You might also like
- Visual attention to social and non-social objects across the autism spectrumFrom EverandVisual attention to social and non-social objects across the autism spectrumNo ratings yet
- hearing lossDocument10 pageshearing lossAndreaNo ratings yet
- Navigating Aging: A Comparative Analysis of Functional Health Among Elderly Individuals in Tamil NaduDocument12 pagesNavigating Aging: A Comparative Analysis of Functional Health Among Elderly Individuals in Tamil Naduindex PubNo ratings yet
- Trends in Vision and Hearing Among Older Americans: HighlightsDocument8 pagesTrends in Vision and Hearing Among Older Americans: HighlightsMansi DabhiNo ratings yet
- IntroductionPublic Health Is One of The Most Important Aspects of National Interest For Any CountryDocument10 pagesIntroductionPublic Health Is One of The Most Important Aspects of National Interest For Any CountrySammy GitauNo ratings yet
- Impact of Ageing On Depression and Activities of Daily Livings in Normal Elderly Subjects Living in Old Age Homes and Communities of Kanpur, U.PDocument8 pagesImpact of Ageing On Depression and Activities of Daily Livings in Normal Elderly Subjects Living in Old Age Homes and Communities of Kanpur, U.PDr. Krishna N. SharmaNo ratings yet
- Zeeshan and AslamDocument11 pagesZeeshan and AslamDian Atnantomi WiliyantoNo ratings yet
- Instrumental Activities of Daily Living and Subjective Wellbeing in Elderly Persons Living in CommunityDocument8 pagesInstrumental Activities of Daily Living and Subjective Wellbeing in Elderly Persons Living in CommunityNailis Sa'adahNo ratings yet
- Exploring The Association Between Multimorbidity and Cognitive Impairment in Older Adults Living in The Community: A Review of The LiteratureDocument11 pagesExploring The Association Between Multimorbidity and Cognitive Impairment in Older Adults Living in The Community: A Review of The LiteraturenabilahbilqisNo ratings yet
- 2019.neglect Older PeopleDocument17 pages2019.neglect Older PeopleambiebieNo ratings yet
- Alzheimer's Disease Research PaperDocument10 pagesAlzheimer's Disease Research PaperHeidi Czaplewski100% (1)
- Neglect Towards Elders in Geriatric Care Settings 3Document15 pagesNeglect Towards Elders in Geriatric Care Settings 3blairNo ratings yet
- Health Care Disparities and The HomelessDocument6 pagesHealth Care Disparities and The Homelessapi-520141947100% (1)
- UC San Diego Previously Published WorksDocument10 pagesUC San Diego Previously Published WorksNinda AlzaNo ratings yet
- Disparidad de Salud en DemenciaDocument13 pagesDisparidad de Salud en Demenciajhoel cruzNo ratings yet
- American Journal of Occupational Therapy - 1Document13 pagesAmerican Journal of Occupational Therapy - 1TIMOTHY NYONGESANo ratings yet
- Community RanDocument10 pagesCommunity Ranmaestro1020No ratings yet
- Issues in Geriatic CareDocument10 pagesIssues in Geriatic CarepremaNo ratings yet
- Intellectual DisabilityDocument25 pagesIntellectual DisabilityMatias CarreñoNo ratings yet
- Ageism & AdultismDocument13 pagesAgeism & AdultismRaazan SapkotaNo ratings yet
- StimsonmDocument25 pagesStimsonmapi-270067627No ratings yet
- Torres Cukier REAL 2021 - Use of Allied-Health Services and Medication Among Adults withASD in Latin AmericaDocument12 pagesTorres Cukier REAL 2021 - Use of Allied-Health Services and Medication Among Adults withASD in Latin Americanatalia barriosNo ratings yet
- Problems of Elderly - Issues & ImplicationsDocument9 pagesProblems of Elderly - Issues & ImplicationsŚáńtőśh Mőkáśhí100% (4)
- Chronic Illness and People With Intellectual Disability: Prevalence, Prevention and ManagementDocument42 pagesChronic Illness and People With Intellectual Disability: Prevalence, Prevention and ManagementErsya MusLih AnshoriNo ratings yet
- Issue Brief Final DraftDocument15 pagesIssue Brief Final Draftapi-664663354No ratings yet
- Vohra Et Al - 2014 - Access To Services, Quality of Care, and Family Impact For Children WithDocument20 pagesVohra Et Al - 2014 - Access To Services, Quality of Care, and Family Impact For Children WithJose A RodasNo ratings yet
- Blah 5 AsdsadsaadsDocument11 pagesBlah 5 Asdsadsaadsprern27No ratings yet
- Review of Related LiteratureDocument28 pagesReview of Related LiteratureporseenaNo ratings yet
- Lonely Young Adults in Modern Britain Findings From An Epidemiological Cohort StudyDocument10 pagesLonely Young Adults in Modern Britain Findings From An Epidemiological Cohort StudyTinaNo ratings yet
- Review of Related LiteratureDocument28 pagesReview of Related LiteratureporseenaNo ratings yet
- Addressing Everyday ChallengesDocument10 pagesAddressing Everyday ChallengesbirjuNo ratings yet
- Krahn Et Al Article - Disability Health DisparitiesDocument9 pagesKrahn Et Al Article - Disability Health DisparitiesMarieNo ratings yet
- Spinal Cord Injury and Its Impact On The Patient Family and The SocietyDocument4 pagesSpinal Cord Injury and Its Impact On The Patient Family and The SocietyInt Journal of Recent Surgical and Medical SciNo ratings yet
- Shin 2012Document7 pagesShin 2012Miranti Dea DoraNo ratings yet
- Mary LonelinessDocument14 pagesMary LonelinessAlade TemitayoNo ratings yet
- Role of RNDocument6 pagesRole of RNCheng IrisNo ratings yet
- Factors That Affect Normal Functioning of The Older PersonsDocument7 pagesFactors That Affect Normal Functioning of The Older Personslouie john abilaNo ratings yet
- Ageing and Mental Health in India A Wakeup CallDocument18 pagesAgeing and Mental Health in India A Wakeup CallmeherprishanunnaNo ratings yet
- Oxford Handbooks Online: Intellectual DisabilitiesDocument20 pagesOxford Handbooks Online: Intellectual DisabilitiesCristinaNo ratings yet
- Oxford Handbooks Online: Intellectual DisabilitiesDocument20 pagesOxford Handbooks Online: Intellectual DisabilitiesCristina100% (1)
- Literature ReviewDocument7 pagesLiterature Reviewapi-583321795No ratings yet
- Ethical ConsiderationsDocument15 pagesEthical ConsiderationsANA DelafuenteNo ratings yet
- Assessment of Depression Among Older AdultsDocument9 pagesAssessment of Depression Among Older Adultsrani nauraNo ratings yet
- Liran Rafaely, Sara Carmel & Yaacov G. Bachner (2018)Document9 pagesLiran Rafaely, Sara Carmel & Yaacov G. Bachner (2018)vascoNo ratings yet
- Assignment 5Document3 pagesAssignment 5Saher AslamNo ratings yet
- Healthcare 09 01536Document11 pagesHealthcare 09 01536Rifqi Fathul ArroisiNo ratings yet
- Ageing in India Some Social Challenges To Elderly CarDocument2 pagesAgeing in India Some Social Challenges To Elderly CarHenryNo ratings yet
- Valoración Geriátrica IntegralDocument13 pagesValoración Geriátrica IntegralBlackthestralNo ratings yet
- Are We Making A Difference in Primary Care For AdultsDocument10 pagesAre We Making A Difference in Primary Care For Adultssanyun_anchNo ratings yet
- Gerontology and Geriatric Medicine: HSOA Journal ofDocument8 pagesGerontology and Geriatric Medicine: HSOA Journal ofHerald Scholarly Open AccessNo ratings yet
- KARTIKA ZARI ARYANI 37D (Tugas Summary General Lecture GERIATRI)Document3 pagesKARTIKA ZARI ARYANI 37D (Tugas Summary General Lecture GERIATRI)TIKANo ratings yet
- Nursing roles in supporting the elderly and their caregiversDocument10 pagesNursing roles in supporting the elderly and their caregiversRichardTangNo ratings yet
- Self-Stigma Experiences Among Older Adults With MeDocument10 pagesSelf-Stigma Experiences Among Older Adults With MeKlinik KitamuraNo ratings yet
- 1 s2.0 S0002939423001150Document10 pages1 s2.0 S0002939423001150Alba García MarcoNo ratings yet
- Relationship of Stigmatization and Social Support With Depression 2022 HeliDocument7 pagesRelationship of Stigmatization and Social Support With Depression 2022 HeliMixa TekluNo ratings yet
- Understanding the Mental Health Needs of the ElderlyDocument36 pagesUnderstanding the Mental Health Needs of the ElderlyKadiah KamaraNo ratings yet
- HHS Public Access: Ageism in Informal Care Network Members of Older WomenDocument17 pagesHHS Public Access: Ageism in Informal Care Network Members of Older WomenElena FNo ratings yet
- Social and Community Inclusion Outcomes For Adults With...Document13 pagesSocial and Community Inclusion Outcomes For Adults With...NobodyNo ratings yet
- Caring for the Elderly: Experiences in Nursing HomesDocument2 pagesCaring for the Elderly: Experiences in Nursing HomesRhin FrancineNo ratings yet
- Assessment of Older People 5: Assessing The Social DomainDocument4 pagesAssessment of Older People 5: Assessing The Social DomainSuci ErvindaNo ratings yet
- NCM 103 Administering Intramuscular MedicationDocument16 pagesNCM 103 Administering Intramuscular MedicationAdrynnette Cruz-LastimadoNo ratings yet
- Scissor Lift ProcedureDocument2 pagesScissor Lift ProcedureAdhi LatifNo ratings yet
- Compre FundaDocument10 pagesCompre FundaAngie SaquingNo ratings yet
- UntitledDocument7 pagesUntitledSucdi AbdirazakNo ratings yet
- Runner Ru4rxDocument45 pagesRunner Ru4rxfcdypmsbssNo ratings yet
- Vale FormDocument1 pageVale FormRANDY BAOGBOGNo ratings yet
- Administrative Diagnosis: Assessing Organizational ProblemsDocument9 pagesAdministrative Diagnosis: Assessing Organizational ProblemsmohammadNo ratings yet
- HACH LANGE Ascorbic Acid PP (1457799) - ENGDocument5 pagesHACH LANGE Ascorbic Acid PP (1457799) - ENGkerem__22No ratings yet
- Cookery1-SPECIALIZED-FINAL 1Document37 pagesCookery1-SPECIALIZED-FINAL 1Princess Aira Malveda100% (1)
- CS 704 Socio-Emotional and Moral Development in Middle ChildhoodDocument25 pagesCS 704 Socio-Emotional and Moral Development in Middle ChildhoodPatricia PamintuanNo ratings yet
- MSDS DDDocument2 pagesMSDS DDBaher SaidNo ratings yet
- EMP 412 - Teaching - Notes - Topic - 1 - Economics - of - Education - and - Human - Capital - Theory - 1Document17 pagesEMP 412 - Teaching - Notes - Topic - 1 - Economics - of - Education - and - Human - Capital - Theory - 1Saka FelistarNo ratings yet
- Australian VSK 2018 LRDocument13 pagesAustralian VSK 2018 LRmuhamadrafie1975No ratings yet
- Broselow Pediatric Emergency TapeDocument13 pagesBroselow Pediatric Emergency TapePaulo KaleNo ratings yet
- Final Draft of Interview TranscriptDocument7 pagesFinal Draft of Interview Transcriptapi-549369201No ratings yet
- Sylvia PlathDocument12 pagesSylvia Plathapi-534201968No ratings yet
- Introduction To Architectural ProgrammingDocument34 pagesIntroduction To Architectural ProgrammingbalaNo ratings yet
- Psychology Learning Objectives, Contents, Activities and EvaluationDocument12 pagesPsychology Learning Objectives, Contents, Activities and EvaluationSAYMABANUNo ratings yet
- Benefits of Eating Dark Chocolate and White Chocolate Bars in Third Year Psychology Students in Cavite State University Silang CampusDocument12 pagesBenefits of Eating Dark Chocolate and White Chocolate Bars in Third Year Psychology Students in Cavite State University Silang CampusPRINCE SARNONo ratings yet
- Introduction To Criminology: By: Catherine G. Acedo, RcrimDocument34 pagesIntroduction To Criminology: By: Catherine G. Acedo, RcrimJEEHAN DELA CRUZNo ratings yet
- CEMP-Framework Beach Project Scope Rev0Document152 pagesCEMP-Framework Beach Project Scope Rev0gowthamNo ratings yet
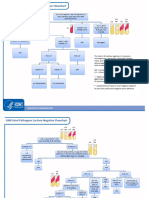
- GNR Stool Pathogens Lactose Negative FlowchartDocument2 pagesGNR Stool Pathogens Lactose Negative FlowchartKeithNo ratings yet
- Welfare Services For Challenged ChildrenDocument42 pagesWelfare Services For Challenged ChildrenRahul Dhaker70% (10)
- Centric Relation Registration With Intraoral Central Bearing On Curved vs. Flat Plates With Rim Trays in Edentulous PatientsDocument8 pagesCentric Relation Registration With Intraoral Central Bearing On Curved vs. Flat Plates With Rim Trays in Edentulous PatientsCamila MuñozNo ratings yet
- Palliative Care Referral SystemDocument6 pagesPalliative Care Referral SystemNATHANIEL YERINo ratings yet
- (24513105 - BANTAO Journal) Oral and Salivary Changes in Patients With Chronic Kidney DiseaseDocument6 pages(24513105 - BANTAO Journal) Oral and Salivary Changes in Patients With Chronic Kidney DiseaseVera Radojkova NikolovskaNo ratings yet
- De-Escalation - Aggression Management TechniquesDocument14 pagesDe-Escalation - Aggression Management Techniquesparis emmaNo ratings yet
- November 2022 Philippine Nurse Licensure Examination ResultsDocument6 pagesNovember 2022 Philippine Nurse Licensure Examination ResultsRappler0% (1)
- Soil Analysis and Agricultural Survey: Jagtap & K. P. Patel 2014)Document7 pagesSoil Analysis and Agricultural Survey: Jagtap & K. P. Patel 2014)Sarvesh RautNo ratings yet
- The Process of PhlebotomyDocument102 pagesThe Process of PhlebotomyCatherine Merilleno100% (1)