You might also like
- Tally and O'Connor's Clinical Examination (8 Edition, Volume 1) Notes & Summaries by Yasin KadriDocument9 pagesTally and O'Connor's Clinical Examination (8 Edition, Volume 1) Notes & Summaries by Yasin KadriYasin KadriNo ratings yet
- Abdominal Pain, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandAbdominal Pain, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- History Taking PDFDocument2 pagesHistory Taking PDFAliNo ratings yet
- 2beginning The History Taking-1Document30 pages2beginning The History Taking-1Wizz Háķìm ĻêşòwNo ratings yet
- A Simple Guide to Rectal Disorders, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Rectal Disorders, Diagnosis, Treatment and Related ConditionsNo ratings yet
- Hopkins History Taking ArtDocument5 pagesHopkins History Taking ArtAnastasia TjanNo ratings yet
- A Practical Guide to Common Presenting Complaints in Primary CareFrom EverandA Practical Guide to Common Presenting Complaints in Primary CareNo ratings yet
- History TakingDocument9 pagesHistory Takingmahmoud selimNo ratings yet
- History Taking: DR Anwar H. SiddiquiDocument26 pagesHistory Taking: DR Anwar H. SiddiquiAssad mustafNo ratings yet
- Cardio History TakingDocument4 pagesCardio History Takingwaleed sonbol100% (2)
- Cardiovascular History Taking FrameworkDocument4 pagesCardiovascular History Taking Frameworkwaleed sonbolNo ratings yet
- Surgery Dr. Parinas 2Document7 pagesSurgery Dr. Parinas 2Cassandra Grace Muerong Dela CruzNo ratings yet
- History Taking Physical ExamininationDocument41 pagesHistory Taking Physical ExamininationAya AmerNo ratings yet
- Taking History & Methods of Physical Examination For: Koray TopgülDocument38 pagesTaking History & Methods of Physical Examination For: Koray Topgülayadalshawki7100% (1)
- PCDDocument15 pagesPCDana100% (1)
- Urological History Taking FrameworkDocument5 pagesUrological History Taking FrameworkahmadNo ratings yet
- HA Lec 16Document10 pagesHA Lec 16Althea Sachi CruzNo ratings yet
- Mustansiriyah Lecture Notes On Surgical History & Clinical ExaminationDocument57 pagesMustansiriyah Lecture Notes On Surgical History & Clinical Examinationنور الهدى ابراهيم خضير معيليNo ratings yet
- CLERKSHIP GUIDE FOR MEDICINE AND SURGERYDocument29 pagesCLERKSHIP GUIDE FOR MEDICINE AND SURGERYtemitopeNo ratings yet
- Cardiovascular History Taking - Geeky MedicsDocument6 pagesCardiovascular History Taking - Geeky MedicsJahangir AlamNo ratings yet
- OSCE Revision Guide for Clinical AssessmentsDocument66 pagesOSCE Revision Guide for Clinical AssessmentsApoorva SaxenaNo ratings yet
- HX TakingDocument37 pagesHX TakingAya SalahNo ratings yet
- Sheet Abeer PDFDocument96 pagesSheet Abeer PDFFate ChanNo ratings yet
- History and Physical Exam SkillsDocument7 pagesHistory and Physical Exam SkillsAnonymous Sfcml4GvZNo ratings yet
- Final Exam Study Guide Health AssessmentDocument16 pagesFinal Exam Study Guide Health AssessmentSraddha Patel100% (1)
- Urological History TakingDocument6 pagesUrological History TakingayuniNo ratings yet
- 02 C F Components of HistoryDocument34 pages02 C F Components of HistoryYared TJNo ratings yet
- Clinical Case Presentations CARE IIDocument44 pagesClinical Case Presentations CARE IIStarr Newman100% (1)
- T C AnkrahDocument198 pagesT C AnkrahDeep Sleep100% (8)
- Introduction History and ExaminationDocument43 pagesIntroduction History and ExaminationDanyal Hassan100% (1)
- DR - Mary JohnPROTOCOL EXAMINATION-2Document9 pagesDR - Mary JohnPROTOCOL EXAMINATION-2Ria MasihNo ratings yet
- Internal All PracticalDocument60 pagesInternal All PracticalearNo ratings yet
- OSCE Paeds Master Sheet Rachel AlbertDocument26 pagesOSCE Paeds Master Sheet Rachel AlbertVahni SamarooNo ratings yet
- 02 1-Principles of History Taking and Physical ExaminationDocument56 pages02 1-Principles of History Taking and Physical ExaminationMorani WijegunawardanaNo ratings yet
- History & Physical Diagnostic#Document106 pagesHistory & Physical Diagnostic#Olsa Alshapira100% (1)
- Basic History Taking: Tim Communication Skill FKUBDocument30 pagesBasic History Taking: Tim Communication Skill FKUBnarulita_94No ratings yet
- History Taking Techniques and Components for EMS ProvidersDocument9 pagesHistory Taking Techniques and Components for EMS ProvidersALI ALFARDANNo ratings yet
- History Taking Techniques for Accurate DiagnosisDocument88 pagesHistory Taking Techniques for Accurate DiagnosisBnB UsmleNo ratings yet
- History Taking & ExaminationDocument14 pagesHistory Taking & ExaminationMark AdrianNo ratings yet
- History TakingDocument19 pagesHistory TakingAlice Verran100% (1)
- History Taking2Document25 pagesHistory Taking2Capture UnseenNo ratings yet
- Examining the Cardiovascular SystemDocument152 pagesExamining the Cardiovascular SystemAloah122346100% (2)
- DR - Muse Medical History & Physical ExmnDocument27 pagesDR - Muse Medical History & Physical Exmnaxmedfare138No ratings yet
- OSCE NotesDocument4 pagesOSCE NotesHighschool AudiobooksNo ratings yet
- Pemeriksaan Abdomen: Dr. Suhaemi, SPPD, FinasimDocument179 pagesPemeriksaan Abdomen: Dr. Suhaemi, SPPD, FinasimiroelnafialyskaNo ratings yet
- General History Taking - CompressDocument37 pagesGeneral History Taking - CompressRawabi Saleh100% (1)
- History & Physical ExaminationDocument67 pagesHistory & Physical ExaminationDiggi VioNo ratings yet
- History Taking - The Critical First Step in DiagnosisDocument51 pagesHistory Taking - The Critical First Step in DiagnosisJAMES TONNY OKINYINo ratings yet
- History Taking Guide - 70% Diagnosis from Patient HistoryDocument51 pagesHistory Taking Guide - 70% Diagnosis from Patient HistoryJAMES TONNY OKINYINo ratings yet
- Holistic Geriatric Assessment ToolDocument15 pagesHolistic Geriatric Assessment ToolMarianne DugosNo ratings yet
- Assessing Abdominal Pain: Key Historical Questions and Physical Exam FindingsDocument24 pagesAssessing Abdominal Pain: Key Historical Questions and Physical Exam FindingsRodaina MohamedNo ratings yet
- Abdominal Examination UMYDocument181 pagesAbdominal Examination UMYMspitha LiaNo ratings yet
- Patient Examination: History: by Professor of Internal MedicineDocument47 pagesPatient Examination: History: by Professor of Internal MedicineMonqith YousifNo ratings yet
- Medicine 250 Interactive Integrative Case Based Session Study Guide For StudentsDocument1 pageMedicine 250 Interactive Integrative Case Based Session Study Guide For StudentsBA OngNo ratings yet
- Surgery History and PhysicalDocument23 pagesSurgery History and PhysicalBilal RowaihiNo ratings yet
- Card Medical HistoryDocument4 pagesCard Medical HistoryDanonino12No ratings yet
- Chronic Cholecystitis GuideDocument33 pagesChronic Cholecystitis Guidegplabon100% (2)
- Internal MedicineDocument18 pagesInternal MedicineNashaat H. AlshawabkehNo ratings yet
- Drainage Manual: State of Florida Department of TransportationDocument78 pagesDrainage Manual: State of Florida Department of TransportationghoyarbideNo ratings yet
- Wave Optics - I: Created by C. Mani, Principal, K V No.1, AFS, Jalahalli West, BangaloreDocument16 pagesWave Optics - I: Created by C. Mani, Principal, K V No.1, AFS, Jalahalli West, BangaloreNitesh Gupta100% (1)
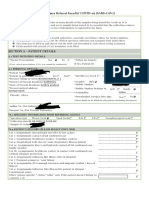
- Sample Id: Sample Id: 6284347 Icmr Specimen Referral Form Icmr Specimen Referral Form For For Covid-19 (Sars-Cov2) Covid-19 (Sars-Cov2)Document2 pagesSample Id: Sample Id: 6284347 Icmr Specimen Referral Form Icmr Specimen Referral Form For For Covid-19 (Sars-Cov2) Covid-19 (Sars-Cov2)Praveen KumarNo ratings yet
- The History of Coins and Banknotes in Mexico: September 2012Document35 pagesThe History of Coins and Banknotes in Mexico: September 2012Mladen VidovicNo ratings yet
- Root Cause Analysis: Identifying Factors Behind Patient Safety IncidentsDocument5 pagesRoot Cause Analysis: Identifying Factors Behind Patient Safety IncidentsPrabhas_Das7No ratings yet
- Parleremo Pzfra1Document218 pagesParleremo Pzfra1Lucia FerentNo ratings yet
- Grammar Pages 109-112 2 PDFDocument4 pagesGrammar Pages 109-112 2 PDFSteve SernaNo ratings yet
- Bioprocess Engineering QuestionsDocument13 pagesBioprocess Engineering QuestionsPalanisamy Selvamani100% (1)
- LQRDocument34 pagesLQRkemoNo ratings yet
- Ndeb Bned Reference Texts 2019 PDFDocument11 pagesNdeb Bned Reference Texts 2019 PDFnavroop bajwaNo ratings yet
- Fit Friend Business Game StrategiesDocument7 pagesFit Friend Business Game StrategiesSanchit AggarwalNo ratings yet
- ASTM D5895 - 2020 Tiempo SecadoDocument4 pagesASTM D5895 - 2020 Tiempo SecadoPablo OrtegaNo ratings yet
- Consumer PerceptionDocument61 pagesConsumer PerceptionPrakhar DwivediNo ratings yet
- DriveDebug User ManualDocument80 pagesDriveDebug User ManualFan CharlesNo ratings yet
- Letter of Invitation ESVC 3000 2024 1Document2 pagesLetter of Invitation ESVC 3000 2024 1pradeep kumarNo ratings yet
- Calendula EbookDocument12 pagesCalendula EbookCeciliaNo ratings yet
- Samsung (UH5003-SEA) BN68-06750E-01ENG-0812Document2 pagesSamsung (UH5003-SEA) BN68-06750E-01ENG-0812asohas77No ratings yet
- Get TRDocDocument209 pagesGet TRDoc10131No ratings yet
- Water Booster Pump Calculations - Plumbing Engineering - Eng-TipsDocument3 pagesWater Booster Pump Calculations - Plumbing Engineering - Eng-TipsNeal JohnsonNo ratings yet
- Manual de Partes 501-601Document27 pagesManual de Partes 501-601camilo bautista100% (2)
- SAP MM ReportsDocument59 pagesSAP MM Reportssaprajpal95% (21)
- Book Notes - The Life Changing Magic of Tidying Up PDFDocument6 pagesBook Notes - The Life Changing Magic of Tidying Up PDFAilyn Bagares AñanoNo ratings yet
- USA Gas TurbineDocument4 pagesUSA Gas TurbineJustin MercadoNo ratings yet
- LEEA-030.2c2 Certificate of Thorough Examination (Multiple Items) (Overseas) (Dev)Document1 pageLEEA-030.2c2 Certificate of Thorough Examination (Multiple Items) (Overseas) (Dev)GaniyuNo ratings yet
- EPON ONU with 4FE+WiFi EONU-04WDocument4 pagesEPON ONU with 4FE+WiFi EONU-04WAndres Alberto ParraNo ratings yet
- Eliminator ® Liquid Line Fi Lter Driers: DML and DCLDocument12 pagesEliminator ® Liquid Line Fi Lter Driers: DML and DCLbracaNSNo ratings yet
- Chengdu Bus GroupDocument2 pagesChengdu Bus GroupMohammad LabbanNo ratings yet
- PILE LOAD TEST PROCEDURE GUIDEDocument2 pagesPILE LOAD TEST PROCEDURE GUIDEJEFFY JACOBNo ratings yet
- Detailed Lesson Plan in TechnologyDocument11 pagesDetailed Lesson Plan in TechnologyReshiela OrtizNo ratings yet
- Q3 SolutionDocument5 pagesQ3 SolutionShaina0% (1)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (14)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 5 out of 5 stars5/5 (4)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 3.5 out of 5 stars3.5/5 (2)
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsFrom EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo ratings yet
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 3.5 out of 5 stars3.5/5 (33)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (44)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (328)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 5 out of 5 stars5/5 (5)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- Summary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisFrom EverandSummary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisRating: 5 out of 5 stars5/5 (8)