You might also like
- Treating Trichotillomania - Cognitive-Behavioral Therapy For Hairpulling and Related Problems PDFDocument211 pagesTreating Trichotillomania - Cognitive-Behavioral Therapy For Hairpulling and Related Problems PDFAlessandro Papa100% (2)
- Search Engine Marketing Course Material 2t4d9Document165 pagesSearch Engine Marketing Course Material 2t4d9Yoga Guru100% (2)
- Designing A Polarity Therapy ProtocolDocument12 pagesDesigning A Polarity Therapy ProtocolTariq J FaridiNo ratings yet
- Andromeda Council About The 4th DimensionDocument11 pagesAndromeda Council About The 4th DimensionWonderlust100% (1)
- Map Project Rubric 2018Document2 pagesMap Project Rubric 2018api-292774341No ratings yet
- Encyclopedia of Behavioral Medicine 9783030399016 303039901x 9783030399023 3030399028 - CompressDocument2,457 pagesEncyclopedia of Behavioral Medicine 9783030399016 303039901x 9783030399023 3030399028 - CompressHilda FadhilahNo ratings yet
- Massage Therapy EffectsDocument12 pagesMassage Therapy EffectsEkalevi FahlepieNo ratings yet
- Palpation in CranioSacral Therapy and Other ModalitiesDocument10 pagesPalpation in CranioSacral Therapy and Other Modalitieskabshiel100% (1)
- Accupuncture Needle DepthDocument21 pagesAccupuncture Needle DepthStephen T LeNo ratings yet
- D41P-6 Kepb002901Document387 pagesD41P-6 Kepb002901LuzioNeto100% (1)
- The Biological Action of Physical Medicine: Controlling the Human Body's Information SystemFrom EverandThe Biological Action of Physical Medicine: Controlling the Human Body's Information SystemNo ratings yet
- Benedetti F. Placebo and The New Physiology of The Doctor-Patient RelationshipDocument40 pagesBenedetti F. Placebo and The New Physiology of The Doctor-Patient Relationshippuntocom11No ratings yet
- Rhetorical Analysis Final-1 4Document6 pagesRhetorical Analysis Final-1 4api-666378857No ratings yet
- Winter's Bracing Approach RevisitedDocument5 pagesWinter's Bracing Approach RevisitedJitendraNo ratings yet
- Therapeutic TouchDocument2 pagesTherapeutic TouchnieotyagiNo ratings yet
- Meehan 1998Document9 pagesMeehan 1998Asriyani HamidNo ratings yet
- A Model For Standardised Documentation in Manual and Massage TherapyDocument7 pagesA Model For Standardised Documentation in Manual and Massage TherapyAnandhu GNo ratings yet
- A Review of Torque Release Technique®Document5 pagesA Review of Torque Release Technique®Ed RibeiroNo ratings yet
- Journal Aplikasi Teori DosseyDocument11 pagesJournal Aplikasi Teori DosseyAnonymous RWUSkCprNo ratings yet
- Terapia Manual Coluna JosptDocument6 pagesTerapia Manual Coluna JosptBia DiasNo ratings yet
- Dry Needling: A Literature Review With Implications For Clinical Practice GuidelinesDocument15 pagesDry Needling: A Literature Review With Implications For Clinical Practice Guidelinesabe lapianNo ratings yet
- Manual Therapy: Neil Langridge, Lisa Roberts, Catherine PopeDocument6 pagesManual Therapy: Neil Langridge, Lisa Roberts, Catherine PopeVizaNo ratings yet
- Prescribing Therapeutic Interventions Through Strategic Treatment SelectionDocument17 pagesPrescribing Therapeutic Interventions Through Strategic Treatment SelectionCentro integral del desarrollo LogrosNo ratings yet
- Joyce 1990Document9 pagesJoyce 1990cs18No ratings yet
- Ultrasound and Laser As Stand-Alone Therapies For Myofascial Trigger Points: A Randomized, Double-Blind, Placebo-Controlled StudyDocument10 pagesUltrasound and Laser As Stand-Alone Therapies For Myofascial Trigger Points: A Randomized, Double-Blind, Placebo-Controlled StudyVikborn TjgNo ratings yet
- The Relationship Between Rate of Algometer Application and Pain Pressure Threshold in TheDocument16 pagesThe Relationship Between Rate of Algometer Application and Pain Pressure Threshold in TheRafael BohnenbergerNo ratings yet
- Sopa de Siglas para El Toc (Act, Epr, CBT)Document9 pagesSopa de Siglas para El Toc (Act, Epr, CBT)Guiliana ValdiviesoNo ratings yet
- Tt10 Kelly AeDocument8 pagesTt10 Kelly AeSoulyogaNo ratings yet
- The Science of Hand TherapyDocument1 pageThe Science of Hand TherapyrayjongsNo ratings yet
- Therapist Interpretation, Patient-Therapist Interpersonal Process, and Outcome in Psychodynamic Psychotherapy For Avoidant Personality DisorderDocument18 pagesTherapist Interpretation, Patient-Therapist Interpersonal Process, and Outcome in Psychodynamic Psychotherapy For Avoidant Personality DisorderPamela Cortés PeñaNo ratings yet
- 14 Ingles PDFDocument112 pages14 Ingles PDFJonathan gAguirre MendozaNo ratings yet
- Nicholls 1996 Objectivity in Physiotherapy AssessmentDocument2 pagesNicholls 1996 Objectivity in Physiotherapy AssessmentGamalia MartaNo ratings yet
- What's Therapeutic About The Therapeutic MilieuDocument9 pagesWhat's Therapeutic About The Therapeutic MilieuEfren FerrerNo ratings yet
- Integrative therapy in ICUDocument8 pagesIntegrative therapy in ICUTassia CamposNo ratings yet
- Therapeutic - Touch Principles and PracticeDocument3 pagesTherapeutic - Touch Principles and PracticejesusmonNo ratings yet
- Listen To Patient and CollagueDocument2 pagesListen To Patient and CollagueVITRIA NOVITA SARINo ratings yet
- Dedo en Gatillo 2Document9 pagesDedo en Gatillo 2Paulina Rodriguez MontelongoNo ratings yet
- Semiology As A Scientific Basis For The Theory of Medicine and PsychiatryDocument1 pageSemiology As A Scientific Basis For The Theory of Medicine and PsychiatryBiblioteca ICSN - Clínica MontserratNo ratings yet
- Empirically Supported Complexity: Rethinking Evidence-Based Practice in PsychotherapyDocument6 pagesEmpirically Supported Complexity: Rethinking Evidence-Based Practice in PsychotherapyPedro VargasNo ratings yet
- Effectiveness of Physical Therapy in Patients With Tension-Type Headache: Literature ReviewDocument8 pagesEffectiveness of Physical Therapy in Patients With Tension-Type Headache: Literature Reviewratnayanti udinNo ratings yet
- Psychotherapy Research: Please Scroll Down For ArticleDocument15 pagesPsychotherapy Research: Please Scroll Down For ArticleJoana Maestra CuturaNo ratings yet
- Aric Vrnada 2Document18 pagesAric Vrnada 2Indra GunawanNo ratings yet
- Clinical Reasoning in Medicine: Practice and EducationDocument28 pagesClinical Reasoning in Medicine: Practice and EducationOmar Azaña VelezNo ratings yet
- Patient and Therapist Introject, Interpersonal Process, and Differential Psychotherapy OutcomeDocument7 pagesPatient and Therapist Introject, Interpersonal Process, and Differential Psychotherapy OutcomeCristhiAldorNo ratings yet
- Raciocinio EticoDocument17 pagesRaciocinio EticoPatrícia PaqueteNo ratings yet
- Milieu Therapy For Short Stay Units: A Transformed Practice TheoryDocument9 pagesMilieu Therapy For Short Stay Units: A Transformed Practice TheoryAlejandra AvilaNo ratings yet
- EH - Patients and Clinicians Opinions - Final CBTDocument24 pagesEH - Patients and Clinicians Opinions - Final CBTMihaela-Claudia NedelceaNo ratings yet
- Gold FriedDocument10 pagesGold FriedPamela Cortés PeñaNo ratings yet
- The Art of Holding HandsDocument8 pagesThe Art of Holding HandsIbrahim Alex Mazur ScotchNo ratings yet
- Accepted Manuscript: 10.1016/j.ijosm.2016.05.003Document25 pagesAccepted Manuscript: 10.1016/j.ijosm.2016.05.003yoverNo ratings yet
- Integrando Terapia Manual e Neurociencia Da DorDocument274 pagesIntegrando Terapia Manual e Neurociencia Da DorÁtila HanemannNo ratings yet
- An Experimental Analysis of Clinical Phenomenn C. B. FersterDocument16 pagesAn Experimental Analysis of Clinical Phenomenn C. B. FersterJuan Alberto GonzálezNo ratings yet
- Texto 2012 Book Reviewj.2042-7166.2011.01107.xDocument6 pagesTexto 2012 Book Reviewj.2042-7166.2011.01107.xPamela Francisca Bobadilla BurgosNo ratings yet
- Prevalence of Myofascial Trigger Points in Spinal Disorders: A Systematic Review and Meta-AnalysisDocument22 pagesPrevalence of Myofascial Trigger Points in Spinal Disorders: A Systematic Review and Meta-AnalysisGabriel Gaspar Bike FitNo ratings yet
- GP-led improvements cut cancer diagnosis timeDocument2 pagesGP-led improvements cut cancer diagnosis timeMj ManuelNo ratings yet
- Episodes For The Study of Change in Psychotherapy. Javiera Duarte SotoDocument28 pagesEpisodes For The Study of Change in Psychotherapy. Javiera Duarte SotoJoaquin OlivaresNo ratings yet
- Epiphany Storytelling As A Means of Reinforcing and Embedding Transformational Therapeutic ChangeDocument20 pagesEpiphany Storytelling As A Means of Reinforcing and Embedding Transformational Therapeutic ChangeVinícius GarciaNo ratings yet
- Being the Other Therapist 2001Document14 pagesBeing the Other Therapist 2001malwinatmdNo ratings yet
- The Transcendental Meditation Technique and Acute Experimental PainDocument8 pagesThe Transcendental Meditation Technique and Acute Experimental PainSamNo ratings yet
- Accepted Manuscript: 10.1016/j.jbmt.2018.02.019Document26 pagesAccepted Manuscript: 10.1016/j.jbmt.2018.02.019Kaïs de Vargas-Machuca GabandéNo ratings yet
- 176 289 1 SMDocument33 pages176 289 1 SMZzNo ratings yet
- Moritz 2012Document7 pagesMoritz 2012Makanudo.No ratings yet
- The Role of The Individual in The Coming Era of Process-Based Therapy (Articulo Examen Final)Document14 pagesThe Role of The Individual in The Coming Era of Process-Based Therapy (Articulo Examen Final)Cristian Steven Cabezas JoyaNo ratings yet
- CP302 Example 01 OKDocument5 pagesCP302 Example 01 OKAw Yeong Pei Yee100% (1)
- 21st Century Literary GenresDocument2 pages21st Century Literary GenresGO2. Aldovino Princess G.No ratings yet
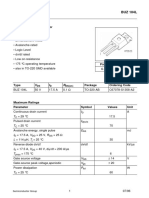
- Sipmos Power Transistor: BUZ 104LDocument10 pagesSipmos Power Transistor: BUZ 104LAlexsander MeloNo ratings yet
- GMS175CSDocument4 pagesGMS175CScorsini999No ratings yet
- Climate Change Survivor GameDocument22 pagesClimate Change Survivor Game许凉发No ratings yet
- Fisher - Techincal Monograph 42 - Understanding DecibelsDocument8 pagesFisher - Techincal Monograph 42 - Understanding Decibelsleslie.lp2003No ratings yet
- ASIA IVALUE Business ProfileDocument9 pagesASIA IVALUE Business ProfileDidiek PriambudiNo ratings yet
- Danbury BrochureDocument24 pagesDanbury BrochureQuique MartinNo ratings yet
- ECE SAR OldDocument168 pagesECE SAR OldNagaraja RaoNo ratings yet
- If Sentences Type 1 First Type Conditionals Grammar Drills - 119169Document2 pagesIf Sentences Type 1 First Type Conditionals Grammar Drills - 119169Ivanciu DanNo ratings yet
- Is Iso 2692-1992Document24 pagesIs Iso 2692-1992mwasicNo ratings yet
- Ventilator Modes - WEANINGDocument3 pagesVentilator Modes - WEANINGAlaa OmarNo ratings yet
- WISECO 2011 Complete CatalogDocument131 pagesWISECO 2011 Complete CatalogfishuenntNo ratings yet
- Application of Gis in Electrical Distribution Network SystemDocument16 pagesApplication of Gis in Electrical Distribution Network SystemMelese Sefiw100% (1)
- Download Zinc Surfaces A Guide To Alloys Finishes Fabrication And Maintenance In Architecture And Art 1St Edition L William Zahner all chapterDocument68 pagesDownload Zinc Surfaces A Guide To Alloys Finishes Fabrication And Maintenance In Architecture And Art 1St Edition L William Zahner all chapterdevin.brown498100% (7)
- Summative Test For Quadratic Equations2Document2 pagesSummative Test For Quadratic Equations2AsmiraMangontra0% (1)
- Q3 Curriculum Map - Mathematics 10Document3 pagesQ3 Curriculum Map - Mathematics 10Manilyn BaltazarNo ratings yet
- Coffee TestDocument6 pagesCoffee TestAmit Satyen RaviNo ratings yet
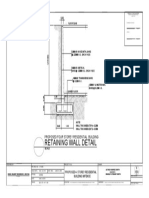
- Retaining Wall DetailsDocument1 pageRetaining Wall DetailsWilbert ReuyanNo ratings yet
- Little ThingsDocument3 pagesLittle ThingszwartwerkerijNo ratings yet
- Bahasa Inggris Kelas XIIDocument2 pagesBahasa Inggris Kelas XIIMuhammad ImadudinNo ratings yet
- Lesson 2Document10 pagesLesson 2angeliquefaithemnaceNo ratings yet
- Cubic Spline Tutorial v3Document6 pagesCubic Spline Tutorial v3Praveen SrivastavaNo ratings yet
- Fast and Reliable: Handheld TympanometerDocument4 pagesFast and Reliable: Handheld TympanometersermedNo ratings yet
- 6 An Indian American Woman in Space 2Document11 pages6 An Indian American Woman in Space 2Manju YadavNo ratings yet