0% found this document useful (0 votes)
1K views8 pagesMetabolic Changes in Starvation Phases
The document discusses how metabolism and micronutrients are altered during periods of starvation and trauma. During starvation, metabolic processes slow down to conserve energy and adapt to calorie deprivation. After trauma, hormonal changes increase the demand for energy, proteins, and micronutrients. If nutritional requirements are not met during starvation or trauma, there may be a loss of body mass, body protein, and impairment of body functions.
Uploaded by
Nkosi JupiterCopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as DOCX, PDF, TXT or read online on Scribd
0% found this document useful (0 votes)
1K views8 pagesMetabolic Changes in Starvation Phases
The document discusses how metabolism and micronutrients are altered during periods of starvation and trauma. During starvation, metabolic processes slow down to conserve energy and adapt to calorie deprivation. After trauma, hormonal changes increase the demand for energy, proteins, and micronutrients. If nutritional requirements are not met during starvation or trauma, there may be a loss of body mass, body protein, and impairment of body functions.
Uploaded by
Nkosi JupiterCopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as DOCX, PDF, TXT or read online on Scribd
- The Phases of Starvation: Explains the physiological and metabolic changes occurring during starvation phases and their impact on the body.
- Early Stage of Fasting: Details glucose homeostasis mechanisms during the early fasting state and hormonal regulation.
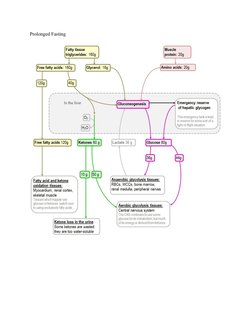
- Prolonged Fasting: Discusses the metabolic processes and substrate utilization during prolonged fasting.
- Key Points and Graphical Data: Summarizes key points about glucose regulation, including a graphical interpretation of metabolic pathways in starvation.
- Clinical Features of Starvation: Correlates clinical symptoms with biochemical changes in starvation, and outlines characteristics of disorders like anorexia nervosa.
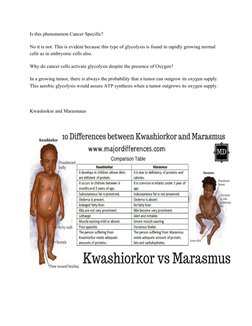
- Protein Energy Malnutrition: Illustrates the differences in metabolic changes between normal and cancer cells.
- Kwashiorkor vs Marasmus: Compares the characteristics, causes, and consequences of kwashiorkor and marasmus.
- Metabolic Response to Trauma: Explains how the body responds metabolically to trauma and its similarities to the starvation response.