Professional Documents
Culture Documents
Neurological Effects of Iron Supplementation in Infancy
Neurological Effects of Iron Supplementation in Infancy
Uploaded by
Adar LázaroCopyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Neurological Effects of Iron Supplementation in Infancy
Neurological Effects of Iron Supplementation in Infancy
Uploaded by
Adar LázaroCopyright:
Available Formats
Viewpoint
Neurological effects of iron supplementation in infancy:
finding the balance between health and harm in iron-replete
infants
Dominic J Hare, Bárbara Rita Cardoso, Ewa A Szymlek-Gay, Beverley-Ann Biggs
Iron mediates many biochemical processes in neural networks that proliferate during brain development. Insufficient Lancet Child Adolesc Health 2017
iron causes irreversible neurodevelopmental deficits, and most high-income countries recommend that infants older Published Online
than 4–6 months receive additional iron via food fortification or supplementation to prevent iron-deficiency anaemia. December 1, 2017
http://dx.doi.org/10.1016/
Now that the prevalence of iron-deficiency anaemia in children has decreased to less than 10% in most developed
S2352-4642(17)30159-1
countries, concerns that the recommended intakes far exceed those required to prevent iron-deficiency anaemia have
The Florey Institute of
been raised, and emerging evidence suggests that iron overexposure could be linked to adverse outcomes later in life. Neuroscience and Mental
In this Viewpoint, we discuss the importance of iron for neurodevelopment, investigate the biochemical markers Health (D J Hare PhD,
used to assess iron stores, summarise the disparity in public health policies among high-income countries, and B R Cardoso PhD) and
Department of Medicine (Royal
discuss the potential association between iron overexposure and adverse neurological outcomes later in life. We
Melbourne Hospital) at the
present a case for new studies to establish the optimal amount of iron that both prevents deficiency and reduces the Doherty Institute, The
potential risk of long-term negative health outcomes. University of Melbourne,
Parkville, Melbourne, VIC,
Introduction both, in children that are iron replete that prevents iron- Australia (D J Hare,
Prof B-A Biggs PhD); Victorian
Iron-deficiency anaemia, particularly in infancy, can have deficiency anaemia, while mitigating the risk of adverse Infectious Diseases Service,
severe negative health effects. Symptoms include fatigue, neurodevelopmental outcomes later in life. Royal Melbourne Hospital,
headache, paleness, stomatitis, restless legs syndrome, Parkville, Melbourne, VIC,
koilonychia, bowel irritation, and impaired glucose Dietary iron and brain iron concentrations Australia (B-A Biggs); and
Institute for Physical Activity
metabolism.1,2 The burden of disease is high, spanning Several processes that are unique to the brain rely on and Nutrition, School of
lost productivity to infant and maternal mortality.3 Iron is iron redox chemistry (panel 1). Iron concentrations are Exercise and Nutrition
essential for neurodevelopment,4 and policies designed compartmentalised and regulated to prevent reactions Sciences, Deakin University,
Geelong, VIC, Australia
to reduce the prevalence of iron-deficiency anaemia with byproducts of mitochondrial respiration that drive (B R Cardoso,
in children are a crowning achievement of preventive oxidative stress (figure 1). E A Szymlek-Gay PhD)
medicine. However, the effectiveness of iron supplemen Uptake of iron into the brain following blood–brain Correspondence to:
tation appears to be situation dependent, with little barrier maturation has been assumed to be independent Dr Dominic J Hare, The Florey
evidence of the overall benefit in low-income and middle- of dietary iron intake in adults; however, rodent studies8 Institute of Neuroscience and
Mental Health, Parkville, VIC
income countries,5 and even less in Organisation for have shown that iron concentration in the brain increases
3052, Australia
Economic Co-operation and Development (OECD) by about 30% in healthy rats from early adulthood to dominic.hare@florey.edu.au
countries.6 The WHO’s 2016 guideline for iron death, and conservative extrapolation to human beings
supplementation in infants and children7 recommends suggests that the half-life of iron in the brain is in the
supplementing infants for only three consecutive months order of decades.8 The precise age when the blood–brain
a year, and only in areas where the prevalence of anaemia
is greater than 40%. However, the evidence of benefit is
often at odds with public health guidelines on a country- Key messages
by-country basis. • Iron is essential for healthy neurodevelopment, although
Existing policies have received criticism because of overexposure could have adverse long-term health
emerging evidence of negative long-term effects of outcomes
excessive iron exposure during neurodevelopment. WHO • Supplementation or food fortification programmes have For Food Fortification
states that obtaining additional data on the safety of iron been implemented to reduce the prevalence of iron Initiative homepage see
supplementation, including effects in children who do not deficiency and iron-deficiency anaemia in infants
http://www.ffinetwork.org
have anaemia or are not iron deficient, should be a • These supplementation and food fortification policies
research priority.7 In this Viewpoint, we critically appraise vary on a country-by-country basis
the evidence surrounding iron supplementation. • Critical windows during development reflect the dynamic
Highlighting the potential negative outcomes of nature of iron that is needed in the growing brain
overexposure, we emphasise the paucity of compelling • The long-term health outcomes of supplementing
evidence supporting or refuting the need for iron children who are iron replete are unclear
supplementation programmes, necessitating the need to • We advocate for new evidence-based studies to identify
revisit public health policies with new evidence-based appropriate iron intake concentrations that prevent
studies. We propose that a potential middle ground should deficiency while reducing risk of overexposure
be pursued for iron supplementation or fortification, or
www.thelancet.com/child-adolescent Published online December 1, 2017 http://dx.doi.org/10.1016/S2352-4642(17)30159-1 1
Viewpoint
deficiency anaemia does not appear to be associated with
Panel 1: Biochemical function and trafficking of iron in the brain impaired cognitive or motor function in offspring at
• Iron is a cofactor in the enzymes that synthesise the neurotransmitters serotonin, 12 months.18 Evidence supporting the benefits of maternal
γ-aminobutyric-acid (GABA), dopamine, and associated catecholamines iron supplementation during pregnancy is hetero
• Oligodendrocytes are enriched with iron and are responsible for the biosynthesis of geneous19 and larger randomised controlled trials are
myelin sheaths needed.
• Distribution of iron is compartmentalised, with higher concentrations within grey The in-utero environment is anoxic, and an infant is
matter—specifically within the basal ganglia and midbrain born with excess haemoglobin (about 170 g/L) that
• Primary transport of iron across the blood–brain barrier is via transcytosis of the provides sufficient iron for the first 4–6 months of life.
transferrin–transferrin receptor-1 complex from the luminal side of brain capillary Intake of iron from breastmilk (containing <1 mg/L) is
endothelial cells and released into the CNS by divalent metal transporter-1 generally thought to be adequate during this time;
• Astrocytes and other support cells secrete apotransferrin and small ligands that, in although, an apparent absence of iron export from
turn, distribute iron to areas in need, including to neurons via endocytosis of the same mammalian secretory cells has given cause for some to
transferrin receptor complex claim that human breastmilk contains no iron of
• The concentration of iron in the brain that accumulates during normal ageing is nutritional value, and dietary supplementation should be
different depending on the anatomical region of the brain considered.20 On the basis of heterogeneous results
• A likely route of iron export from the brain is via cerebrospinal fluid in the from randomised controlled trials, opinions among
subarachnoid space and eventual return to the bloodstream specialists are conflicting as to whether the neuro
developmental benefits of supplemental iron are
measurable (appendix pp 2–4). For instance, a randomised
See Online for appendix barrier is fully formed is a matter of some debate: studies controlled trial in China21 comparing maternal and
in human beings are scarce, and although the barrier is neonatal iron supplementation found that gross motor-
impermeable to macromolecules at birth, tight junctions function indices improved with treatment after birth,
continue to develop for an unknown period during regardless of intake during pregnancy, whereas a
infancy, enabling diffusion of small molecules into the prospective longitudinal study in Spain22 found that
CNS.9 psychomotor development was more advanced in low-
iron breastfed 6-month-old infants than in mixed-fed
Critical windows for iron and neurodevelopment children who had a higher dietary iron intake. To date, the
In exposure biology, critical windows are periods when best evidence regarding long-term neurodevelopmental
factors such as nutritional deficiency, environmental outcomes in iron-replete infants recommends delayed
exposure, and gut microbiota can influence cord clamping (≥180 sec) to maximise iron transfer,
neurodevelopment. For iron at least three such windows although the benefits are not apparent until the child is
exist, these include: the preconception and in-utero aged 4 years.23
period, when the fetus is dependent on maternal iron The evidence that the behavioural effects of iron
supplies that seed and support neurodevelopment; the deficiency or iron-deficiency anaemia during infancy are
first 6 months of life, when iron is recycled from excess permanent is conflicting. Biochemical studies have
haemoglobin and is essential for myelin synthesis; focused on rodents, and although these provide useful
and the following 6–24 months, when iron-dependent information on neurochemical development, many
neurotransmitter pathways are established (figure 2). An assumptions are extrapolated to human beings.24 A
infant’s brain at birth is approximately a third the volume Cochrane review25 acknowledged that the deleterious
of an adult brain, and it increases by 64% over the first effects of iron-deficiency anaemia on the brain are
3 months,13 and by age 10 years the total iron content of probably irreversible, and yet evidence of the short-term
the brain increases from 10 to 50% of an adult brain’s benefits of iron therapy is absent and the long-term
iron content.14 effects remain unknown. Longitudinal cohort studies26–28
Although we focus on dietary supplementation during have identified associations between iron deficiency and
the window of 6–24 months, the importance of the iron-deficiency anaemia and neurological development,
preceding periods should not be viewed in isolation. although with multiple confounders. For example, iron
Maternal factors including iron deficiency, diabetes, deficiency and iron-deficiency anaemia in infancy were
smoking, intrauterine growth restriction, multiple associated with risk-taking behaviour into adolescence
gestations, and fetal haemorrhage can negatively affect an and poor emotional processing in childhood (attributed
infant’s iron stores at birth.15 Maternal iron and folic acid to stunted development of neurotransmitter pathways)
supplementation reduces mortality and improves infant in a prospective cohort of Chilean children aged 10 and
iron status; although, excessive iron intake is also linked 14 years, controlling for socioeconomic status, home
to gestational diabetes.16 Prenatal iron and folic acid environment, and family stability.26 However, other
improves neurological function in late childhood confounding effects cannot be discounted—eg, chronic
(7–9 years) in countries where iron-deficiency anaemia is inflammation and assessment. Supplementing children
endemic.17 However, maternal iron deficiency or iron- who have iron deficiency or iron-deficiency anaemia
2 www.thelancet.com/child-adolescent Published online December 1, 2017 http://dx.doi.org/10.1016/S2352-4642(17)30159-1
Viewpoint
Duodenum Circulation CNS
Lactotransferrin
from breastmilk Blood–brain barrier
Hepcidin
Iron
Transferrin
Iron-fortified formula
Neurons
Astrocytes
Haem
N N
HO O
Ferritin
Enterocytes
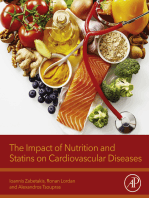
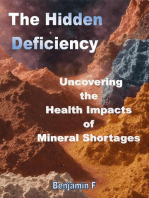
Figure 1: Schematic of dietary iron intake and transit to the CNS
Iron is absorbed in the duodenum from either naturally occurring or fortified products. Once exiting enterocytes, iron is loaded onto transferrin, which distributes
iron around the body. At the blood–brain barrier, iron is imported via transferrin receptor-mediated endocytosis and released into the CNS, reloaded onto transferrin,
and delivered to the various brain regions.
during the 6–24-month period had improved social– anaemia, it increased adverse effects (vomiting, fever)
emotional and behavioural outcomes, but not global and showed no evidence of improved neurodevelopment.29
developmental scores.27 The lead investigator of the
Chilean study described the benefits on motor and Iron deficiency versus iron-deficiency anaemia
cognitive functions as “subtle”,28 and that improved The clinical distinction between iron deficiency and iron-
nutrition in a contemporary Chilean (or other iron- deficiency anaemia is of great importance with respect to
replete) setting could give different results.28 A 2013 clinical management. Bermejo and García-López define
systematic review and meta-analysis29 of daily iron iron deficiency as “the decrease of the total content of
supplementation in children aged 4–23 months found iron in the body” and iron-deficiency anaemia as
that although intervention prevented iron-deficiency “when [iron deficiency] is sufficiently severe to reduce
www.thelancet.com/child-adolescent Published online December 1, 2017 http://dx.doi.org/10.1016/S2352-4642(17)30159-1 3
Viewpoint
Anoxic Oxygen replete More studies on the neurodevelopmental effects of iron
Rapid fetal Neonatal Brain volume expansion deficiency, as opposed to focusing only on iron-deficiency
haemoglobin haemoglobin Proliferation of neurotransmitters anaemia, are necessary to better inform public health
synthesis recycling
policies. The scarcity of well conducted studies that
Blood–brain barrier tight
categorically show iron deficiency causes adverse
Iron concentration
neurodevelopmental outcomes poses the question of
junction closure
whether iron deficiency requires clinical intervention. If
markers of iron deficiency remain stable and an infant
shows no evidence of adverse health effects, iron
supplementation might be unnecessary, and could even
Exclusive lead to long-term negative health outcomes.
breastfeeding Formula or mixed feeding and complementary foods A clinical diagnosis of iron deficiency and iron-
2nd 3rd Birth 6 12 24 deficiency anaemia is established by measuring iron-
Trimesters Age (months)
associated proteins in the blood. The latest guidelines
Iron supplementation and iron-rich diet
Iron supplementation and restricted diet
from the American Academy of Pediatrics (AAP)
Committee on Nutrition11 established a panel of
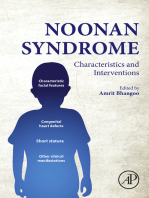
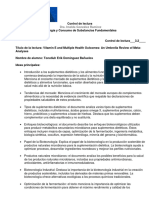
Figure 2: Trajectory of infant iron concentrations and critical windows of neurodevelopment diagnostic biomarkers (panel 2). However, aside from the
Full-term and exclusively breastfed infants with healthy mothers should have similar iron concentrations that
generally accepted cutoff for iron-deficiency anaemia in
diverge when iron rich (formula or complementary solid foods, or both; blue line) or poor (red line) diets are
introduced. Illustrative trajectories of iron intake are based on data from Atkins and colleagues,10 Baker and infants of less than 110 g/L of haemoglobin in the blood,
colleagues,11 Domellöf and colleagues,4 and Ramakrishnan and Yip.12 contention regarding the precise analytical values for
other biomarkers exists as a result of a degree of
erythropoiesis”.30 Iron deficiency affects approximately disconnection between clinicians and biochemists
2 billion people worldwide,31 with iron-deficiency concerning their specific function in maintaining iron
anaemia being the most common cause of anaemia.3 homoeostasis.
Iron-deficiency anaemia is a global health concern, and
policies of iron supplementation or food fortification, or Treating iron deficiency and iron-deficiency
both, have reduced global prevalence of iron-deficiency anaemia in infants
anaemia in children younger than 5 years, with WHO For iron deficiency and iron-deficiency anaemia, iron
data estimating a decrease from 47% in 1995 to 43% in supplementation and fortification of food products
2011; although, the prevalence was only 11% in high- remains a primary point-of-care strategy for addressing
income countries in 2011.32 these conditions in areas of high prevalence—ie, in many
The prevalence of iron deficiency is approximately low-income and middle-income countries.3
double that of iron-deficiency anaemia,33 and iron However, in many high-income countries, fortification
deficiency can be considered as prodromal to iron- of infant formula has been commonplace for decades.
deficiency anaemia, in that iron stores in the body are The Australian Institute for Health and Welfare reports
depleted in the absence of clinical symptoms. Whether that 96% of infants in Australia are initially breastfed, but
iron deficiency is pathological is still under contention, only 39% are exclusively breastfed for longer than
since most studies in human beings have examined 4 months, and 15% for more than 6 months.43 A large
neurodevelopmental deficits only in individuals with iron- cohort study10 in Australia showed that formula accounts
deficiency anaemia, and are often of poor quality. One for 44% of dietary iron intake at age 9 months.
example of a study in which iron deficiency and iron- Guidelines for fortification of infant formula varies
deficiency anaemia were poorly defined was published in between countries. Recommendations published in 2010
1983,34 wherein investigators used a single intramuscular from the AAP Committee on Nutrition to prevent iron
injection of iron to assess behavioural outcomes in infants deficiency and iron-deficiency anaemia in children aged
who were stratified as “iron sufficient”, “iron depleted”, or 0–3 years are shown in panel 3.11 These recommendations
“iron deficient”.34 By modern guidelines, all groups in this incited debate among prominent members of the infant
study would be defined as non-anaemic (haemoglobin nutrition community. Hernell and Lönnerdal44 criticised
levels >110 g/L). Clinical classification was made according the study by Friel and colleagues45 that formed the
to serum ferritin and erythrocyte porphyrin concentrations. groundwork for these recommendations, stating that
Only infants considered as “iron deficient” (ferritin their double-masked randomised controlled trial
<12 µg/L; erythrocyte porphyrin >300 µg/L) showed assessing iron supplementation in healthy breastfed
improvements in the Bayley Mental Development Index, infants was underpowered, and that Friel and colleagues
with “iron depleted” infants (using the same parameters, themselves stated in their report that “A larger study
with erythrocyte porphyrin concentrations <300 µg/L) [ focusing] on the long-term developmental outcomes is
showing no difference after intervention. In a later needed before recommendations can be considered
discussion,35 the same authors used the terms iron regarding the whole population of breast-fed infants.”45
deficiency and iron-deficiency anaemia interchangeably. Hernell and Lönnerdal stated that fortification of infant
4 www.thelancet.com/child-adolescent Published online December 1, 2017 http://dx.doi.org/10.1016/S2352-4642(17)30159-1
Viewpoint
formula with 12 mg/L of iron is unnecessarily high, and
questioned the interpretation of biomarkers used by the Panel 2: The American Academy of Pediatrics Committee on Nutrition’s
investigators. Furthermore, Furman commented that recommended diagnostic biomarkers for iron deficiency and iron-deficiency
calls to supplement exclusively breastfed infants were anaemia11
“premature”,46 and raised concerns regarding the Haemoglobin
supplementation of iron to infants who are iron replete, • Most commonly used clinical biomarker of iron deficiency and iron-deficiency anaemia
noting that information on negative health outcomes was • Diagnosis of iron-deficiency anaemia is defined as haemoglobin <110 g/L at age
available, and advocated for delayed cord clamping to be 6 months to 5 years, <115 g/L at age 6–11 years, and <120 g/L for adults and children
added to the AAP recommendations. The AAP’s own older than 11 years
independent Section on Breastfeeding published in 201047 • Haemoglobin status has low specificity and sensitivity36
noted that they were consulted by Baker, Greer, and the • US National Health and Nutrition Examination Survey III data showed that
Committee on Nutrition before publication of the 2011 haemoglobin was associated with unacceptable levels of false positives and negatives
guidelines,11 but the AAP failed to report that the Section in diagnosing iron deficiency and iron-deficiency anaemia in children37
on Breastfeeding was in disagreement with the overall • Reticulocyte (immature erythrocytes) haemoglobin content indicates iron status
conclusions of the issued recommendation, and had within a 1–2-day period
published their own alternative guidelines in 2009.48 The
Section on Breastfeeding also echoed concerns regarding Transferrin
oversupplementation and risks of long-term negative • An 80 kDa glycoprotein with two iron binding sites
health outcomes. • Iron is loaded onto transferrin by two ferroxidase proteins: ceruloplasmin (circulation)
In response to these comments, Baker and Greer and hephaestin (within intestinal enterocytes)
defended the use of Friel and colleagues’ results to set • Largest contributor to circulating iron concentrations after haemoglobin
guidelines and cited that the paucity of studies assessing • Transferrinsat is the percentage of transferrin binding sites occupied
long-term outcomes did not outweigh benefits: “[i]ron • Acute-phase inflammatory response can cause false-positive iron deficiency or
deficiency occurs long before there is overt an[a]emia and iron-deficiency anaemia diagnoses
may have long-lasting consequences. Because of the very • Clinical assays of transferrinsat are imprecise and have poor sensitivity to small
low iron content of human milk, exclusively breastfed changes38
infants are at risk of iron deficiency. Supplementing Transferrin receptor-1
breastfed infants would protect them; why put these • A regulator of evolutionarily conserved iron uptake and transport mechanisms;
infants at any risk when no appreciable harm of iron transcription and expression dictated by cellular iron concentrations
supplementation has been convincingly demonstrated?”49 • Serum transferrin receptor-1 combined with other markers improves the diagnostic
Since the AAP’s guidelines were first released, a accuracy of iron deficiency and iron-deficiency anaemia, and can distinguish between
randomised controlled trial of iron supplementation iron-deficiency anaemia and non-iron-deficiency aneamia39
(1 mg/kg per day as an additive to breastmilk or formula)
including an iron-replete patient group focusing on Serum ferritin
psychomotor and mental development outcomes has • High-capacity storage protein capable of binding up to 4500 iron atoms
commenced (NCT02242188), and the Benefits and Risks • Not synthesised in serum, rarely saturated, and iron load across multiple human
of Iron interventionS in Children (BRISC) trial in individuals is very variable40
Bangladesh (ACTRN12617000660381) has been registered. • No clinically approved assays for ferritin saturation exist, and serum ferritin
Hernell and Lönnerdal’s reply44 to the AAP cited studies concentration is typically used as a proxy for iron concentration
from Europe, where recommendations on iron • Contribution to circulating iron is small compared with haemoglobin or transferrin
supplementation are more conservative. The position of (approximately 5% of transferrin iron)
the European Society for Paediatric Gastroenterology, • A major inflammatory response protein and should be assessed in concert with other
Hepatology and Nutrition (ESPGHAN; panel 4)4 includes inflammatory markers
comprehensive definitions of iron deficiency and iron- Hepcidin
deficiency anaemia. Notably, when ESPGHAN formed • Proposed master regulator of iron homoeostasis
an international advisory group and released their global • Synthesised by the liver (and to a lesser extent in the brain) to inhibit cellular iron
standard for infant formula composition, one member export41
withdrew support for the proposed range of iron • Strong antimicrobial properties and acute-phase inflammatory response factor
fortification levels (0·3–1·3 mg per 100 kcal for cow milk • Accurate analytical assays for clinical translation still require validation42
formula; 0·45–2·0 mg per 100 kcal for soy) on the basis
of them being too low per the standards of their national
advisory body. A subsequent Mead Johnson Pediatric group”.51 Although the panel’s recommendations still
Nutrition Institute Iron Expert Panel meeting in advocated fortification of infant formulas, they suggested
November, 2014, reported that “panel members were in concentrations be more in line with the ESPHGAN
agreement that the current levels of iron fortification of guidelines, and reflected the changing attitudes with
infant formulas in the US are not optimal and do not respect to iron exposure during critical windows of
reflect current evidence for iron requirements in this age neurodevelopment.
www.thelancet.com/child-adolescent Published online December 1, 2017 http://dx.doi.org/10.1016/S2352-4642(17)30159-1 5
Viewpoint
Iron intake concentrations in other high-income
Panel 3: Summary of the American Academy of Pediatrics Committee on Nutrition countries that have specific policies in place tend to
recommendations for iron intake in children and infants11 fall somewhere between the AAP and ESPHGAN
• Full-term infants who are exclusively breastfed beyond age 4 months are at risk of recommendations, or have no set guidelines (appendix
iron deficiency, and should receive oral iron at a dose of 1 mg/kg until complementary p 5). In the UK, infant formulas average at 6 mg/L of
foods are introduced, including iron-fortified cereals iron and follow-on formulas at 10 mg/L of iron.52
• Infants aged 0–12 months receive an adequate iron supply from a commercial Australia does not specify a value for all formulas (Food
formula, which contains 10–12 mg/L in the USA; from 4–6 months complementary Standards Australia and New Zealand advise
foods, including iron-fortified cereals, should be introduced 5·5–13·6 mg/L for follow-on formulas, which is under
• Iron intake between ages 6 and 12 months should be 11 mg/day, sourced from both review), but states that, at around 6 months, “[t]o prevent
fortified and naturally iron-rich foods. iron deficiency, iron-containing nutritious foods are
• Infants aged 1–3 years should receive 7 mg/day of iron, primarily through iron-rich recommended to be included in the first foods.”53 This
foods, including red meat, vegetables, and fruits that are rich in vitamin C, which statement is important, since increasing iron intake
promotes iron absorption in the gut; if this diet cannot be provided, oral supplements from complementary foods is often not accounted for
can be given up to age 3 years, and chewable vitamin preparations should be added when guidelines for iron supplementation are set
beyond this age (figure 2). Japan has no policy on the iron fortification of
• Preterm infants require additional iron (2 mg/kg per day) up to age 12 months and formula54 and has substantially higher rates of long-term
weaning to iron-fortified infant formula is recommended breastfeeding than other high-income countries.55
• Assessment for iron deficiency and iron-deficiency anaemia should be done at age
12 months, primarily assessed by measuring haemoglobin concentrations and, if risk Does the chemical state of iron matter?
of iron deficiency or iron-deficiency anaemia is indicated, other biomarkers listed in The iron in human breastmilk is primarily bound to
panel 2 should be measured lactotransferrin, with a smaller contribution from ferritin
and α-lactalbumin. Relative to protein-bound iron,
breastmilk contains very little inorganic iron.
Lactotransferrin has a normal concentration range of
2–3 g/L in human breastmilk and reaches 7 g/L in
colostrum, equating to around 0·35 mg/L of iron. Infant
Panel 4: Summary of ESPGHAN statements and recommendations on iron intake in
formulas are typically fortified with inorganic iron at
children and infants4
higher concentrations. We did an extensive review56 of
• Iron absorption in infants is generally low, but endogenous response mechanisms the reported iron concentrations in breastmilk and
might increase intake when dietary iron concentrations are low fortified formulas, and showed that iron-fortified milk
• Iron-deficiency anaemia causes long-lasting neurodevelopmental deficits, but iron substitutes contained, on average, around 20 times more
overexposure is also associated with stunted growth, increased infection risk, and iron than normal breastmilk.
potential neurodevelopmental deficits; evidence of neurodevelopmental benefits of The difference in chemical state is one of the primary
supplementation is conflicting justifications given by the AAP in their 2010 recom
• ESPGHAN recommendations are more moderate than those of the AAP’s Committee mendations,11 citing a Committee on Nutrition report57
on Nutrition; they state that no convincing evidence is available to support that claimed that more than 50% of the iron in breastmilk
supplementation in full-term breastfed infants up to age 6 months is absorbed in the infant gut, whereas less than 12% of
• In European pregnant women, iron supplementation does not seem to have had an inorganic iron added to bovine-derived formulas is
effect on neonatal iron status absorbed. These figures are not referenced, and the
• Delayed cord clamping improves iron status in neonates source of this information in the committee report is
• Formula-fed infants who are aged 0–6 months should receive 2·0–8·5 mg/L of iron, unknown. More comprehensive studies58,59 have assessed
and little evidence supports setting an optimal concentration range for follow-on differential uptake of inorganic iron versus protein-
(>6 months) formulas bound iron from breastmilk, although the expense of
• Iron supplementation does not reduce the proportion of infants with iron-deficiency small-scale trials using isotope tracing has resulted in
anaemia in populations with low (<5–10%) prevalence at age 6 months, although considerable disparity in reported uptakes. In one
neurodevelopment might be improved in formula-fed infants under 6 months; study,58 investigators used an isotopic tracer in both
however, this supplementation strategy does prevent iron-deficiency anaemia in normal unfortified breastmilk and breastmilk fortified
infants who are aged 6–12 months with iron, and found that the uptake of iron in infants at
• Introduction of naturally iron-rich complementary foods at age 4–12 months prevents age 6 months was the same (at approximately 16%) for
iron-deficiency anaemia, and treatment with supplements from age 4–12 months are both milks, with absorption from unfortified breastmilk
only effective in populations with high (>10%) prevalence of iron-deficiency anaemia only increasing to around 30% at age 9 months. A
• The European Union has a non-binding directive with a suggested range for iron of similar study59 with formula fortified with α-lactalbumin
3·6–14·0 mg/L50 and casein-glycomacropeptide to promote iron
absorption, showed no significant difference in iron
AAP=American Academy of Pediatrics. ESPGHAN=European Society for Paediatric Gastroenterology,
Hepatology and Nutrition.
uptake between formula preparations and breastmilk. A
study60 in which investigators used an iron isotope tracer
6 www.thelancet.com/child-adolescent Published online December 1, 2017 http://dx.doi.org/10.1016/S2352-4642(17)30159-1
Viewpoint
to measure iron uptake in human adult erythrocytes most comprehensive systematic review67 to date reported
from natural and simulated breastmilk, as well as that treating zinc deficiency with supplementation does
formulas, showed 15% of the iron from natural human not affect iron status, whereas randomised controlled
breastmilk was found in red blood cells, compared with trials of cosupplementation were mostly observational
less than 10% of iron from simulated breastmilk and (eg, increasing zinc dose was not associated with iron
less than 5% of iron from infant formulas. The authors deficiency) and could not resolve discordance in the
noted that erythrocyte uptake represented 80% of the literature regarding potential adverse effects on clinical
absorbed iron in the participants, with the fate of the outcomes related to iron deficiency and iron-deficiency
remaining 20% unknown. Higher concentrations of anaemia.
iron in formula results in a greater net uptake than from
human breastmilk, even though iron in breastmilk is Iron fortification and natural sources
more bioavailable than that in infant formula. The One of the most common so-called first foods, along with
addition of lactotransferrin into infant formulas could fruits and vegetables, is infant cereals, which are
better reflect the chemical form of iron in breastmilk, routinely fortified with inorganic iron. If a formula-fed
and rodent studies have shown that fortification with infant continues on a mixed diet that includes a
apo-lactotransferrin and inorganic iron increases total component of infant formula, this additional source
absorption.61 Similar effects, including responses from could further add to the bioavailable iron consumed. In
iron-store biomarkers, were observed in exclusively an Australian study, 9-month-old infants received 28% of
breastfed infants supplemented with milk that contained their dietary iron intake from specific infant and toddler
lactotransferrin.62 A compensatory effect is apparent on food products excluding formula,10 many of which are
iron uptake when lactotransferrin is added to formulas, fortified with iron. Australia does not mandate iron
as was found by Hernell and Lönnerdal,63 with the fortification of cereals, although voluntary addition is
addition of bovine lactotransferrin to infant formula commonplace in foods marketed for infants. In toddlers
containing 2–4 mg/L of inorganic iron showing no effect (older than 20 months) their primary iron source shifts
on circulating iron concentrations. This trial did make to cereal products (eg, flour, grains) that are consumed by
other important observations, including that 20 (34%) of the general population, which accounted for 43% of their
59 participants (who were aged <6 months) had total iron intake.10 This transition to foods that are not
haemoglobin concentrations below 110 g/L at the end of infant specific substantially changes the amount of
the study, and yet showed no symptoms of iron- dietary iron to which a growing child is exposed.
deficiency anaemia, leading the authors to suggest that Accurately assessing the total dietary iron intake of a
the haemoglobin cutoff for iron-deficiency anaemia was toddler is clearly a challenging task.
too high. Additionally, formula containing 1·6 mg/L of Fortification of infant formulas has successfully
iron was sufficient to meet the health needs of a reduced the prevalence of iron deficiency and iron-
6-month-old infant, a concentration that is less than 10% deficiency anaemia in infants and children in high-
of the AAP recommendation. A larger-scale trial by the income countries, although this policy was preceded by
same researchers comparing low-iron infant formula the fortification of wheat, maize, and rice with iron
(ie, lactotransferrin sourced) with high (inorganic) iron to address iron-deficiency anaemia in the general
formula is underway (NCT02103205). population. The American Medical Association adopted
a policy of iron fortification in 1936.68 Both the USA and
Interactions between iron and other minerals the UK have a compulsory iron fortification of flour,
Few high-quality studies have been done on the effects Australia maintains a voluntary programme of
of iron supplementation on infants when taken fortification, and countries including Norway, Denmark,
as a multivitamin or mineral preparation,64 with and Sweden prohibited iron fortification in the mid-to-
most randomised controlled trials focused on the late 20th century. Denmark and Sweden cited the
administration of micronutrient mixtures to pregnant absence of evidence that fortification with iron reduced
women. Compounds such as phytates and oxalates form total prevalence of iron-deficiency anaemia, and that
stable complexes with iron in the gastrointestinal tract potential adverse health effects dictated their directive.
and prevent the uptake of non-haem iron, whereas Before this prohibition, Sweden had the highest flour
calcium appears to inhibit the release of iron from fortification levels (65 mg/kg) of any country.69
enterocytes into the circulatory system.65 Experimental Longitudinal studies following the prohibition of iron
assessment of how multiple nutrients at a range of doses fortification have shown that the prevalence of iron-
effect not only health outcomes but also iron uptake is a deficiency anaemia is steady, whereas disease
challenging task and is likely to be pieced together from progression of hereditary haemochromatosis, which
individual studies and settings. For instance, data are has a significantly higher frequency in Scandinavian
conflicting as to whether coadministration of zinc and populations, has slowed.69,70
iron results in the competitive uptake of the two divalent The AAP’s guidelines list recommended foods for
metals, and the effects appear to be dose dependent.66 The boosting iron concentrations,11 with estimated elemental
www.thelancet.com/child-adolescent Published online December 1, 2017 http://dx.doi.org/10.1016/S2352-4642(17)30159-1 7
Viewpoint
iron content per serving. Excluding fortified products, disease in areas with poor hygiene and sanitation. Jaeggi
haem-containing foods are the richest source of iron. and colleagues77 supported this concept in a randomised
Introduction of haem-rich meat undoubtedly has a controlled trial of iron-fortified porridge that they fed to
substantial effect on iron stores, since absorption of Kenyan infants with iron-deficiency anaemia for
haem is more efficient than inorganic iron. Haem is 4 months. They found that children that were fed both
transported across the duodenum via an independent the low (2·5 mg iron per day, as a ferric sodium ethylene
transporter.71 Although haem-containing foods are diaminetetraacetate [NaFeEDTA] micronutrient powder)
consumed in smaller amounts, the iron is two to three and high iron (12·5 mg per day, as a ferrous fumarate
times more bioavailable than inorganic iron and micronutrient powder) showed a significant increase in
absorption is not affected by other chemicals.72 pathological bacteria in the gastrointestinal tract. A
subsequent randomised controlled trial78 in the same
Risks and negative health outcomes in setting found that the delivery of iron as an equimolar
iron-supplemented infants and children mixture of NaFeEDTA and ferrous fumarate micro
Short-term adverse health effects nutrient powder totalling 5 mg per day, with the inactive
Iron supplementation can cause adverse health events, maltodextrin component of the preparation replaced
even in populations that are clinically anaemic. In her with probiotic galacto-oligosaccharides, decreased iron-
overview of clinical, pathological, and therapeutic aspects deficiency anaemia by 50% without adversely affecting
of iron-deficiency anaemia, Camaschella33 identified the gut microbiome when compared with children who
nausea, vomiting, constipation, and dysgeusia as the were receiving the equivalent 5 mg of iron alone.
most common acute side-effects of iron supplementation. A long-standing concern regarding iron supple
Intravenous iron therapy has a similar side-effect profile, mentation has been the potential risk in areas where
in addition to pruritus, myalgia, and other localised malaria is endemic. The WHO’s guidelines for daily iron
sources of pain.73 A systematic review and meta-analysis29 supplementation7 state that strong, high-quality evidence
on infants aged 4–23 months receiving direct supple exists to support iron supplementation only in
mentation reported increased risk ratios for vomiting conjunction with measures to prevent, diagnose, and
and fever (which could be antecedent to infection), treat malaria.7 If in place, surveillance and treatment
regardless of whether the recipients had anaemia or were services should ensure the risk of infection is not
iron replete; although, the authors noted that higher- increased in children who are supplemented with iron.29
powered studies are needed to confirm the adverse effect Delaying the administration of supplemental iron to
profiles. children with malaria who had anaemia until 28 days
The chemical state of the iron supplement does after the administration of antimalarial therapies did not
appear to influence its side-effect profile. A systematic affect their overall response in a randomised controlled
review74 of adverse events in 111 trials of supplementation trial in Uganda,79 since at 56 days after treatment their
with various preparations of iron found that extended- replenishment of iron stores was not substantially
release ferrous sulfate with mucoproteose was best different to those who started antimalarial drugs and
tolerated, whereas ferrous fumarate was associated with supplemental iron treatment concurrently.79
the highest proportion of reported adverse events. Pasricha and colleagues29 did not identify an association
Although hetero geneity in the data precluded meta- between iron supplementation and respiratory tract
analysis, the large sample size (n >10 000) allowed the infections. Other factors could contribute to reduced
authors to state the limitations of the trials that were infection risk—eg, combined administration of iron with
studied while still reporting their findings with a high long-chain polyunsaturated fatty acids has inherent anti-
degree of confidence. inflammatory properties80 and lactotransferrin is
antimicrobial.81 A large randomised controlled trial
Iron supplementation and infection in Pakistan82 found a strong association between iron
Consideration should also be given to the adverse effects supplementation of infants who were aged 6–18 months
of iron intervention studies, particularly considering that and incidence of diarrhoea, as well as some respiratory
iron depletion can protect against microbial pathogens.75 difficulties.
A particularly interesting perspective was described by
Quinn,76 who hypothesised that the depletion of iron Effects on growth
stores in an infant at age 6 months could in fact be a The AAP and ESPGHAN both acknowledge that
conserved evolutionary mechanism to restrict the access iron stores are adequate during the first 4–6 months
of pathogenic microbiota to iron. Quinn posited that of life of a full-term infant, and thus
introduction of iron-fortified formulas after the age of iron supplementation is unnecessary. The AAP also
6 months could undermine this adaptive mechanism acknowledges that iron overload can occur as a result of
that has been in place long before both the agricultural excessive intake, although it did not discuss the
revolution and introduction of fortification programmes, potential adverse effects when issuing their guidelines
and could result in an increased risk of gastrointestinal for infants and children.11 Conversely, the recommen
8 www.thelancet.com/child-adolescent Published online December 1, 2017 http://dx.doi.org/10.1016/S2352-4642(17)30159-1
Viewpoint
dations of ESPGHAN state: “Because high iron intakes reported an association between fetal iron status and
may have adverse effects in iron-replete infants, it is mental and psychomotor development at age 5 years,
important to identify iron requirements in young with both low and high iron status correlating with poor
children and to identify risk groups that benefit from full-scale intelligence quotient testing.
higher iron intakes.”4 Infants who have severe anaemia and receive iron
One of the most studied outcomes of supplementation supplementation still show signs of poor developmental
during infancy is the effect on growth. A review83 of and behavioural outcomes 10 years after intervention.91
26 randomised controlled trials involving children aged Follow-up studies such as these are the most powerful
0–59 months identified a negative effect on weight when tool for assessing the possible neurological effects of iron
children who were iron replete were supplemented, and supplementation, although tracing cohorts over an
inconclusive evidence that iron supplementation affected extended period of time can be a costly and lengthy
height. A systematic review and meta-analysis84 of exercise. Lozoff and colleagues28 revisited a randomised
21 randomised controlled trials in infants, children, controlled trial of iron supplementation of Chilean
and adolescents, and seven in pregnant women, showed infants without anaemia who were given high
no measurable benefit of iron intervention on a range (12·7 mg/L) or low (2·3 mg/L) iron-fortified formula. Of
of infant growth markers. A subsequent randomised the original population, 473 (57%) of 835 Chilean infants
controlled trial85 done in marginally low-birthweight were assessed at 10 years. In every measured category of
infants who were supplemented with iron from neuro development, the high-iron formula group
0–6 months did not find any measurable effects performed more poorly than the low-iron group,
on anthropometric measures; whereas, a randomised although not in global development scores.27 Clearly the
controlled trial86 that focused primarily on children who loss of over 40% of the study population to follow-up
were iron replete indicated that excess iron intake retarded restricts the conclusions that can be drawn from this
growth. Although somewhat paradoxical, considering the study, and the authors acknowledged that high variance
importance of iron for growth and development, evidence in haemoglobin concentrations restricted analytical
suggests that iron supplementation has little effect (on power in each comparison group and warned against
growth) regardless of whether an infant is iron deficient or making changes in practice on the basis of these results
replete, and could in fact be detrimental when in excess.4 In alone.
particular, more attention should be paid to both beneficial An increased rate of iron accumulation in the brain
and adverse health effects of supplementation to infants beyond that of normal ageing has been linked to the
who have sufficient iron stores.6 development of some neurodegenerative diseases.56
Localised iron-induced oxidative stress can result in
Effects on neurodevelopment chronic and irreversible neuron death.92 We have
In contrast to the understanding of iron deficiency and hypothesised that early-life dietary iron overexposure
iron-deficiency anaemia and neurodevelopment,87 could be a risk factor for such neurodegenerative
relatively little is known about the acute health effects of diseases,56 and that the excessive fortification of foods to
iron overload on the developing brain. In 2005, Georgieff which infants are exposed creates an unnecessary risk of
and Innis wrote: “No study has convincingly developing diseases with few treatment options. The
demonstrated that nutritional iron overload contributes long-standing association between brain iron
to adverse neurodevelopment in preterm infants”88—a accumulation and Parkinson’s disease has resulted in
comment that could be extended to full-term infants. more attention being paid to potential sources that
However, a study by Buonocore and colleagues89 of increase iron in the brains of individuals with this
infants who had birth asphyxia showed that the non- condition. The primary concern is that, in the infant gut
transferrin-bound iron content of blood was an extremely and brain, adequate feedback mechanisms that limit
effective marker for neurodevelopmental outcomes, with excessive iron uptake might not be properly developed.
high concentrations (>849 µg/L) related to neurodisability, In a reply to the recommendations set by the AAP,
measured by in-vivo imaging of ischaemic damage and Furman46 cited the trial by Domellöf and colleagues93 that
the Bayley Scales of Infant Development. The authors showed iron absorption did not influence haemoglobin
speculated that, in addition to being a suitable predictive concentrations, stating that “it seems that 4- to
marker for poor neurodevelopmental outcomes, the high 6-month-olds will absorb the additional iron they receive
concentrations of non-transferrin-bound iron were also regardless of whether they need it”.
contributing to CNS injury by enhancing oxidative stress
and damage to lipid membranes. Is iron supplementation during infancy a risk factor for
The potential for iron-mediated brain injury begins in neurodegeneration?
utero. The placenta ensures the fetus has adequate access We previously56,94 proposed that overexposure of infants
to iron even when maternal iron deficiency is present, to iron during the 6–24 month critical window of
although little is known about how the placenta responds iron-dependent neurodevelopment gives a so-called head
to maternal iron overload. Tamura and colleagues90 start to natural iron accumulation, which could become
www.thelancet.com/child-adolescent Published online December 1, 2017 http://dx.doi.org/10.1016/S2352-4642(17)30159-1 9
Viewpoint
Panel 5: Lessons from genetic disorders that feature iron overload Panel 6: Insights into the role of iron from animal studies
• Patients with heterozygous hereditary haemochromatosis (caused by the mutated • Mice orally supplmented with 40 times the typical iron
HFE gene) do not typically show evidence of iron overload, but do absorb more iron in concentrations of mouse milk during 10–17 days
the gut than usual; homozygotes manifest symptoms of iron overload; diagnosis of postpartum (equivalent to the first 12 months in human
hereditary haemochromatosis in infants and children is rare, since iron deposition that neonates)—reflecting the proportional difference
is substantial enough to cause pathology can take many years; symptoms include between human breastmilk and the AAP’s
growth retardation, lactic acidosis, aminoaciduria, and hypotransferrinaemia and the recommendations—showed increased concentrations of
associated effects on erythropoiesis, although effects on the immature brain are iron in the substantia nigra pars compacta (the primary
unclear site of neurodegeneration in Parkinson’s disease) from
• Juvenile haemochromatosis is a pathologically distinct condition resulting from 2 months, oxidative stress at 12 months, and
mutations to either the HFE2 gene encoding haemojuvelin or the HAMP gene dopamine-specific cell loss from 16 months95
encoding hepcidin • Evidence suggests a synergistic relationship between iron
• Neonatal haemochromatosis is phenotypically similar to juvenile haemochromatosis; concentration in the brain and the Parkinson’s
however, iron deposition occurs at a faster rate, resulting in rapid liver failure, disease-associated protein α-synuclien;96 iron
stillbirth, death during the immediate postnatal period, or the urgent need for a liver supplementation to both wild-type mice and mice
transplant; it is not associated with an HFE mutation, and the direct cause is unknown; expressing the Ala53Thr mutation of α-synuclien with
liver failure typically precedes neurological symptoms impaired dopamine metabolism was sufficient to cause
• Early-onset, rapidly progressing neurodegeneration with brain iron accumulation that increased concentrations of iron in the brain and nigral
occurs in childhood causes parkinsonism and associated movement disorders cell loss at age 8–12 months
• Transfusion-dependent thalassaemias, particularly in mothers and pregnant women, • Chronic treatment of mice with the iron chelator
require careful management to prevent the potential negative effects of iron overload in clioquinol at age 5 months was unable to arrest extensive
the fetus and neonate; the different thalassaemias have similar symptomatic profiles, in age-related neurodegeneration, even though clioquinol
addition to an increased risk of diabetes, splenomegaly, cardiomyopathy, returned the concentration of iron in the brain to
hyperthyroidism, and pulmonary hypertension; thalassaemias are often misdiagnosed as baseline, indicating that α-synuclien and iron exert
iron-deficiency anaemia, and thus the risks of iron supplementation can be substantial neurotoxic effects before therapeutic intervention
• Most association studies between genetic disorders of iron overload and
AAP=American Academy of Pediatrics
neurodegeneration have focused only on the frequency of mutations; studies are
needed that directly assess iron status, concentrations of iron in the brain, and the
prevalence of neurodegeneration in populations with inherited disorders, particularly
in whom iron overload is well managed as a preventive treatment, and at-risk patients with
high brain iron concentrations resulting from high
dietary iron exposure could benefit from short courses
pathological when the individual is 60 years or older, of treatment with the chelator to reduce iron
substantially increasing the risk of Parkinson’s disease. accumulation to the baseline concentrations of normal
Iron turnover in the brain is slow and concentrations ageing.94
increase with age.56 Much can be learned about iron
overload and the effects exerted on the brain from genetic Conclusion
disorders (panel 5), and although these disorders are an As the collective understanding of iron biochemistry
acute response to iron overload, they provide important grew throughout the 20th century, the importance of
For WHO Nutrition homepage clues to what deleterious effects iron overload can have, maintaning an iron-replete biological system became
see http://www.who.int/
particularly during ageing. apparent, with awareness of the role of nutrition and
nutrition/en
Animal studies have provided important insight into signs and symptoms of anaemia increasing worldwide.
For WHO Anaemia Health Topic
page see http://www.who.int/
the biochemical mechanisms of iron storage and Accordingly, ensuring that a population has sufficient
topics/anaemia/en/ dyshomoeostasis in neurodegenerative disorders, access to dietary iron is an ongoing public health
particularly Parkinson’s disease, as well as potential endeavour. However, unlike other essential
therapies to reduce brain iron concentrations (panel 6). micronutrients that have well described toxic effects
The pilot trial by Devos and colleagues97 showed that when in excess, such as manganese and selenium, the
the strong chelator deferiprone reduced the potential toxicity of dietary iron overload is not often
concentration of iron in the brains of a neurotoxin considered. Furthermore, following the commentary of
mouse-model of parkinsonism and human beings with experts in the field about the AAP Committee on
early-stage Parkinson’s disease, with the human group Nutrition’s most recent recommendations for preventing
also showing marked improvement in the Unified iron deficiency and iron-deficiency anaemia, signs are
Parkinson’s Disease Rating Scale. This work preceded encouraging that the guidelines will be revisited and that
the commencement of the FAIRPARK II phase 2 trial new and thorough clinical trials in infants who are iron
of deferiprone (NCT02728843). If FAIRPARK II proves replete will take place in line with the recommendations
to be successful, deferiprone could potentially be given of WHO.7
10 www.thelancet.com/child-adolescent Published online December 1, 2017 http://dx.doi.org/10.1016/S2352-4642(17)30159-1
Viewpoint
4 Domellöf M, Braegger C, Campoy C, et al. Iron requirements of
Search strategy and selection criteria infants and toddlers. J Pediatr Gastroenterol Nutr 2014; 58: 119–29.
5 Pasricha S-R, Drakesmith H, Black J, Hipgrave D, Biggs B-A.
We identified references for this Viewpoint through searches Control of iron deficiency anemia in low- and middle-income
of PubMed and Google Scholar with the search terms “iron countries. Blood 2013; 121: 2607–17.
supplementation”, “iron fortification”, “iron deficiency an[a] 6 Krebs NF, Domellöf M, Ziegler E. Balancing benefits and risks of
iron fortification in resource-rich countries. J Pediatr 2015;
emia”, “brain iron”, and related terms from Jan 1, 1900, to 167 (suppl 4): S20–25.
June 30, 2017. Articles were also identified through searches 7 WHO. WHO guideline: daily iron supplementation in infants and
of the authors’ own collections. Only papers published in children. Geneva: World Health Organization, 2016. http://apps.
who.int/iris/bitstream/10665/204712/1/9789241549523_eng.
English were reviewed. The final reference list was generated pdf?ua=1&ua=1 (accessed Oct 26, 2017).
on the basis of originality and relevance to the broad scope of 8 Chen J-H, Singh N, Tay H, Walczyk T. Imbalance of iron influx and
this Viewpoint. efflux causes brain iron accumulation over time in the healthy adult
rat. Metallomics 2014; 6: 1417–26.
9 Jones HC, Keep RF, Butt AM. The development of ion regulation at
the blood-brain barrier. Prog Brain Res 1992; 91: 123–31.
The evidence we have presented in this Viewpoint 10 Atkins LA, McNaughton SA, Campbell KJ, Szymlek-Gay EA. Iron
gives added justification for re-examining public health intakes of Australian infants and toddlers: findings from the
Melbourne Infant Feeding, Activity and Nutrition Trial (InFANT)
approaches to treating iron deficiency and iron-deficiency Program. Br J Nutr 2016; 115: 285–93.
anaemia (if indeed iron deficiency needs intervention). 11 Baker RD, Greer FR, Committee on Nutrition American Academy
Fortification is certainly more economically viable, but of Pediatrics. Diagnosis and prevention of iron deficiency and
iron-deficiency anemia in infants and young children (0–3 years of
with it comes the added risk of negative health outcomes age). Pediatrics 2010; 126: 1040–50.
in children who are iron replete. Supplementation on a 12 Ramakrishnan U, Yip R. Experiences and challenges in
case-by-case basis, using a comprehensive panel of industrialized countries: control of iron deficiency in industrialized
countries. J Nutr 2002; 132 (suppl 4): 820S–24.
biomarkers of iron-deficiency anaemia, would probably
13 Holland D, Chang L, Ernst TM, et al. Structural growth trajectories
be a more effective means for disease mitigation without and rates of change in the first 3 months of infant brain
the added risk, although the economic implications development. JAMA Neurol 2014; 71: 1266–74.
would need to be considered. Whether the withdrawal of 14 Leibel RL, Greenfield DB, Pollitt E. Iron deficiency: behavior
and brain biochemistry In: Winick M, ed. Nutrition: pre-
food-fortification programmes can offset the cost of and postnatal development. New York, NY: Springer,
clinical screening in infants and children suspected of 1979: 383–439.
being iron deficient is yet to be fully assessed. What is 15 Rao R, Georgieff MK. Iron in fetal and neonatal nutrition.
Semin Fetal Neonatal Med 2007; 12: 54–63.
clear from the evidence presented here is that little
16 Scholl TO. Iron status during pregnancy: setting the stage for
consensus exists on what the precise benefits and mother and infant. Am J Clin Nutr 2005; 81: 1218S–22S.
potential harms of iron supplementation are; numerous 17 Christian P, Murray-Kolb LE, Khatry SK, et al. Prenatal
studies have identified a benefit in settings where iron- micronutrient supplementation and intellectual and motor
function in early school-aged children in Nepal. JAMA 2010;
deficiency anaemia is endemic, in terms of restoring 304: 2716–23.
haematological markers to those considered acceptable 18 Mireku MO, Davidson LL, Boivin MJ, et al. Prenatal iron deficiency,
(panel 2), although the effects on neurodevelopment are neonatal ferritin, and infant cognitive function. Pediatrics 2016;
138: e20161319.
not as obvious. Iron is crucial for neurodevelopment, 19 Alwan NA, Hamamy H. Maternal iron status in pregnancy and
although direct intervention has become somewhat long-term health outcomes in the offspring. J Pediatr Genet 2015;
controversial, and will remain so until further large-scale 4: 111–23.
longitudinal trials are able to categorically confirm or 20 Cai C, Eck P, Friel JK. Gene expression profiles suggest iron
transport pathway in the lactating human epithelial cell.
refute long-term benefits. J Pediatr Gastroenterol Nutr 2017; 64: 460–64.
Contributors 21 Angulo-Barroso RM, Li M, Santos D, et al. Iron supplementation in
DJH conceived and drafted the manuscript. BRC, EAS-G and B-AB pregnancy or infancy and motor development: a randomized
contributed to, edited, and approved the final version of the manuscript. controlled trial. Pediatrics 2016; 137: e20153547.
22 Jardí C, Hernández-Martínez C, Canals J, et al. Influence of
Declaration of interests breastfeeding and iron status on mental and psychomotor
DJH reports grants from the Australian National Health and Medical development during the first year of life. Infant Behav Dev 2017;
Research Council during the conduct of this study; and grants and published online June 5. DOI:10.1016/j.infbeh.2017.05.009.
materials support from Agilent Technologies and the Australian 23 Andersson O, Lindquist B, Lindgren M, Stjernqvist K, Domellöf M,
Research Council outside the submitted work. All other authors declare Hellström-Westas L. Effect of delayed cord clamping on
no competing interests. neurodevelopment at 4 years of age: a randomized clinical trial.
JAMA Pediatr 2015; 169: 631–38.
Acknowledgments 24 Georgieff MK. Long-term brain and behavioral consequences of
The Florey Institute acknowledges the Victorian Government’s early iron deficiency. Nutr Rev 2011; 69 (suppl 1): S43–48.
Operational Infrastructure Support Program. 25 Wang B, Zhan S, Gong T, Lee L. Iron therapy for improving
References psychomotor development and cognitive function in children under
1 Lopez A, Cacoub P, Macdougall IC, Peyrin-Biroulet L. Iron the age of three with iron deficiency anaemia.
deficiency anaemia. Lancet 2016; 387: 907–16. Cochrane Database Syst Rev 2013; 6: CD001444.
2 Soliman AT, De Sanctis V, Yassin M, Soliman N. Iron deficiency 26 East P, Delker E, Lozoff B, Delva J, Castillo M, Gahagan S.
anemia and glucose metabolism. Acta Biomed 2017; 88: 112–18. Associations among infant iron deficiency, childhood
3 Kassebaum NJ, Jasrasaria R, Naghavi M, et al. A systematic analysis emotion and attention regulation, and adolescent problem
of global anemia burden from 1990 to 2010. Blood 2014; 123: 615–24. behaviors. Child Dev 2017; publsihed online Feb 23. DOI:10.1111/
cdev.12765.
www.thelancet.com/child-adolescent Published online December 1, 2017 http://dx.doi.org/10.1016/S2352-4642(17)30159-1 11
Viewpoint
27 Lozoff B, De Andraca I, Castillo M, Smith JB, Walter T, Pino P. 51 Kleinman RE. Expert recommendations on iron fortification in
Behavioral and developmental effects of preventing iron-deficiency infants. J Pediatr 2015; 167 (suppl 4): S48–49.
anemia in healthy full-term infants. Pediatrics 2003; 112: 846–54. 52 Crawley H, Westland S. Infant milks in the UK: a practical guide for
28 Lozoff B, Castillo M, Clark KM, Smith JB. Iron-fortified vs low-iron health professionals—August 2017. First Steps Nutrition Trust, 2013.
infant formula: developmental outcome at 10 years. http://www.firststepsnutrition.org/pdfs/Infant_Milks_August2017.
Arch Pediatr Adolesc Med 2012; 166: 208–15. pdf (accessed Oct 16, 2017).
29 Pasricha S-R, Hayes E, Kalumba K, Biggs B-A. Effect of daily iron 53 Australian Government. National Health and Medical Research
supplementation on health in children aged 4–23 months: Council (2012). Eat for health. Infant feeding guidelines: summary.
a systematic review and meta-analysis of randomised controlled Canberra: National Health and Medical Research Institute, 2013.
trials. Lancet Glob Health 2013; 1: e77–86. 54 Isomura H, Takimoto H, Miura F, et al. Type of milk feeding affects
30 Bermejo F, García-López S. A guide to diagnosis of iron deficiency hematological parameters and serum lipid profile in Japanese
and iron deficiency anemia in digestive diseases. infants. Pediatr Int 2011; 53: 807–13.
World J Gastroenterol 2009; 15: 4638–43. 55 Inoue M, Binns CW, Otsuka K, Jimba M, Matsubara M. Infant
31 McLean E, Cogswell M, Egli I, Wojdyla D, de Benoist M. Worldwide feeding practices and breastfeeding duration in Japan: a
prevalence of anaemia, WHO Vitamin and Mineral Nurition review. Int Breastfeed J 2012; 7: 15.
Information System, 1993-2005. Public Health Nutr 2009; 56 Hare DJ, Arora M, Jenkins NL, Finkelstein DI, Doble PA, Bush AI.
12: 444–554. Is early-life iron exposure critical in neurodegeneration?
32 Stevens GA, Finucane MM, De-Regil LM, et al. Global, regional, Nat Rev Neurol 2015; 11: 536–44.
and national trends in haemoglobin concentration and prevalence 57 Committee on Nutrition. Iron fortification of infant formulas.
of total and severe anaemia in children and pregnant and American Academy of Pediatrics Committee on Nutrition. Pediatrics
non-pregnant women for 1995–2011: a systematic analysis of 1999; 104: 119–23.
population-representative data. Lancet Global Health 2013; 58 Domellöf M, Lönnerdal B, Abrams SA, Hernell O. Iron absorption
1: e16–e25. in breast-fed infants: effects of age, iron status, iron supplements,
33 Camaschella C. Iron-deficiency anemia. N Engl J Med 2015; and complementary foods. Am J Clin Nutr 2002; 76: 198–204.
372: 1832–43. 59 Szymlek-Gay EA, Lönnerdal B, Abrams SA, Kvistgaard AS,
34 Oski FA, Honig AS, Helu B, Howanitz P. Effect of iron therapy on Domellöf M, Hernell O. α-Lactalbumin and
behavior performance in nonanemic, iron-deficient infants. casein-glycomacropeptide do not affect iron absorption from
Pediatrics 1983; 71: 877–80. formula in healthy term infants. J Nutr 2012; 142: 1226–31.
35 Oski FA. Iron deficiency in infancy and childhood. N Engl J Med 60 McMillan JA, Oski FA, Lourie G, Tomarelli RM, Landaw SA.
1993; 329: 190–93. Iron absorption from human milk, simulated human milk,
36 Zimmermann MB, Hurrell RF. Nutritional iron deficiency. Lancet and proprietary formulas. Pediatrics 1977; 60: 896–900.
2007; 370: 511–20. 61 Fernández-Menéndez S, Fernández-Sánchez ML,
37 White KC. Anemia is a poor predictor of iron deficiency among González-Iglesias H, Fernández-Colomer B, López-Sastre J,
toddlers in the United States: for heme the bell tolls. Pediatrics 2005; Sanz-Medel A. Iron bioavailability from supplemented formula
115: 315–20. milk: effect of lactoferrin addition. Eur J Nutr 2017; 56: 2611–20.
38 Hare DJ, Doecke JD, Faux NG, et al. Decreased plasma iron in 62 Ke C, Lan Z, Hua L, et al. Iron metabolism in infants: influence of
Alzheimer’s disease is due to transferrin desaturation. bovine lactoferrin from iron-fortified formula. Nutrition 2015;
ACS Chem Neurosci 2015; 6: 398–402. 31: 304–09.
39 Kohgo Y, Torimoto Y, Kato J. Transferrin receptor in tissue and 63 Hernell O, Lönnerdal B. Iron status of infants fed low-iron formula:
serum: updated clinical significance of soluble receptor. no effect of added bovine lactoferrin or nucleotides. Am J Clin Nutr
Int J Hematol 2002; 76: 213–18. 2002; 76: 858–64.
40 Konz T, Añón-Alvarez E, Montes-Bayón M, Sanz-Medel A. 64 Rautiainen S, Manson JE, Lichtenstein AH, Sesso HD.
Antibody labeling and elemental mass spectrometry (inductively Dietary supplements and disease prevention—a global overview.
coupled plasma-mass spectrometry) using isotope dilution for Nat Rev Endocrinol 2016; 12: 407–20.
highly sensitive ferritin determination and iron-ferritin ratio 65 Lönnerdal B. Calcium and iron absorption—mechanisms and
measurements. Anal Chem 2013; 85: 8334–40. public health relevance. Int J Vitam Nutr Res 2010; 80: 293–99.
41 Hare DJ. Hepcidin: a real-time biomarker of iron need. Metallomics 66 Bjørklund G, Aaseth J, Skalny AV, et al. Interactions of iron with
2017; 9: 606–18. manganese, zinc, chromium, and selenium as related to
42 Kroot JJ, van Herwaarden AE, Tjalsma H, Jansen RT, prophylaxis and treatment of iron deficiency. J Trace Elem Med Biol
Hendriks JC, Swinkels DW. Second round robin for plasma 2017; 41: 41–53.
hepcidin methods: first steps toward harmonization. 67 Mayo-Wilson E, Imdad A, Junior J, Dean S, Bhutta ZA.
Am J Hematol 2012; 87: 977–83. Preventive zinc supplementation for children, and the effect of
43 Australian Government. Australian Institute of Health and Welfare. additional iron: a systematic review and meta-analysis. BMJ Open
2010 Australian national infant feeding survey. Canberra: Australian 2014; 4: e004647.
Institute for Health and Welfare, 2011. 68 Bishai D, Nalubola R. The history of food fortification in the
44 Hernell O, Lönnerdal B. Recommendations on iron questioned. United States: its relevance for current fortification efforts in
Pediatrics 2011; 127: e1099–101. developing countries. Econ Devel Cult Change 2002; 51: 37–53.
45 Friel JK, Aziz K, Andrews WL, Harding SV, Courage ML, Adams RJ. 69 Olsson KS, Väisänen M, Konar J, Bruce Å. The effect of withdrawal
A double-masked, randomized control trial of iron supplementation of food iron fortification in Sweden as studied with phlebotomy in
in early infancy in healthy term breast-fed infants. J Pediatr 2003; subjects with genetic hemochromatosis. Eur J Clin Nutr 1997;
143: 582–86. 51: 782–86.
46 Furman LM. Exclusively breastfed infants: iron recommendations 70 Milman N, Pedersen P, Steig T, Melsen GV. Frequencies of the
are premature. Pediatrics 2011; 127: e1098–99. hereditary hemochromatosis allele in different populations.
47 Schanler RJ, Feldman-Winter L, Landers S, et al. Concerns with Comparison of previous phenotypic methods and novel genotypic
early universal iron supplementation of breastfeeding infants. methods. Int J Hematol 2003; 77: 48–54.
Pediatrics 2011; 127: e1097. 71 Shayeghi M, Latunde-Dada GO, Oakhill JS, et al. Identification of
48 Kleinman RE, American Academy of Pediatrics, Committee on an intestinal heme transporter. Cell 2005; 122: 789–801.
Nutrition. Pediatric nutrition handbook, 6th edn. Elk Grove Village, 72 Pizarro F, Olivares M, Valenzuela C, et al. The effect of proteins
IL: American Academy of Pediatrics, 2009. from animal source foods on heme iron bioavailability in humans.
49 Baker RD, Greer FR. In reply. Pediatrics 2011; 127: e1101–04. Food Chem 2016; 196: 733–38.
50 European Commission Directive 2006/141/EC of 22 December 2006 73 Auerbach M, Strauss W, Auerbach S, Rineer S, Bahrain H. Safety
on infant formulae and follow-on formulae and amending Directive and efficacy of total dose infusion of 1,020 mg of ferumoxytol
1999/21/EC. OJ L 2006; 401: 1–33. administered over 15 min. Am J Hematol 2013; 88: 944–47.
12 www.thelancet.com/child-adolescent Published online December 1, 2017 http://dx.doi.org/10.1016/S2352-4642(17)30159-1
Viewpoint
74 Cancelo-Hidalgo MJ, Castelo-Branco C, Palacios S, et al. 85 Berglund SK, Westrup B, Domellöf M. Iron supplementation until
Tolerability of different oral iron supplements: a systematic review. 6 months protects marginally low-birth-weight infants from iron
Curr Med Res Opin 2013; 29: 291–303. deficiency during their first year of life. J Pediatr Gastroenterol Nutr
75 Ganz T, Nemeth E. Iron homeostasis in host defence and 2015; 60: 390–95.
inflammation. Nat Rev Immunol 2015; 15: 500–10. 86 Idjradinata P, Watkins WE, Pollitt E. Adverse effect of iron
76 Quinn EA. Too much of a good thing: evolutionary perspectives on supplementation on weight gain of iron-replete young children.
infant formula fortification in the United States and its effects on Lancet 1994; 343: 1252–54.
infant health. Am J Hum Biol 2013; 26: 10–17. 87 Lozoff B, Jimenez E, Wolf AW. Long-term developmental outcome
77 Jaeggi T, Kortman GA, Moretti D, et al. Iron fortification adversely of infants with iron deficiency. N Engl J Med 1991; 325: 687–94.
affects the gut microbiome, increases pathogen abundance and 88 Georgieff MK, Innis SM. Controversial nutrients that potentially
induces intestinal inflammation in Kenyan infants. Gut 2015; affect preterm neurodevelopment: essential fatty acids and iron.
64: 731–42. Pediatr Res 2005; 57: 99R–103R.
78 Paganini D, Uyoga MA, Kortman GAM, et al. Prebiotic 89 Buonocore G, Perrone S, Longini M, et al. Non protein bound iron
galacto-oligosaccharides mitigate the adverse effects of iron as early predictive marker of neonatal brain damage. Brain 2003;
fortification on the gut microbiome: a randomised controlled study 126: 1224–30.
in Kenyan infants. Gut 2017; 66: 1956–67. 90 Tamura T, Goldenberg RL, Hou J, et al. Cord serum ferritin
79 Cusick SE, Opoka RO, Abrams SA, John CC, Georgieff MK, concentrations and mental and psychomotor development of
Mupere E. Delaying iron therapy until 28 days after antimalarial children at five years of age. J Pediatr 2002; 140: 165–70.
treatment is associated with greater iron incorporation and 91 Lozoff B, Jimenez E, Hagen J, Mollen E, Wolf AW. Poorer behavioral
equivalent hematologic recovery after 56 days in children: and developmental outcome more than 10 years after treatment for
a randomized controlled trial. J Nutr 2016; 146: 1769–74. iron deficiency in infancy. Pediatrics 2000; 105: E51.
80 Malan L, Baumgartner J, Zandberg L, Calder PC, Smuts CM. 92 Hare DJ, Double KL. Iron and dopamine: a toxic couple. Brain 2016;
Iron and a mixture of DHA and EPA supplementation, alone and in 139: 1026–35.
combination, affect bioactive lipid signalling and morbidity of iron 93 Domellöf M, Cohen RJ, Dewey KG, Hernell O, Rivera LL,
deficient South African school children in a two-by-two randomised Lönnerdal B. Iron supplementation of breast-fed Honduran and
controlled trial. Prostaglandins Leukot Essent Fatty Acids 2016; Swedish infants from 4 to 9 months of age. J Pediatr 2001;
105: 15–25. 138: 679–87.
81 Chen K, Chai L, Li H, et al. Effect of bovine lactoferrin from 94 Hare DJ, Cardoso BR, Raven EP, et al. Excessive early-life dietary
iron-fortified formulas on diarrhea and respiratory tract infections exposure: a potential source of elevated brain iron and a risk factor
of weaned infants in a randomized controlled trial. Nutrition 2016; for Parkinson’s disease. NPJ Parkinsons Dis 2017; 3: 1–5.
32: 222–27.
95 Kaur D, Peng J, Chinta SJ, et al. Increased murine neonatal iron
82 Soofi S, Cousens S, Iqbal SP, et al. Effect of provision of daily zinc intake results in Parkinson-like neurodegeneration with age.
and iron with several micronutrients on growth and morbidity Neurobiol Aging 2007; 28: 907–13.
among young children in Pakistan: a cluster-randomised trial.
96 Billings JL, Hare DJ, Nurjono M, et al. Effects of neonatal iron
Lancet 2013; 382: 29–40.
feeding and chronic clioquinol administration on the parkinsonian
83 Iannotti LL, Tielsch JM, Black MM, Black RE. Iron supplementation human A53T transgenic mouse. ACS Chem Neurosci 2016;
in early childhood: health benefits and risks. Am J Clin Nutr 2006; 7: 360–66.
84: 1261–76.
97 Devos D, Moreau C, Devedjian JC, et al. Targeting chelatable iron as
84 Vucic V, Berti C, Vollhardt C, et al. Effect of iron intervention on a therapeutic modality in Parkinson’s disease. Antiox Redox Signal
growth during gestation, infancy, childhood, and adolescence: 2014; 21: 195–210.
a systematic review with meta-analysis. Nutr Rev 2013; 71: 386–401.
www.thelancet.com/child-adolescent Published online December 1, 2017 http://dx.doi.org/10.1016/S2352-4642(17)30159-1 13
You might also like
- Men's Muscle & Health - August 2015 AUDocument140 pagesMen's Muscle & Health - August 2015 AUZoltán DánNo ratings yet
- Lean Bulk E BookDocument25 pagesLean Bulk E BookChuts100% (5)
- Molecular Mechanisms of Dementia: Biomarkers, Neurochemistry, and TherapyFrom EverandMolecular Mechanisms of Dementia: Biomarkers, Neurochemistry, and TherapyNo ratings yet
- The Man Diet-FINAL+Document194 pagesThe Man Diet-FINAL+Jaime GarNo ratings yet
- Dysphagia: Foundation, Theory and PracticeFrom EverandDysphagia: Foundation, Theory and PracticeJulie A. Y. CicheroNo ratings yet
- Folic Acid (Vitamin B9), A Simple Guide To The Vitamin, Functions And DeficiencyFrom EverandFolic Acid (Vitamin B9), A Simple Guide To The Vitamin, Functions And DeficiencyRating: 5 out of 5 stars5/5 (1)
- Soal Latihan Bahasa InggrisDocument20 pagesSoal Latihan Bahasa Inggrislina marlina50% (2)
- The Impact of Nutrition and Statins on Cardiovascular DiseasesFrom EverandThe Impact of Nutrition and Statins on Cardiovascular DiseasesNo ratings yet
- Developing Brain Behaviour: The Role of Lipids in Infant FormulaFrom EverandDeveloping Brain Behaviour: The Role of Lipids in Infant FormulaNo ratings yet
- Noonan Syndrome: Characteristics and InterventionsFrom EverandNoonan Syndrome: Characteristics and InterventionsAmrit P.S. BhangooNo ratings yet
- Nutrigenetics: Applying the Science of Personal NutritionFrom EverandNutrigenetics: Applying the Science of Personal NutritionRating: 4.5 out of 5 stars4.5/5 (3)
- Advances in Pathobiology and Management of Paget’s Disease of BoneFrom EverandAdvances in Pathobiology and Management of Paget’s Disease of BoneSakamuri V. ReddyNo ratings yet
- Link Iso 13485 - 21cfr 820Document7 pagesLink Iso 13485 - 21cfr 820Phan ChaugiangNo ratings yet
- Autism Reversal ToolboxDocument15 pagesAutism Reversal ToolboxLazaf KilamNo ratings yet
- Thiamine Deficiency Disease, Dysautonomia, and High Calorie MalnutritionFrom EverandThiamine Deficiency Disease, Dysautonomia, and High Calorie MalnutritionRating: 4.5 out of 5 stars4.5/5 (5)
- Parkinson’s Disease Therapeutics: Emphasis on Nanotechnological AdvancesFrom EverandParkinson’s Disease Therapeutics: Emphasis on Nanotechnological AdvancesNo ratings yet
- Summary of Mark P. Mattson's The Intermittent Fasting RevolutionFrom EverandSummary of Mark P. Mattson's The Intermittent Fasting RevolutionRating: 5 out of 5 stars5/5 (1)
- Building Bone Vitality: A Revolutionary Diet Plan to Prevent Bone Loss and Reverse Osteoporosis--Without Dairy Foods, Calcium, Estrogen, or DrugsFrom EverandBuilding Bone Vitality: A Revolutionary Diet Plan to Prevent Bone Loss and Reverse Osteoporosis--Without Dairy Foods, Calcium, Estrogen, or DrugsRating: 4.5 out of 5 stars4.5/5 (7)
- The Placenta and Neurodisability 2nd EditionFrom EverandThe Placenta and Neurodisability 2nd EditionIan CrockerNo ratings yet
- Living with Spina Bifida: A Guide for Families and ProfessionalsFrom EverandLiving with Spina Bifida: A Guide for Families and ProfessionalsRating: 5 out of 5 stars5/5 (1)
- Modelo de IndiceDocument1 pageModelo de Indiceedmark9271549No ratings yet
- Molecular Nutrition and Genomics: Nutrition and the Ascent of HumankindFrom EverandMolecular Nutrition and Genomics: Nutrition and the Ascent of HumankindNo ratings yet
- Epigenomics in Health and DiseaseFrom EverandEpigenomics in Health and DiseaseMario FragaNo ratings yet
- Gentle Detox: The Natural Detoxification ProgramFrom EverandGentle Detox: The Natural Detoxification ProgramNo ratings yet
- Practical Pediatric Endocrinology in a Limited Resource SettingFrom EverandPractical Pediatric Endocrinology in a Limited Resource SettingMargaret ZacharinRating: 5 out of 5 stars5/5 (1)
- Neurotoxic Metals affecting Autism / Aspergers Syndrome / ADHD: Booklet 2From EverandNeurotoxic Metals affecting Autism / Aspergers Syndrome / ADHD: Booklet 2No ratings yet
- Cognitive Development in Anemic Infants of Different PrakritiFrom EverandCognitive Development in Anemic Infants of Different PrakritiNo ratings yet
- Disorders of the Spinal Cord in ChildrenFrom EverandDisorders of the Spinal Cord in ChildrenMichael PikeNo ratings yet
- Malnutrition in the ElderlyFrom EverandMalnutrition in the ElderlyW.O. SeilerNo ratings yet
- Fluid and Electrolytes in Pediatrics: A Comprehensive HandbookFrom EverandFluid and Electrolytes in Pediatrics: A Comprehensive HandbookNo ratings yet
- Human Milk: Composition, Clinical Benefits and Future Opportunities: 90th Nestlé Nutrition Institute Workshop, Lausanne, October-November 2017From EverandHuman Milk: Composition, Clinical Benefits and Future Opportunities: 90th Nestlé Nutrition Institute Workshop, Lausanne, October-November 2017No ratings yet
- Environmental Causes and Prevention Measures for Alzheimer’s DiseaseFrom EverandEnvironmental Causes and Prevention Measures for Alzheimer’s DiseaseNo ratings yet
- Nutrition for Healthy Hair: Guide to Understanding and Proper PracticeFrom EverandNutrition for Healthy Hair: Guide to Understanding and Proper PracticeNo ratings yet
- The Prevention and Treatment of Disease with a Plant-Based Diet Volume 2: Evidence-based articles to guide the physicianFrom EverandThe Prevention and Treatment of Disease with a Plant-Based Diet Volume 2: Evidence-based articles to guide the physicianNo ratings yet
- Current Topics in BiochemistryFrom EverandCurrent Topics in BiochemistryC.B. AnfinsenNo ratings yet
- A Practical Approach to Adolescent Bone Health: A Guide for the Primary Care ProviderFrom EverandA Practical Approach to Adolescent Bone Health: A Guide for the Primary Care ProviderSarah PittsNo ratings yet
- Molecular, Cellular, and Metabolic Fundamentals of Human AgingFrom EverandMolecular, Cellular, and Metabolic Fundamentals of Human AgingNo ratings yet
- Management of Wilson Disease: A Pocket GuideFrom EverandManagement of Wilson Disease: A Pocket GuideMichael L. SchilskyNo ratings yet
- Complementary and Alternative Medical Lab Testing Part 1: EENT (Eyes, Ears, Nose and Throat)From EverandComplementary and Alternative Medical Lab Testing Part 1: EENT (Eyes, Ears, Nose and Throat)No ratings yet
- The Hidden Deficiency Uncovering the Health Impacts of Mineral ShortagesFrom EverandThe Hidden Deficiency Uncovering the Health Impacts of Mineral ShortagesNo ratings yet
- Etiologia EnfisemaDocument3 pagesEtiologia Enfisemaedmark9271549No ratings yet
- Semiologia de Aparato PsicomotorDocument78 pagesSemiologia de Aparato Psicomotoredmark9271549100% (1)
- LaringitisDocument59 pagesLaringitisedmark9271549100% (1)
- AutomatizacionDocument8 pagesAutomatizacionedmark9271549No ratings yet
- Construccion de Carreteras TécnicasDocument8 pagesConstruccion de Carreteras Técnicasedmark9271549No ratings yet
- Segundo Trabajo en ArchivoDocument37 pagesSegundo Trabajo en Archivoedmark9271549No ratings yet
- European Best Practice Guidelines For Haemodialysis (Part 2) PDFDocument43 pagesEuropean Best Practice Guidelines For Haemodialysis (Part 2) PDFВладимир Ильич ЛенинNo ratings yet
- Etude Bibliographique Sur La Reglementation de La Vente Des Plantes Medicinales en Algerie Compares Au Reste Du MondeDocument87 pagesEtude Bibliographique Sur La Reglementation de La Vente Des Plantes Medicinales en Algerie Compares Au Reste Du MondeAnaïs Célia BoudaoudNo ratings yet
- Guía Del Participante NUTRILITEDocument68 pagesGuía Del Participante NUTRILITEJanna Terrones100% (1)
- Bill Starr - Q&A (Power Clean)Document4 pagesBill Starr - Q&A (Power Clean)TomSusNo ratings yet
- SUPLEMENTACION DEPORTIVA - Nutricion DeportivaDocument3 pagesSUPLEMENTACION DEPORTIVA - Nutricion DeportivaSantiago Diaz LopezNo ratings yet
- Do You Believe in Magic by Paul A. Offit, MDDocument5 pagesDo You Believe in Magic by Paul A. Offit, MDsimasNo ratings yet
- SantalubbyDocument10 pagesSantalubbyMark Cruze100% (1)
- Sheep NutritionDocument1 pageSheep NutritionRhibNo ratings yet
- Migraine Cause and TreatmentDocument4 pagesMigraine Cause and TreatmentSorin PalcuNo ratings yet
- Forging An Anaemia Free Future 2018Document8 pagesForging An Anaemia Free Future 2018shreya kaleNo ratings yet
- Facts of The CaseDocument4 pagesFacts of The CasetanNo ratings yet
- NUTRICOSMETICOS - Legislação - BrasilDocument3 pagesNUTRICOSMETICOS - Legislação - BrasilDotressus MmokNo ratings yet
- Cockroach (Periplaneta Americana) : Nutritional Value As Food and Feed For Man and LivestockDocument11 pagesCockroach (Periplaneta Americana) : Nutritional Value As Food and Feed For Man and LivestockJibrinNo ratings yet
- Health Characteristics of Older Australian Dietary Supplement Users Compared To Non-Supplement UsersDocument8 pagesHealth Characteristics of Older Australian Dietary Supplement Users Compared To Non-Supplement UsersDeff HaningNo ratings yet
- Free Shipping - AmwayDocument14 pagesFree Shipping - Amwayjaymarshall3No ratings yet
- Alerta - TONIPONTE - TÓNICO CEREBRALDocument4 pagesAlerta - TONIPONTE - TÓNICO CEREBRALJmad JohanaNo ratings yet
- Folletos NEX02-1Document2 pagesFolletos NEX02-1Copiadora EconocopiasNo ratings yet
- Fulvic AcidDocument2 pagesFulvic AcidNatalia NeliNo ratings yet
- English Project Subject and Verb AgreementDocument6 pagesEnglish Project Subject and Verb AgreementArianne Faye de GuzmanNo ratings yet
- NUTR2002 Human Nutrition 2Document14 pagesNUTR2002 Human Nutrition 2Ben LagatNo ratings yet
- Altrum Nutritional Catalog - Multi-Vitamin, Mineral, Herbal, Superfood SupplementsDocument28 pagesAltrum Nutritional Catalog - Multi-Vitamin, Mineral, Herbal, Superfood Supplementsaltrum_dealerNo ratings yet
- Latihan Soal Ukk Bahasa Inggris Kelas 9 SMP k13Document9 pagesLatihan Soal Ukk Bahasa Inggris Kelas 9 SMP k13Hapsari C. Hanandya NannaNo ratings yet
- Control de Lectura 3.3UAM-EyCSFDocument3 pagesControl de Lectura 3.3UAM-EyCSFTontiuh Erik Domínguez BañuelosNo ratings yet