You might also like
- 2022 Clinthera S1T3 Ami PDFDocument6 pages2022 Clinthera S1T3 Ami PDFmedicoNo ratings yet
- Patofisiologi ACSDocument48 pagesPatofisiologi ACSImelva GirsangNo ratings yet
- New Approaches to Aortic Diseases from Valve to Abdominal BifurcationFrom EverandNew Approaches to Aortic Diseases from Valve to Abdominal BifurcationNo ratings yet
- Acute Coronary SyndromeDocument27 pagesAcute Coronary SyndromeSahr Anne Pilar B. ParreñoNo ratings yet
- Acute Coronary Syndrome O: UtlineDocument5 pagesAcute Coronary Syndrome O: UtlinevmdcabanillaNo ratings yet
- Myocardia IschemiaDocument114 pagesMyocardia Ischemiasara rababahNo ratings yet
- Curriculum Vitae: Personal InformationDocument71 pagesCurriculum Vitae: Personal Informationtri kurniawanNo ratings yet
- Acute Coronary Syndrome: Imelva Yulviani GirsangDocument34 pagesAcute Coronary Syndrome: Imelva Yulviani GirsangAmeel BubbleeNo ratings yet
- Acute Coronary SyndromeDocument84 pagesAcute Coronary SyndromeRinkita MallickNo ratings yet
- Pathology 1016-Test 2 - Path 4Document3 pagesPathology 1016-Test 2 - Path 4Nicholas ObasiNo ratings yet
- 5.4 IHD HHD CHF Cor PulmonaleDocument15 pages5.4 IHD HHD CHF Cor PulmonaleMemay velascoNo ratings yet
- Acute Coronary SyndromeDocument41 pagesAcute Coronary SyndromeShrests SinhaNo ratings yet
- Cardiac ConditionsDocument15 pagesCardiac ConditionsMariane GumbanNo ratings yet
- NASKAHDocument19 pagesNASKAHHikmahhijab ColectionNo ratings yet
- Cardiac Biomarker 2014Document52 pagesCardiac Biomarker 2014karin amalia sabrina100% (1)
- Unstable Angina (UAP) and non-STEMIDocument66 pagesUnstable Angina (UAP) and non-STEMIIddrisu Abdul-AzizNo ratings yet
- 3) Management of IHD (Notes)Document25 pages3) Management of IHD (Notes)Priyanka GosaiNo ratings yet
- Myocardial Ischemia and Infarction, Part I ST Segment Elevation and Q Wave Syndromes, Goldberger's Clinical Electrocardiography PDFDocument19 pagesMyocardial Ischemia and Infarction, Part I ST Segment Elevation and Q Wave Syndromes, Goldberger's Clinical Electrocardiography PDFDavidNo ratings yet
- Acute Coronary Syndrome Sindroma Koroner AkutDocument50 pagesAcute Coronary Syndrome Sindroma Koroner AkutWinda Ayu PurnamasariNo ratings yet
- P 3b SKA StemiDocument72 pagesP 3b SKA StemiSasha ManoNo ratings yet
- Tinywow - L.4 Ischemic Cardiomyopathy - 28139370Document19 pagesTinywow - L.4 Ischemic Cardiomyopathy - 28139370filymascoloNo ratings yet
- Myocardial Ischemia and Infarction, Part II Non-ST Segment Elevation and Non-Q Wave Syndromes PDFDocument12 pagesMyocardial Ischemia and Infarction, Part II Non-ST Segment Elevation and Non-Q Wave Syndromes PDFDavidNo ratings yet
- Ekg PJKDocument110 pagesEkg PJKDexel Putra SimbolonNo ratings yet
- Notes Before ExamDocument24 pagesNotes Before Exams2175183No ratings yet
- 5 Coronary Artery DiseasesDocument60 pages5 Coronary Artery Diseasesjyothi lekshmi sNo ratings yet
- Konsep Tatalaksana Pada ImaDocument57 pagesKonsep Tatalaksana Pada Imariska silviaNo ratings yet
- Ardhendu Sinha Ray - Essentials of Internal Medicine-Jp Medical LTD (2017) - 92-105Document14 pagesArdhendu Sinha Ray - Essentials of Internal Medicine-Jp Medical LTD (2017) - 92-105Noveno CNo ratings yet
- Ischaemic Heart Disease (CR)Document11 pagesIschaemic Heart Disease (CR)Banana CakeNo ratings yet
- Acute Coronary Sindromes 21046 61975Document28 pagesAcute Coronary Sindromes 21046 61975Simina ÎntunericNo ratings yet
- L1 - Acute Coronary Syndrome - Yassen AyadDocument22 pagesL1 - Acute Coronary Syndrome - Yassen Ayadmtr325gfNo ratings yet
- Coronary Artery Disease (Cad)Document4 pagesCoronary Artery Disease (Cad)Freddy PanjaitanNo ratings yet
- Acute Coronary Syndrome - 2023Document38 pagesAcute Coronary Syndrome - 2023Noval LiadyNo ratings yet
- Acute Coronary SyndromeDocument12 pagesAcute Coronary SyndromeAnamaria SNo ratings yet
- Acute Coronary SyndromesDocument8 pagesAcute Coronary Syndromesadek07No ratings yet
- Myocardial Infarction (MI)Document29 pagesMyocardial Infarction (MI)ناصر دويكاتNo ratings yet
- Cardiac EmergencyDocument34 pagesCardiac EmergencyRima HannaniNo ratings yet
- ACS LectureDocument76 pagesACS Lecture21701101047 Laksmita AnggaraniNo ratings yet
- Ischemic Heart DiseaseDocument5 pagesIschemic Heart DiseaseBert DivinagraciaNo ratings yet
- Principle Management of Acute Coronary Syndrome: Nahar Taufiq Bagian Kardiologi Dan Kedokteran Vaskuler FK UGM YogyakartaDocument57 pagesPrinciple Management of Acute Coronary Syndrome: Nahar Taufiq Bagian Kardiologi Dan Kedokteran Vaskuler FK UGM YogyakartaIntan Farida YasminNo ratings yet
- Acute Coronary Syndrome (Acs) : DR M. Arman Nasution SPPDDocument162 pagesAcute Coronary Syndrome (Acs) : DR M. Arman Nasution SPPDfifahNo ratings yet
- ACS LectureDocument74 pagesACS Lecturekarin amalia sabrinaNo ratings yet
- Pathophysiology of Pathophysiology of Ischemic Heart Ischemic Heart Disease DiseaseDocument6 pagesPathophysiology of Pathophysiology of Ischemic Heart Ischemic Heart Disease DiseaseYudo PrabowoNo ratings yet
- POSTER - CASE REPORT Ver.2 Ventricular Tachycardia Storm and Unstable Ventricular Tachycardia in A 48-Years-Old Man Following A Non-ST Elevation Myocardial InfarctionDocument1 pagePOSTER - CASE REPORT Ver.2 Ventricular Tachycardia Storm and Unstable Ventricular Tachycardia in A 48-Years-Old Man Following A Non-ST Elevation Myocardial InfarctionRJMNo ratings yet
- Ischemic Heart DiseaseDocument8 pagesIschemic Heart DiseaseNina Natalia Bautista100% (1)
- MI SlidesDocument65 pagesMI SlidesJobelyn TunayNo ratings yet
- A. Narrative: Iv. PathophysiologyDocument3 pagesA. Narrative: Iv. Pathophysiologyr_cyrusNo ratings yet
- Cardio Dra. Deduyo: Ischemic Heart DiseaseDocument4 pagesCardio Dra. Deduyo: Ischemic Heart DiseaseIm SharaNo ratings yet
- PATHO-II Unit V Cardiovascular DisordersDocument52 pagesPATHO-II Unit V Cardiovascular DisordersMuhammad ShayanNo ratings yet
- OMedEd - Cardiology - CAD PDFDocument2 pagesOMedEd - Cardiology - CAD PDFJohn DoeNo ratings yet
- Acute MIDocument4 pagesAcute MICasuga, Jessica Carmela F.No ratings yet
- Overview of Acute Coronary Syndromes (ACS) : MSD Manual Professional VersionDocument11 pagesOverview of Acute Coronary Syndromes (ACS) : MSD Manual Professional VersionSuhadak DrsNo ratings yet
- Askep Pada Acute Coronary Syndrome AcsDocument62 pagesAskep Pada Acute Coronary Syndrome Acsdefi rhNo ratings yet
- Acute Coronary Syndrome Sindroma Koroner Akut: Toni Mustahsani Aprami, DR., SPPD, SPJPDocument57 pagesAcute Coronary Syndrome Sindroma Koroner Akut: Toni Mustahsani Aprami, DR., SPPD, SPJPrian susantoNo ratings yet
- Myocardial - Infarction Ferri PDFDocument9 pagesMyocardial - Infarction Ferri PDFEgidia SetyaNo ratings yet
- Acute Coronary SyndromesDocument40 pagesAcute Coronary Syndromesandi siregarNo ratings yet
- Acute Coronary Syndrome: by Ho NisaDocument58 pagesAcute Coronary Syndrome: by Ho NisaShre RanjithamNo ratings yet
- Acute Coronary SyndromeDocument48 pagesAcute Coronary SyndromeAchmad ulil Albab100% (1)
- Cvspa04 Ihd and MiDocument8 pagesCvspa04 Ihd and MiRobert So JrNo ratings yet
- Raminder Nirula - High-Yield Internal Medicine (High-Yield Series) - Lippincott Williams and Wilkins (2006)Document228 pagesRaminder Nirula - High-Yield Internal Medicine (High-Yield Series) - Lippincott Williams and Wilkins (2006)Isah Mohammed100% (1)
- Hemodynamic Monitoring in Cardiogenic Shock: ReviewDocument6 pagesHemodynamic Monitoring in Cardiogenic Shock: ReviewLeyden Chavez VergaraNo ratings yet
- StemphylumDocument5 pagesStemphylumapi-276652085No ratings yet
- Physiology of The Circulatory SystemDocument12 pagesPhysiology of The Circulatory SystemRugene Naragas BeratoNo ratings yet
- 50 Star Ccs Cases - USMLE ForumsDocument43 pages50 Star Ccs Cases - USMLE ForumsAbia Izzeldin Kamil100% (1)
- Clinical Abbreviations List - SESLHDPR 282Document46 pagesClinical Abbreviations List - SESLHDPR 282VitusMpotwaNo ratings yet
- Bootcamp 1 CTA Techniques - MitsumoriDocument72 pagesBootcamp 1 CTA Techniques - MitsumorirmdeloneyNo ratings yet
- Clinical Findings and Treatment in Cattle With Cae PDFDocument10 pagesClinical Findings and Treatment in Cattle With Cae PDFvetthamilNo ratings yet
- Workshop About The Heart and Cardiac CycleDocument4 pagesWorkshop About The Heart and Cardiac CycleLina Mafla100% (1)
- Livia Sagita Ruslim Cardio StemiDocument34 pagesLivia Sagita Ruslim Cardio StemiAnthony ChandraNo ratings yet
- Chapter 1: Introduction The Phylum Chordata: Big Four Protochordates HeadDocument14 pagesChapter 1: Introduction The Phylum Chordata: Big Four Protochordates HeadMacy MarianNo ratings yet
- Car&Ane&Pra&ASP&Sar&Gva&1 STDocument334 pagesCar&Ane&Pra&ASP&Sar&Gva&1 STAna Belén Artero CastañoNo ratings yet
- Circulationaha 108 191098Document9 pagesCirculationaha 108 191098rajesh kumarNo ratings yet
- Lab Manual Bio II 201701Document79 pagesLab Manual Bio II 201701Charlie LaiNo ratings yet
- Defining Characteristics Nursing Diagnosis Background Knowledge Desired Outcome Nursing Intervention Rationale EvaluationDocument2 pagesDefining Characteristics Nursing Diagnosis Background Knowledge Desired Outcome Nursing Intervention Rationale EvaluationnarsDNo ratings yet
- Dragon Maken War FULLDocument2,021 pagesDragon Maken War FULLaaNo ratings yet
- B.SC - Biochemistry Syllabus Srmasc May 2016 UpdatedDocument32 pagesB.SC - Biochemistry Syllabus Srmasc May 2016 UpdatedParthi ParthibanNo ratings yet
- Anatomy Supertable PDFDocument14 pagesAnatomy Supertable PDFAlex Ondevilla100% (1)
- Medical Power PointDocument124 pagesMedical Power PointPhysiology by Dr Raghuveer75% (4)
- Labelling (Answers)Document12 pagesLabelling (Answers)红熊红熊No ratings yet
- ch-4Document28 pagesch-4Nazmul Hasan SadiNo ratings yet
- CSA-AKI PatophysiologyDocument15 pagesCSA-AKI PatophysiologyOğuz KayıkçıNo ratings yet
- A Pediatric Echocardiographic Z Score Nomogram For A Developing Country: Indian Pediatric Echocardiography Study - The Z ScoreDocument8 pagesA Pediatric Echocardiographic Z Score Nomogram For A Developing Country: Indian Pediatric Echocardiography Study - The Z ScoreTia mssNo ratings yet
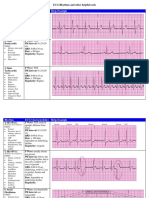
- Rhythm ECG Characteristics Strip Example: ECG Rhythms and Other Helpful ToolsDocument6 pagesRhythm ECG Characteristics Strip Example: ECG Rhythms and Other Helpful ToolsJohnildy MatiasNo ratings yet
- FP Form ItrDocument2 pagesFP Form ItrAlibasher Macalnas100% (1)
- CALIXRO, LJ NARRATIVE Ventricular Septal DefectDocument2 pagesCALIXRO, LJ NARRATIVE Ventricular Septal DefectKim SunooNo ratings yet
- Module in Science DoneeeeeDocument35 pagesModule in Science DoneeeeeManelyn TagaNo ratings yet
- Holter Medilog AR-4Document12 pagesHolter Medilog AR-4alistipis2165No ratings yet
- Dental Management of The Patient With Cardiac Arrhythmias: An UpdateDocument5 pagesDental Management of The Patient With Cardiac Arrhythmias: An UpdateDiego Zúñiga de LeónNo ratings yet
- Year 8. End of Semester Exam Marking SchemeDocument27 pagesYear 8. End of Semester Exam Marking SchemeAlejandro EspiNo ratings yet
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDFrom EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDRating: 5 out of 5 stars5/5 (5)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (39)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 4 out of 5 stars4/5 (5)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 4.5 out of 5 stars4.5/5 (84)
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)From EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Rating: 3 out of 5 stars3/5 (1)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (404)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeRating: 2 out of 5 stars2/5 (1)
- The Twentysomething Treatment: A Revolutionary Remedy for an Uncertain AgeFrom EverandThe Twentysomething Treatment: A Revolutionary Remedy for an Uncertain AgeRating: 4.5 out of 5 stars4.5/5 (3)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (44)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (267)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (170)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- I Shouldn't Feel This Way: Name What’s Hard, Tame Your Guilt, and Transform Self-Sabotage into Brave ActionFrom EverandI Shouldn't Feel This Way: Name What’s Hard, Tame Your Guilt, and Transform Self-Sabotage into Brave ActionNo ratings yet
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (46)
- Critical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsFrom EverandCritical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsRating: 4.5 out of 5 stars4.5/5 (39)
- The Fun Habit: How the Pursuit of Joy and Wonder Can Change Your LifeFrom EverandThe Fun Habit: How the Pursuit of Joy and Wonder Can Change Your LifeRating: 4.5 out of 5 stars4.5/5 (19)
- Manipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesFrom EverandManipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesRating: 4.5 out of 5 stars4.5/5 (1412)
- Summary: How to Be an Adult in Relationships: The Five Keys to Mindful Loving by David Richo: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: How to Be an Adult in Relationships: The Five Keys to Mindful Loving by David Richo: Key Takeaways, Summary & Analysis IncludedRating: 4 out of 5 stars4/5 (11)
- Dark Psychology: Learn To Influence Anyone Using Mind Control, Manipulation And Deception With Secret Techniques Of Dark Persuasion, Undetected Mind Control, Mind Games, Hypnotism And BrainwashingFrom EverandDark Psychology: Learn To Influence Anyone Using Mind Control, Manipulation And Deception With Secret Techniques Of Dark Persuasion, Undetected Mind Control, Mind Games, Hypnotism And BrainwashingRating: 4 out of 5 stars4/5 (1138)
- The Story of Philosophy: The Lives and Opinions of the Greater PhilosophersFrom EverandThe Story of Philosophy: The Lives and Opinions of the Greater PhilosophersNo ratings yet