You might also like
- Sample Business Plan For Bank Loan PDF594Document32 pagesSample Business Plan For Bank Loan PDF594assefamenelik1No ratings yet
- Project Proposal For WFP-Final13032019Document28 pagesProject Proposal For WFP-Final13032019simbiroNo ratings yet
- CLUP - Vol3 - Chapter 3 - SocialDocument90 pagesCLUP - Vol3 - Chapter 3 - SocialSharina GNo ratings yet
- GONZAGA NATIONAL HIGH SCHOOL Conplan SampleDocument41 pagesGONZAGA NATIONAL HIGH SCHOOL Conplan Samplejoei Arquero100% (2)
- Iloilo City Gov't Bring COVID-19 Vaccination To Villages: Leni Vs Sara: Why Robredo Is The Better ChoiceDocument1 pageIloilo City Gov't Bring COVID-19 Vaccination To Villages: Leni Vs Sara: Why Robredo Is The Better ChoiceFrancine Mhae SulitNo ratings yet
- Federal Republic of Somalia Ministry of Health & Human ServicesDocument2 pagesFederal Republic of Somalia Ministry of Health & Human Serviceshaileselassie bisratNo ratings yet
- Situation Report - Ethiopia - 20 Mar 2023Document16 pagesSituation Report - Ethiopia - 20 Mar 2023አማን በአማንNo ratings yet
- Ethiopia Flood Update No.3 18 August 2020Document5 pagesEthiopia Flood Update No.3 18 August 2020Tty SmithNo ratings yet
- CholeraOutbreakCTA 2023Document9 pagesCholeraOutbreakCTA 2023w.wills0011No ratings yet
- Emergency Plan of Action (Epoa) Ethiopia: Drought Emergency in South RegionsDocument23 pagesEmergency Plan of Action (Epoa) Ethiopia: Drought Emergency in South RegionsSufianNo ratings yet
- Inpursuitmadmul 00 DixogoogDocument38 pagesInpursuitmadmul 00 DixogoogIbrahim MoussaNo ratings yet
- SierraLeoneCountryProfile2013 PDFDocument2 pagesSierraLeoneCountryProfile2013 PDFBottle2014No ratings yet
- WFP 0000006330Document13 pagesWFP 0000006330Min AshtrielleNo ratings yet
- ET Support DU July2003Document7 pagesET Support DU July2003hundee100% (3)
- Ethiopia: Drought Update # 4Document4 pagesEthiopia: Drought Update # 4SufianNo ratings yet
- TyphoonsDocument15 pagesTyphoonsThea Sophia BuenoNo ratings yet
- Morocco - Earthquake - Disaster Brief - September - 2023Document5 pagesMorocco - Earthquake - Disaster Brief - September - 2023Aya KhalifaNo ratings yet
- Somali RHB Cholera Outbreak SitrepDocument6 pagesSomali RHB Cholera Outbreak SitrepManeNo ratings yet
- 1193 4484 1 PBDocument7 pages1193 4484 1 PBMohammad Iqbal MunirNo ratings yet
- MDRDZ009 OuDocument12 pagesMDRDZ009 OumyticmoneyNo ratings yet
- Situation Report - Ethiopia - 1 Dec 2023Document21 pagesSituation Report - Ethiopia - 1 Dec 2023Goytom NeayeNo ratings yet
- Humanitarian Situation Report-March April 2016Document9 pagesHumanitarian Situation Report-March April 2016Unicef RdCongoNo ratings yet
- Aedes (Stegomyia) Mosquitoes in The Ashanti Region of Ghana Implications For Yellow Fever PaucityDocument13 pagesAedes (Stegomyia) Mosquitoes in The Ashanti Region of Ghana Implications For Yellow Fever PaucityAlexander DeckerNo ratings yet
- Philippines' Country Profile: I. General InformationDocument38 pagesPhilippines' Country Profile: I. General InformationMark VillanuevaNo ratings yet
- The Casualties in The Caraga Region. (2 PTS)Document2 pagesThe Casualties in The Caraga Region. (2 PTS)KATHLEEN JOSOLNo ratings yet
- EPHI - PHEOC - COVID-19 and Drought Related PHE Bulletin - 01 - English - 04022023Document21 pagesEPHI - PHEOC - COVID-19 and Drought Related PHE Bulletin - 01 - English - 04022023Selam KidaneNo ratings yet
- B Acaps Start BN South Central Somalia Floods 30 October 2014Document4 pagesB Acaps Start BN South Central Somalia Floods 30 October 2014Salsabiil water well drillingNo ratings yet
- Progress On COVID-19: South Africa Public Health Response Minister of Health South AfricaDocument33 pagesProgress On COVID-19: South Africa Public Health Response Minister of Health South AfricaMail and Guardian50% (2)
- MDRPH051 DoDocument23 pagesMDRPH051 DoDiether AguilarNo ratings yet
- CP HealthDocument20 pagesCP Healthnjbxhycn4bNo ratings yet
- The Outbreak of Desert Locusts in The Eastern Africa RegionDocument4 pagesThe Outbreak of Desert Locusts in The Eastern Africa RegionGCICNo ratings yet
- An Overview of Factors Responsible For Geographic Distribution Pattern of Ixodid Ticks in The SudanDocument9 pagesAn Overview of Factors Responsible For Geographic Distribution Pattern of Ixodid Ticks in The SudanFrontiersNo ratings yet
- Cholera - Global SituationDocument10 pagesCholera - Global SituationOlmar Reyes UribeNo ratings yet
- Sudan COVID 19 Response Plan 2020Document12 pagesSudan COVID 19 Response Plan 2020mahammadNo ratings yet
- Somalia Rainfall Forecast 18 October 2023Document2 pagesSomalia Rainfall Forecast 18 October 2023npetkovski0101No ratings yet
- MDRET015Revised EPoADocument21 pagesMDRET015Revised EPoAMERHAWIT NEGATUNo ratings yet
- Op. Update Ecuador Floods and Earthquake March 2023Document30 pagesOp. Update Ecuador Floods and Earthquake March 2023riumbamikellinezcoNo ratings yet
- MDREBOLA21 Ear 1Document19 pagesMDREBOLA21 Ear 1aniket singhNo ratings yet
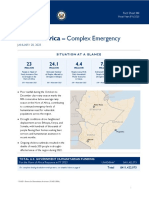
- 2023-01-20 USG Horn of Africa Complex Emergency Fact Sheet 4 0Document6 pages2023-01-20 USG Horn of Africa Complex Emergency Fact Sheet 4 0Suad AbdulmajedNo ratings yet
- Article1380636119 - Onyeka Et AlDocument8 pagesArticle1380636119 - Onyeka Et AlBabatunde Idowu EbenezerNo ratings yet
- 109753-301481-1-PB: White Mango Scale, Aulacaspis Tubercularis, Distribution and Severity Status in East and West Wollega Zones, Western EthiopiaDocument10 pages109753-301481-1-PB: White Mango Scale, Aulacaspis Tubercularis, Distribution and Severity Status in East and West Wollega Zones, Western EthiopiaTemesgen FitaNo ratings yet
- OVJ-2018-04-100 D. GebremichaelDocument9 pagesOVJ-2018-04-100 D. GebremichaelOriosNo ratings yet
- Malaria in Somalia: Assembling The Evidence and Modelling RisksDocument34 pagesMalaria in Somalia: Assembling The Evidence and Modelling RisksdrhaariyeNo ratings yet
- Syria - COVID-19 - Humanitarian Update - No 25 - 5 April - FINALDocument10 pagesSyria - COVID-19 - Humanitarian Update - No 25 - 5 April - FINALlive freedomNo ratings yet
- Climate Variability and The Yora' Rural Community in The Commune of Djougou, Donga Department, in The North-West of BeninDocument8 pagesClimate Variability and The Yora' Rural Community in The Commune of Djougou, Donga Department, in The North-West of Beniniaset123No ratings yet
- Pre-Scaling Up of Improved Finger Millet Technologies: The Case of Daro Lebu and Habro Districts of West Hararghe Zone, Oromia National Regional State, EthiopiaDocument9 pagesPre-Scaling Up of Improved Finger Millet Technologies: The Case of Daro Lebu and Habro Districts of West Hararghe Zone, Oromia National Regional State, EthiopiaPremier PublishersNo ratings yet
- The Role of Rodents and Small Carnivores in Plague Ende-Micity in TanzaniaDocument8 pagesThe Role of Rodents and Small Carnivores in Plague Ende-Micity in TanzaniacaliNo ratings yet
- Occupied Palestinian Territory (Opt) : Covid-19 Emergency: Situation Report No. 18Document11 pagesOccupied Palestinian Territory (Opt) : Covid-19 Emergency: Situation Report No. 18kovi mNo ratings yet
- Anthrax Action Plan For Tigray No Cost ExtensionDocument7 pagesAnthrax Action Plan For Tigray No Cost ExtensionNega TewoldeNo ratings yet
- Stl-Emergency Situation Report-21.06.2023Document14 pagesStl-Emergency Situation Report-21.06.2023Mohamad Samer S. ALYASAKINo ratings yet
- Morocco: Earthquake: in BriefDocument8 pagesMorocco: Earthquake: in BriefChaitra KamuriNo ratings yet
- Multi-Country Outbreak-Of-Cholera Sitrep 11Document18 pagesMulti-Country Outbreak-Of-Cholera Sitrep 11HZT 99No ratings yet
- 10 1 1 573 7049Document8 pages10 1 1 573 70495-Mint PUBGNo ratings yet
- Som Unicef Somrvwnov06fnlacDocument6 pagesSom Unicef Somrvwnov06fnlacOmar AwaleNo ratings yet
- Geo Ass 1Document12 pagesGeo Ass 1Kort LeonardnforNo ratings yet
- TabueDocument11 pagesTabueibrahima1968No ratings yet
- Application of Geographical Information System (GIS) Technology in The Control of Buruli Ulcer in GhanaDocument9 pagesApplication of Geographical Information System (GIS) Technology in The Control of Buruli Ulcer in GhanaKj_bdNo ratings yet
- The Spatial Distribution of Anopheles Gambiae Sensu Stricto and An. Arabiensis (Diptera: Culicidae) in MaliDocument10 pagesThe Spatial Distribution of Anopheles Gambiae Sensu Stricto and An. Arabiensis (Diptera: Culicidae) in Maliibrahima1968No ratings yet
- The Development Agricultural Land The Transmission Sleeping Sickness in Daloa, Côte D'ivoireDocument12 pagesThe Development Agricultural Land The Transmission Sleeping Sickness in Daloa, Côte D'ivoireLowell SmithNo ratings yet
- Time and Power in Azraq Refugee Camp: A Nine-to-Five EmergencyFrom EverandTime and Power in Azraq Refugee Camp: A Nine-to-Five EmergencyNo ratings yet
- Ebola Virus Disease: A Manual for EVD ManagementFrom EverandEbola Virus Disease: A Manual for EVD ManagementMarta LadoNo ratings yet
- Business Plan For Industrial Zone Edited 2Document33 pagesBusiness Plan For Industrial Zone Edited 2assefamenelik1No ratings yet
- ZewdineshDocument27 pagesZewdineshassefamenelik1No ratings yet
- NEGASI Feasiblity Study FinalDocument32 pagesNEGASI Feasiblity Study Finalassefamenelik1No ratings yet
- @30digital Marketing On Hotel Busines PerformaceDocument80 pages@30digital Marketing On Hotel Busines Performaceassefamenelik1No ratings yet
- Business Plan Format Commercial BankDocument5 pagesBusiness Plan Format Commercial Bankassefamenelik1100% (2)
- WitnessDocument1 pageWitnessassefamenelik1No ratings yet
- Hand To Hand Business PlanDocument32 pagesHand To Hand Business Planassefamenelik1No ratings yet
- CGAP Technical Guide Due Diligence Guidelines For The Review of Microcredit Loan Portfolios Dec 2009Document58 pagesCGAP Technical Guide Due Diligence Guidelines For The Review of Microcredit Loan Portfolios Dec 2009assefamenelik1No ratings yet
- Horizontal Intergovernmental Relations Between Ethiopian Federating Units: The Case of Amhara and Benshangul Gumuz RegionsDocument103 pagesHorizontal Intergovernmental Relations Between Ethiopian Federating Units: The Case of Amhara and Benshangul Gumuz RegionsDessalegnNo ratings yet
- 06 Chapter 1Document58 pages06 Chapter 1ልጅ እያሱNo ratings yet
- COUNTRY Food Security UpdateDocument4 pagesCOUNTRY Food Security UpdateSamson HaileyesusNo ratings yet
- Oromia Region 2017 Meher Assessment Non Food Draft Report 20 Dec'17 - FDocument58 pagesOromia Region 2017 Meher Assessment Non Food Draft Report 20 Dec'17 - FMERHAWIT NEGATU100% (1)
- DEMEKECH Proposal PADMDocument19 pagesDEMEKECH Proposal PADMAbdi AdanNo ratings yet
- Community FacilitatorDocument3 pagesCommunity FacilitatorDanbobi Shaka DubeNo ratings yet
- FACILITY RRF Reporting Rate 2013Document43 pagesFACILITY RRF Reporting Rate 2013zinabu tesfayeNo ratings yet
- Ethiopia: Drought Update # 4Document4 pagesEthiopia: Drought Update # 4SufianNo ratings yet
- The Quest For The Resolution of Guji-Gedeo Conflicts in Southern EthiopiaDocument42 pagesThe Quest For The Resolution of Guji-Gedeo Conflicts in Southern EthiopiaRamona Padurean100% (1)
- #7 Launching Site Journal 56962-204659-1-PBDocument19 pages#7 Launching Site Journal 56962-204659-1-PBLijalem GebrehiwetNo ratings yet
- Oromia National Regional State Borena Zone Finance and Economic Cooperation Office Offices Now InviteDocument3 pagesOromia National Regional State Borena Zone Finance and Economic Cooperation Office Offices Now InviteichichbinNo ratings yet
- Livestock Value Chain and Market Study in BorenaDocument47 pagesLivestock Value Chain and Market Study in BorenaYusuff QuadrilateralNo ratings yet
- Third Party Soft Copy Report FormDocument1 pageThird Party Soft Copy Report Formlight of moonNo ratings yet
- Indigenous and Modern Environmental EthicsDocument358 pagesIndigenous and Modern Environmental EthicsAbiyot NegeraNo ratings yet
- Environment BorenaDocument31 pagesEnvironment BorenaGuutaa DirbabaaNo ratings yet