You might also like
- Magnetic Resonance Imaging: Recording, Reconstruction and AssessmentFrom EverandMagnetic Resonance Imaging: Recording, Reconstruction and AssessmentRating: 5 out of 5 stars5/5 (1)
- 1 s2.0 S1746809422007662 MainDocument11 pages1 s2.0 S1746809422007662 MainWided HechkelNo ratings yet
- IQRO'Document8 pagesIQRO'Aulia HudaNo ratings yet
- MRI Preprocessing for Early Alzheimer's PredictionDocument4 pagesMRI Preprocessing for Early Alzheimer's PredictionMatheus SilvaNo ratings yet
- Brain Tumor Detection by Using Artificial Neural NetworkDocument6 pagesBrain Tumor Detection by Using Artificial Neural NetworkHaritha ReddyNo ratings yet
- A New Alzheimer's Disease Classification Technique From Brain MRI ImagesDocument6 pagesA New Alzheimer's Disease Classification Technique From Brain MRI ImagesBENAZIR BEGAM RNo ratings yet
- Alzheimer's Disease Classification Using Feed Forwarded Deep Neural Networks For Brain MRI ImagesDocument15 pagesAlzheimer's Disease Classification Using Feed Forwarded Deep Neural Networks For Brain MRI ImagesWided HechkelNo ratings yet
- Diagnostics 11 01589 v2Document19 pagesDiagnostics 11 01589 v2sekharraoNo ratings yet
- Paper 07Document15 pagesPaper 07Electro ElkoranyNo ratings yet
- Paper 1 Deep Learning Cardiac Motion Analysis For Human Survival PredictionDocument14 pagesPaper 1 Deep Learning Cardiac Motion Analysis For Human Survival PredictionShambhavi Malik 5-Yr. IDD Biomedical Engg., IIT(BHU), VaranasiNo ratings yet
- 2018-Aasd DfasdDocument10 pages2018-Aasd DfasdAhmet KaragozNo ratings yet
- Brain Sciences: A Deep Siamese Convolution Neural Network For Multi-Class Classification of Alzheimer DiseaseDocument15 pagesBrain Sciences: A Deep Siamese Convolution Neural Network For Multi-Class Classification of Alzheimer DiseaseVictorvikkNo ratings yet
- Ima 22549Document17 pagesIma 22549Muhammad Junaid AliNo ratings yet
- Applsci 11 06175Document22 pagesApplsci 11 06175Gurumoorthy KrishnamoorthyNo ratings yet
- Deep Learning Is Effective For Classifying Normal Versus Age-Related MacularDocument6 pagesDeep Learning Is Effective For Classifying Normal Versus Age-Related MacularNicolòNo ratings yet
- TMP 768 BDocument8 pagesTMP 768 BFrontiersNo ratings yet
- ContentsDocument85 pagesContentsJeevaNo ratings yet
- GL Neuro Img FDGDocument8 pagesGL Neuro Img FDGdanielep1No ratings yet
- Pet Vs Mbgi NeuroblastomaDocument12 pagesPet Vs Mbgi NeuroblastomaItzia VerduzcoNo ratings yet
- Journal 3 IJASEAIT Scopus AcceptedDocument9 pagesJournal 3 IJASEAIT Scopus AcceptedDigambar PuriNo ratings yet
- Alzheimer's Disease Diagnosis Based On The Hippocampal Unified Multi Atlas Network (HUMAN) AlgorithmDocument16 pagesAlzheimer's Disease Diagnosis Based On The Hippocampal Unified Multi Atlas Network (HUMAN) Algorithmdess101No ratings yet
- 3D Brain Slice Classification and Feature Extraction 2022 Computers in BiolDocument7 pages3D Brain Slice Classification and Feature Extraction 2022 Computers in Bioldebora eireneNo ratings yet
- Brain Tumor Segmentation Using Double Density Dual Tree Complex Wavelet Transform Combined With Convolutional Neural Network and Genetic AlgorithmDocument11 pagesBrain Tumor Segmentation Using Double Density Dual Tree Complex Wavelet Transform Combined With Convolutional Neural Network and Genetic AlgorithmIAES IJAINo ratings yet
- Multi Modal Classification of Alzheimer S Disease Using N 2017 Pattern RecogDocument11 pagesMulti Modal Classification of Alzheimer S Disease Using N 2017 Pattern RecogDesirée López PalafoxNo ratings yet
- A Simple Approach For Relatively Automated Hippocampus Segmentation From Sagittal View of Brain MriDocument8 pagesA Simple Approach For Relatively Automated Hippocampus Segmentation From Sagittal View of Brain MriijbbjournalNo ratings yet
- Deep Learning Based PET MR Radiomics For The ClassDocument8 pagesDeep Learning Based PET MR Radiomics For The ClassRon FranklinNo ratings yet
- A Novel Gaussian Discriminant Analysis-Based Computer Aided Diagnosis System For Screening Different Stages of Alzheimers DiseaseDocument6 pagesA Novel Gaussian Discriminant Analysis-Based Computer Aided Diagnosis System For Screening Different Stages of Alzheimers Disease1NT20CS076 KAMSALA THARUNNo ratings yet
- Spatial Component Analysis of MRI Data For Alzheimer's Disease Diagnosis: A Bayesian Network ApproachDocument8 pagesSpatial Component Analysis of MRI Data For Alzheimer's Disease Diagnosis: A Bayesian Network ApproachFrancisco Jesús Martínez MurciaNo ratings yet
- Dataset Meds2Document8 pagesDataset Meds2ANKIT KUMAR RAINo ratings yet
- 1 s2.0 S235239642200161X MainDocument13 pages1 s2.0 S235239642200161X Mainspamkt2002No ratings yet
- Prediction of Alzheimer's Disease Using CNNDocument11 pagesPrediction of Alzheimer's Disease Using CNNIJRASETPublications100% (2)
- IEEE Conference TemplateDocument4 pagesIEEE Conference TemplatepriyalNo ratings yet
- International Journal of Neuroscience: Alzheimer's diagnosis using deep learningDocument16 pagesInternational Journal of Neuroscience: Alzheimer's diagnosis using deep learningHaider ALHussainyNo ratings yet
- Brain Tumor Classification in MRI Image Using Convolutional Neural NetworkDocument14 pagesBrain Tumor Classification in MRI Image Using Convolutional Neural Networkaggarwal nNo ratings yet
- Predicting Alzheimer's Disease Progression Using Multi-Modal Deep Learning ApproachDocument12 pagesPredicting Alzheimer's Disease Progression Using Multi-Modal Deep Learning ApproachMayssa SOUSSIANo ratings yet
- Convolutional NeuralDocument13 pagesConvolutional NeuralVenky Naidu BalineniNo ratings yet
- Deep Learning Based Convolutional Neural Networks (DLCNN) On Classification Algorithm To Detect The Brain Turnor Diseases Using MRI and CT Scan ImagesDocument8 pagesDeep Learning Based Convolutional Neural Networks (DLCNN) On Classification Algorithm To Detect The Brain Turnor Diseases Using MRI and CT Scan ImagesInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- ECR 2022 ProgrammeDocument1,126 pagesECR 2022 ProgrammejbmbritoNo ratings yet
- AlzheimersDocument10 pagesAlzheimersDivya WaghmareNo ratings yet
- Overview On Segmentation and Classification For The Alzheimer's Disease Detection From Brain MRIDocument3 pagesOverview On Segmentation and Classification For The Alzheimer's Disease Detection From Brain MRISoorya Prakash ShuklaNo ratings yet
- Research Article: Brain MR Image Classification For Alzheimer's Disease Diagnosis Based On Multifeature FusionDocument14 pagesResearch Article: Brain MR Image Classification For Alzheimer's Disease Diagnosis Based On Multifeature FusionKrishna ReddyNo ratings yet
- Deep Learning Methods To Generate Synthetic CT From MRI in Radiotherapy A Literature ReviewDocument17 pagesDeep Learning Methods To Generate Synthetic CT From MRI in Radiotherapy A Literature ReviewColman SiuNo ratings yet
- Automated Tumor Segmentation in MR Brain Image Using Fuzzy C-Means Clustering and Seeded Region MethodologyDocument7 pagesAutomated Tumor Segmentation in MR Brain Image Using Fuzzy C-Means Clustering and Seeded Region MethodologyIAES IJAINo ratings yet
- ABSTRACTDocument11 pagesABSTRACTTime PassNo ratings yet
- Automated Brain Tumor Detection of MRI Image Based On Hybrid Image Processing TechniquesDocument10 pagesAutomated Brain Tumor Detection of MRI Image Based On Hybrid Image Processing TechniquesTELKOMNIKANo ratings yet
- Predicting Alzheimer's Disease Progression Using Multi-Modal Deep Learning ApproachDocument12 pagesPredicting Alzheimer's Disease Progression Using Multi-Modal Deep Learning ApproachManoj MaggotNo ratings yet
- Predicting Alzheimer's Disease: A Neuroimaging Study With 3D Convolutional Neural NetworksDocument9 pagesPredicting Alzheimer's Disease: A Neuroimaging Study With 3D Convolutional Neural NetworksManoj MaggotNo ratings yet
- 10.1109@ISMSIT.2019.8932878Document4 pages10.1109@ISMSIT.2019.8932878Vemula Prasanth KumarNo ratings yet
- Deep GradingDocument10 pagesDeep GradingLaudrup KaptueNo ratings yet
- 2103.14660Document6 pages2103.14660okuwobiNo ratings yet
- Update On Neuroimaging in Brain Tumours: ReviewDocument8 pagesUpdate On Neuroimaging in Brain Tumours: ReviewYo MismoNo ratings yet
- MCA-net - A Multi-Task Channel Attention Network For Myocardial Infarction Detection and Location Using 12-Lead ECGsDocument12 pagesMCA-net - A Multi-Task Channel Attention Network For Myocardial Infarction Detection and Location Using 12-Lead ECGs施展No ratings yet
- 1 s2.0 S1746809422003500 MainDocument16 pages1 s2.0 S1746809422003500 MainWided HechkelNo ratings yet
- 1 s2.0 S1746809421000744 MainDocument14 pages1 s2.0 S1746809421000744 Mainمظفر حسنNo ratings yet
- 1 s2.0 S2772528622000243 MainDocument15 pages1 s2.0 S2772528622000243 Mainmukundagarwalla2002No ratings yet
- Discriminating between bipolar and major depressive disorder using a machine learning approach and resting-state EEG dataDocument10 pagesDiscriminating between bipolar and major depressive disorder using a machine learning approach and resting-state EEG dataLander CannaertsNo ratings yet
- El Valor Diagnostico de La Neuroimagen en DemenciaDocument22 pagesEl Valor Diagnostico de La Neuroimagen en Demenciajhoel cruzNo ratings yet
- Ryai 210205Document7 pagesRyai 210205Sonia Akter 1064No ratings yet
- Segmentation of Vestibular Schwannoma From MRI, An Open Annotated Dataset and Baseline AlgorithmDocument6 pagesSegmentation of Vestibular Schwannoma From MRI, An Open Annotated Dataset and Baseline AlgorithmIndra PrimaNo ratings yet
- Research Article Robust Blood Cell Image Segmentation Method Based On Neural Ordinary Differential EquationsDocument11 pagesResearch Article Robust Blood Cell Image Segmentation Method Based On Neural Ordinary Differential EquationsSamir GhoualiNo ratings yet
- Terpin Hydrate Oral SolutionDocument1 pageTerpin Hydrate Oral SolutionAbelard Maria EscrivaNo ratings yet
- General ALT Model For Step Stress TestDocument12 pagesGeneral ALT Model For Step Stress TestAnshul NautiyalNo ratings yet
- BrosurDocument68 pagesBrosurKiki Xhui7No ratings yet
- Encapsulation and Inheritance in Object-Orlented Programming LanguagesDocument8 pagesEncapsulation and Inheritance in Object-Orlented Programming Languageszsolt kormanyNo ratings yet
- VSD Power Supply Connections and EarthingDocument4 pagesVSD Power Supply Connections and EarthingHumaid ShaikhNo ratings yet
- IAL Edexcel Pure Math 1 January 2020Document28 pagesIAL Edexcel Pure Math 1 January 2020Mohamed Said Daw100% (4)
- Yanmar Mechnical PumpDocument16 pagesYanmar Mechnical Pump송성훈100% (9)
- Queer Ecology Critique - Georgetown 2014Document104 pagesQueer Ecology Critique - Georgetown 2014Evan JackNo ratings yet
- Communications in Algebra: On The U-Invariant of P-Adic Function FieldsDocument9 pagesCommunications in Algebra: On The U-Invariant of P-Adic Function FieldsKarim ZahidiNo ratings yet
- Fs 1100 Flame Simulator Data Sheet en Us 584524Document4 pagesFs 1100 Flame Simulator Data Sheet en Us 584524Rildon Valqui CiezaNo ratings yet
- Reles, Fuentes, Etc. Catalogo - ABBDocument452 pagesReles, Fuentes, Etc. Catalogo - ABBmpica100% (1)
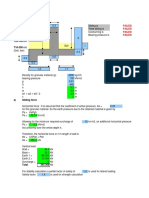
- Sliding, Overturning, Bearing Pressure and Bending Reinforcement Calculations for Retaining WallDocument4 pagesSliding, Overturning, Bearing Pressure and Bending Reinforcement Calculations for Retaining WallAbdul Aziz Julkarnain ZulkifliNo ratings yet
- Radiological Investigations: UltrasonographyDocument42 pagesRadiological Investigations: UltrasonographyDeeptanu GhoshNo ratings yet
- The Image of The CityDocument17 pagesThe Image of The CityMay Rose ParagasNo ratings yet
- Science 8-02.02 - Sensitivity in Living OrganismsDocument9 pagesScience 8-02.02 - Sensitivity in Living OrganismsAnoushia AhmerNo ratings yet
- AbstractDocument2 pagesAbstractramyaNo ratings yet
- Collaboration Processes: Looking Inside the Black BoxDocument13 pagesCollaboration Processes: Looking Inside the Black Boxเข้าใจว่า น่าจะชื่อตุ้นNo ratings yet
- Reverse Phrase Action Camera LightsDocument40 pagesReverse Phrase Action Camera LightsDINDO AzucenaNo ratings yet
- Electronic V-MAC IV Vehicle Mgmt. and Control With Co-Pilot Display Operator ManualDocument133 pagesElectronic V-MAC IV Vehicle Mgmt. and Control With Co-Pilot Display Operator Manualsanach0412No ratings yet
- 09 Exp 11 Buffer SolutionsDocument8 pages09 Exp 11 Buffer SolutionsShainmaugne AdvientoNo ratings yet
- Creme Brulee - Printer Friendly PDFDocument1 pageCreme Brulee - Printer Friendly PDFmtlpcguysNo ratings yet
- Bread and Pastry Production NCII June 10, 2019 - July 03, 2019 ReviewerDocument14 pagesBread and Pastry Production NCII June 10, 2019 - July 03, 2019 ReviewerJames BaculaNo ratings yet
- Tejas: Practice Sheet JEE PhysicsDocument3 pagesTejas: Practice Sheet JEE PhysicsAshree KesarwaniNo ratings yet
- Oxford Reading Tree: The Pet ShopDocument12 pagesOxford Reading Tree: The Pet ShopKanjaNo ratings yet
- Physics Formulas and Symbols: Physics I Symbol FormulaDocument5 pagesPhysics Formulas and Symbols: Physics I Symbol Formulakaparthy100% (9)
- Anchor Systems.: Hilti. Outperform. OutlastDocument49 pagesAnchor Systems.: Hilti. Outperform. Outlastthapa786mNo ratings yet
- 0610 m16 QP 62Document12 pages0610 m16 QP 62faryal khanNo ratings yet
- Amco Veba Marine - Brochure - LRDocument24 pagesAmco Veba Marine - Brochure - LRHươngTpuNo ratings yet
- MD R2 Nastran Release GuideDocument276 pagesMD R2 Nastran Release GuideMSC Nastran BeginnerNo ratings yet
- XR5 9 Element 5 Band Yagi 20-17-15-12-10MDocument16 pagesXR5 9 Element 5 Band Yagi 20-17-15-12-10Msboonuy331No ratings yet
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (14)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 3.5 out of 5 stars3.5/5 (2)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 5 out of 5 stars5/5 (4)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 5 out of 5 stars5/5 (5)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsFrom EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo ratings yet
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (328)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 3.5 out of 5 stars3.5/5 (33)
- Daniel Kahneman's "Thinking Fast and Slow": A Macat AnalysisFrom EverandDaniel Kahneman's "Thinking Fast and Slow": A Macat AnalysisRating: 3.5 out of 5 stars3.5/5 (130)
- Summary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisFrom EverandSummary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisRating: 5 out of 5 stars5/5 (3)