You might also like
- Physiology of BalanceDocument45 pagesPhysiology of BalanceThadei MrumaNo ratings yet
- Vestibular DisordersDocument8 pagesVestibular DisordersHilwy Al-haninNo ratings yet
- Vestibuloocular Reflex Testing: Emedicine Specialties Clinical Procedures NoneDocument11 pagesVestibuloocular Reflex Testing: Emedicine Specialties Clinical Procedures NoneNarendra MaliNo ratings yet
- The Vestibular System: Michael E. Goldberg, M.D. Please Sit Where You Can Examine A PartnerDocument36 pagesThe Vestibular System: Michael E. Goldberg, M.D. Please Sit Where You Can Examine A PartnerlindaNo ratings yet
- Proprioception, Vestibular & CoordinationDocument28 pagesProprioception, Vestibular & Coordinationzm2h8hpsq8No ratings yet
- Acute Dizziness, Vertigo, and Unsteadiness 2021 NCDocument17 pagesAcute Dizziness, Vertigo, and Unsteadiness 2021 NCLaura A M MNo ratings yet
- VOR FornixDocument10 pagesVOR FornixIneke IntaniaNo ratings yet
- Visual-Vestibular Interaction - Basic Science To Clinical RelevanceDocument13 pagesVisual-Vestibular Interaction - Basic Science To Clinical RelevanceEnrico ArmatoNo ratings yet
- Vestibular DysfunctionDocument23 pagesVestibular DysfunctionEnzo VicencioNo ratings yet
- Vestibuloocular Reflex Testing: Emedicine Specialties Clinical Procedures NoneDocument11 pagesVestibuloocular Reflex Testing: Emedicine Specialties Clinical Procedures NonemannjainNo ratings yet
- Anatomy & Physiology of Vestibular System.Document68 pagesAnatomy & Physiology of Vestibular System.Prasanna DattaNo ratings yet
- Cervical Vertigo: Nosological Entities?Document5 pagesCervical Vertigo: Nosological Entities?Rendra DananjayaNo ratings yet
- Vertigo Physiology and Clinical AssessmentDocument63 pagesVertigo Physiology and Clinical AssessmentdraseemmishraNo ratings yet
- Dr. Herman - Physiology of EquilibriumDocument70 pagesDr. Herman - Physiology of EquilibriumAndrew Sabastian Geraldyno PaagoNo ratings yet
- Animal Physiology 1Document29 pagesAnimal Physiology 1ADITYAROOP PATHAKNo ratings yet
- Ataxia em GatosDocument12 pagesAtaxia em GatosGabriela De Aguiar KufnerNo ratings yet
- Gangguan Keseimbangan Pada LansiaDocument52 pagesGangguan Keseimbangan Pada LansiaSyarifah Ro'fah100% (1)
- Understanding A Dizzy AdultDocument39 pagesUnderstanding A Dizzy AdultR Srinivasa RaghavanNo ratings yet
- Revised Vestibular System 1Document7 pagesRevised Vestibular System 1KevinYonathanNo ratings yet
- Chapter Three Vestibular SystemDocument22 pagesChapter Three Vestibular SystemramopavelNo ratings yet
- Human Balance SystemDocument5 pagesHuman Balance SystemHendri SaputraNo ratings yet
- Why Understanding Brain Structure and Reflexes Is Important in NursingDocument10 pagesWhy Understanding Brain Structure and Reflexes Is Important in NursingPaul BarriosNo ratings yet
- Examination of v. SystemDocument64 pagesExamination of v. SystemYibeltalNo ratings yet
- Rund Aljarrah Dana RidaDocument54 pagesRund Aljarrah Dana RidaRundNo ratings yet
- Benign Paroxysmal Positional Vertigo & Lung MassDocument4 pagesBenign Paroxysmal Positional Vertigo & Lung MassKevin Roy MirandaNo ratings yet
- Vestibular Lecture - Anatomy - PhysiologyDocument85 pagesVestibular Lecture - Anatomy - PhysiologyJawad MohammadNo ratings yet
- 4 2 19 517Document10 pages4 2 19 517fitria indah SekarwangiNo ratings yet
- Disorders of The Vestibular SystemDocument25 pagesDisorders of The Vestibular SystemEnzo VicencioNo ratings yet
- Dizziness and VertigoDocument27 pagesDizziness and VertigoPutriAyuWidyastutiRNo ratings yet
- CNS Path Pharm KelnerDocument9 pagesCNS Path Pharm Kelnerjazzdoc007No ratings yet
- A Simple Guide to The Posture, Spine Diseases and Use in Disease DiagnosisFrom EverandA Simple Guide to The Posture, Spine Diseases and Use in Disease DiagnosisNo ratings yet
- Spinal Cord AnatomyDocument6 pagesSpinal Cord AnatomyBharath Raj YadavNo ratings yet
- Anatomical Characteristics of The Vestibular SystemDocument7 pagesAnatomical Characteristics of The Vestibular SystemRuth AlooNo ratings yet
- Black Vestibular DisordersDocument102 pagesBlack Vestibular DisorderskimNo ratings yet
- 14 Osteopathic Manipulative Treatment - HVLA Procedure - Cervical Vertebrae - StatPearls - NCBI BookshelfDocument11 pages14 Osteopathic Manipulative Treatment - HVLA Procedure - Cervical Vertebrae - StatPearls - NCBI Bookshelfjaswant bhadaneNo ratings yet
- Vertigo - A Practical Approach: Vertigo Is A Relatively Common Presentation in General PracticeDocument12 pagesVertigo - A Practical Approach: Vertigo Is A Relatively Common Presentation in General PracticeKarl Martin PinedaNo ratings yet
- Types of VertigoDocument3 pagesTypes of VertigoAkanksha PashineyNo ratings yet
- Cervical Vertigo PDFDocument5 pagesCervical Vertigo PDFPaijo SusenoNo ratings yet
- Dance Psychology Section 4 Lecture 14 Dance Vertigo & Balance CompressedDocument13 pagesDance Psychology Section 4 Lecture 14 Dance Vertigo & Balance CompressedMariel NaumazevNo ratings yet
- Vertigo, A Simple Guide to The Condition, Treatment And Related ConditionsFrom EverandVertigo, A Simple Guide to The Condition, Treatment And Related ConditionsRating: 5 out of 5 stars5/5 (1)
- Spastic TorticollisDocument2 pagesSpastic TorticollisRamesh SinghNo ratings yet
- Lopez - Neil - Case StudyDocument17 pagesLopez - Neil - Case StudyNeil LopezNo ratings yet
- Physiology of Balance/Equilibrium: Departemen Fisiologi FK UsuDocument20 pagesPhysiology of Balance/Equilibrium: Departemen Fisiologi FK UsuSonia P SNo ratings yet
- Extrapyramidal Disorders, OedemaDocument104 pagesExtrapyramidal Disorders, OedemaAyman RehmanNo ratings yet
- Equilibrium: DR - Basma ElgatanyDocument26 pagesEquilibrium: DR - Basma ElgatanyEklas Kalame2218No ratings yet
- The Cerebellum: Clinical ExaminationDocument70 pagesThe Cerebellum: Clinical ExaminationTarun MathurNo ratings yet
- 3-Vestibular System Part 2 - StudentsDocument18 pages3-Vestibular System Part 2 - StudentsjessNo ratings yet
- B.4 Paper VertigoDocument34 pagesB.4 Paper VertigoAnonymous oiHTNWLNo ratings yet
- Sense Organ:vestibular OrganDocument55 pagesSense Organ:vestibular OrganivanNo ratings yet
- Vestibular Disorder and Rehab PDFDocument15 pagesVestibular Disorder and Rehab PDFMehul RathoreNo ratings yet
- Vestibular Disorders and Rehabilitations: 1. AnatomyDocument15 pagesVestibular Disorders and Rehabilitations: 1. AnatomyMehul RathoreNo ratings yet
- Cerebellum S23Document26 pagesCerebellum S23Mansoor MughalNo ratings yet
- Jaut 12 I 1 P 11Document9 pagesJaut 12 I 1 P 11lisa ekaNo ratings yet
- Ataxia Physical Therapy and Rehabilitation Applications For Ataxic PatientsDocument19 pagesAtaxia Physical Therapy and Rehabilitation Applications For Ataxic PatientsAnastasios ChortisNo ratings yet
- 2017 Spine ExaminationDocument7 pages2017 Spine Examinationradhika thapaNo ratings yet
- Case StudyDocument9 pagesCase StudySamantha AdduruNo ratings yet
- Spinal InjuryDocument62 pagesSpinal Injuryanupama vargheseNo ratings yet
- Oscillopsia Is The Illusion of Oscillation of The Visual Surroundings While Vertigo Refers To A Sense of Spinning or Other Motion That May Be PhysiologicalDocument2 pagesOscillopsia Is The Illusion of Oscillation of The Visual Surroundings While Vertigo Refers To A Sense of Spinning or Other Motion That May Be PhysiologicalRubie Ann TillorNo ratings yet
- NC - Muh HafizDocument16 pagesNC - Muh HafizDodi DiNo ratings yet
- PPPD HandoutDocument5 pagesPPPD HandoutLeeNo ratings yet
- Geography of Health and EnvironmentDocument11 pagesGeography of Health and EnvironmentMohaiminul Islam BappyNo ratings yet
- Article Discourse AnalysisDocument11 pagesArticle Discourse AnalysisAseel Atef NassarNo ratings yet
- Types of Personality DisorderDocument2 pagesTypes of Personality DisorderWinnie Salazar AriolaNo ratings yet
- Materialism Medicine PDFDocument25 pagesMaterialism Medicine PDFSravani0% (1)
- Try This! Directions: Answer All The Necessary Information Needed in The Column Below. UseDocument10 pagesTry This! Directions: Answer All The Necessary Information Needed in The Column Below. UseChristine Joy Molina100% (1)
- AtpdDocument48 pagesAtpddrkadiyala2100% (2)
- Foodborne IllnessDocument16 pagesFoodborne IllnessPardeep SinghNo ratings yet
- Health Assessment QuizDocument3 pagesHealth Assessment QuizSamantha Joy VidalNo ratings yet
- Viral Latency and Immune EvasionDocument11 pagesViral Latency and Immune Evasionማላያላም ማላያላም100% (1)
- FilgrastimDocument3 pagesFilgrastimfransiscaNo ratings yet
- Public Health Midterm StudyguideDocument21 pagesPublic Health Midterm StudyguideJustin Lee100% (1)
- Inflammation Questions: Dr. Abdullah Al-Samawi Professor of PathologyDocument147 pagesInflammation Questions: Dr. Abdullah Al-Samawi Professor of PathologyAhmed AzeezNo ratings yet
- Probabilistic Graphical ModelsDocument25 pagesProbabilistic Graphical ModelskhoantdNo ratings yet
- Typology of Nursing Problems FNCPDocument9 pagesTypology of Nursing Problems FNCPPrsnigarbha Dasi D PotianNo ratings yet
- ملخص عن حب الشبابDocument10 pagesملخص عن حب الشبابMohammadSAL-RawashdehNo ratings yet
- Ppok 2023 PDFDocument33 pagesPpok 2023 PDFBagas Trikuncoro BawonoNo ratings yet
- BARLA S. J. Emmanuel ETHNO MEDICINAL BELIEFS AND PRACTICES AMONG TRIBALS OF JHARKHANDDocument20 pagesBARLA S. J. Emmanuel ETHNO MEDICINAL BELIEFS AND PRACTICES AMONG TRIBALS OF JHARKHANDsaurabhshubhamNo ratings yet
- Starvation Biochem NotesDocument8 pagesStarvation Biochem NotesNkosi JupiterNo ratings yet
- Daftar Pustaka Fix GbsDocument2 pagesDaftar Pustaka Fix GbsElizabeth IvanaNo ratings yet
- My ThesisDocument10 pagesMy Thesishinduja reddipilliNo ratings yet
- Full Name Nationality Status SEX Place of Birth Date of Birth Passport Number Languages Educational QualificationsDocument3 pagesFull Name Nationality Status SEX Place of Birth Date of Birth Passport Number Languages Educational QualificationsHoseinNo ratings yet
- Cet 27 July 2012 KipiotiDocument6 pagesCet 27 July 2012 KipiotiMaureen SimNo ratings yet
- Unit Plan MSC Nursing 2nd YearDocument12 pagesUnit Plan MSC Nursing 2nd YearSanthu Su100% (4)
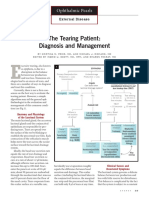
- The Tearing Patient: Diagnosis and Management: Ophthalmic PearlsDocument3 pagesThe Tearing Patient: Diagnosis and Management: Ophthalmic PearlsAnonymous otk8ohj9No ratings yet
- Jane Eyre Charlotte BronteDocument691 pagesJane Eyre Charlotte BrontePeggytaBruinhart100% (6)
- How To Read A CTGDocument31 pagesHow To Read A CTGAbdullah As'ad100% (1)
- Professional English in Use Medicine Book With Answers Table of ContentsDocument4 pagesProfessional English in Use Medicine Book With Answers Table of ContentsHeidy Barrientos15% (13)
- Bhutani's Color Atlas of Dermatology 6th EditionDocument495 pagesBhutani's Color Atlas of Dermatology 6th Editionparaschevi100% (8)