sac Tumors An Analysis of The National Cancer Data BaseDocument6 pages(2017) - Management and Prognosis of Ovarian Yolk Sac Tumors An Analysis of The National Cancer Data Basehop truongvanNo ratings yet
- Prostate Cancer 2015 ESMODocument9 pagesProstate Cancer 2015 ESMOpalomazul007No ratings yet
- Merrick2005 CCDocument11 pagesMerrick2005 CCantoine ailloudNo ratings yet
- Reduced Chemotherapy for Intermediate-Risk Neuroblastoma Yields High SurvivalDocument17 pagesReduced Chemotherapy for Intermediate-Risk Neuroblastoma Yields High Survivaldini kusmaharaniNo ratings yet
- Non-Suppressed Thyrotropin and Elevated Thyroglobulin Are Independent Predictors of Recurrence in Differentiated Thyroid CarcinomaDocument8 pagesNon-Suppressed Thyrotropin and Elevated Thyroglobulin Are Independent Predictors of Recurrence in Differentiated Thyroid CarcinomaPressureserveNo ratings yet
- Molecular Diagnostics in Cytopathology: A Practical Handbook for the Practicing PathologistFrom EverandMolecular Diagnostics in Cytopathology: A Practical Handbook for the Practicing PathologistSinchita Roy-ChowdhuriNo ratings yet
- Detecting and Diagnosing Diseases of the Peritoneal CavityDocument19 pagesDetecting and Diagnosing Diseases of the Peritoneal CavityJoanna BisNo ratings yet
- 2.3 - LIVER Patho - ARBDocument73 pages2.3 - LIVER Patho - ARBCRUZ Jill EraNo ratings yet
- CTR Conference BookletDocument150 pagesCTR Conference BookletAhmad Abu-AyshehNo ratings yet
- TiflitisDocument5 pagesTiflitisJosé Luis Navarro RomeroNo ratings yet
- History of Cancer ChemotherapyDocument9 pagesHistory of Cancer ChemotherapyJoydeep MajumdarNo ratings yet
- Nihms 737785Document78 pagesNihms 737785afg_19No ratings yet
- Breast Cancer TreatmentDocument13 pagesBreast Cancer TreatmentRissa AlmiraNo ratings yet
- Bse (Breast Self Examination) : Wykenie B. Fernandez, RN, ManDocument25 pagesBse (Breast Self Examination) : Wykenie B. Fernandez, RN, ManWykenie Fernandez OwensNo ratings yet
- Assessing The Genetic Impact of Enterococcus FaecaDocument10 pagesAssessing The Genetic Impact of Enterococcus Faecayonnu aasNo ratings yet
- Bevacizumab Product Presentation ModuleDocument35 pagesBevacizumab Product Presentation ModuleBeryl OngNo ratings yet
- SIOP22 - EPoster ViewingDocument1,855 pagesSIOP22 - EPoster ViewingmgNo ratings yet
- Arleeluck C2395-Stu - Cancer Brochure TemplateDocument3 pagesArleeluck C2395-Stu - Cancer Brochure Templateapi-552283875No ratings yet
- Surgery MnemonicsDocument4 pagesSurgery MnemonicsMark Anthony Namoca100% (1)
- SGL1 - Breast ImagingDocument93 pagesSGL1 - Breast ImagingDarawan MirzaNo ratings yet
- Prostate - Needle.specimen - BX 1.0.0.0.REL CAPCPDocument17 pagesProstate - Needle.specimen - BX 1.0.0.0.REL CAPCPkarimahihdaNo ratings yet
- Union Christian College School of Health and Sciences City of San Fernando La UnionDocument11 pagesUnion Christian College School of Health and Sciences City of San Fernando La UnionJobelle AcenaNo ratings yet
- ĐÁP ÁN TIẾNG ANH CHUYÊN NGÀNH - Y DU KÍ MÙA 2Document7 pagesĐÁP ÁN TIẾNG ANH CHUYÊN NGÀNH - Y DU KÍ MÙA 2Lộc HuỳnhNo ratings yet
- FfghhthjgvyujhDocument1 pageFfghhthjgvyujhBibek RajNo ratings yet
- Temozolomide in Glioblastoma Multiforme: Dr. Djoko Widodo, DR., Spbs (K)Document19 pagesTemozolomide in Glioblastoma Multiforme: Dr. Djoko Widodo, DR., Spbs (K)Andre KristantoNo ratings yet
- Original ContributionDocument8 pagesOriginal ContributionĐô Lê PhiNo ratings yet
- Lecture 3 Associated Risk FactorsDocument55 pagesLecture 3 Associated Risk FactorsTHANISHTA KUMARNo ratings yet
- Breast Cancer by Professor B. T. UgwuDocument16 pagesBreast Cancer by Professor B. T. UgwuMusaNo ratings yet
- Why Are Elephants Less Likely To Get CancerDocument8 pagesWhy Are Elephants Less Likely To Get Canceralicia tNo ratings yet
- ENGLISH REFARAT 3.2 - Sem 5 - Septina - Malignant Tumours With Follicular DifferentiationDocument28 pagesENGLISH REFARAT 3.2 - Sem 5 - Septina - Malignant Tumours With Follicular DifferentiationAffan Akbar TalamiNo ratings yet
- Pharmaceuticals 13 00081 v2Document9 pagesPharmaceuticals 13 00081 v2denisaNo ratings yet
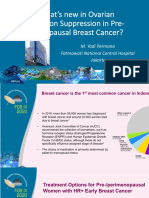
- 2.3.a DR Yadi Permana Whats New in Ovarian Function Suppression in Pre-MenopausalDocument36 pages2.3.a DR Yadi Permana Whats New in Ovarian Function Suppression in Pre-Menopausaltepat rshsNo ratings yet
- 2015 Nature Glypican 1 Identifies Cancer ExosomesDocument24 pages2015 Nature Glypican 1 Identifies Cancer ExosomesAgata HugglerNo ratings yet
- Prostate Fossa Contouring GuideDocument32 pagesProstate Fossa Contouring GuideAna Paula IoostNo ratings yet
- Endoscopic Treatment of Early Gastric CancerDocument47 pagesEndoscopic Treatment of Early Gastric CancerFaiza Hashim SoomroNo ratings yet