You might also like
- The Comprehensive Adult Health History Taking: For C-I StudentsDocument18 pagesThe Comprehensive Adult Health History Taking: For C-I StudentskderibNo ratings yet
- History ExaminationDocument37 pagesHistory ExaminationDina GamalNo ratings yet
- ASSESSMENTDocument52 pagesASSESSMENTPaul walkerNo ratings yet
- S1 - History Taking PresentationDocument37 pagesS1 - History Taking Presentationyouservezeropurpose113No ratings yet
- Health History Format Imad Lesson 1Document18 pagesHealth History Format Imad Lesson 1ellen_lomioNo ratings yet
- Diagnostic of Internal Diseases. Main Methods of Examination. Lecture N1Document40 pagesDiagnostic of Internal Diseases. Main Methods of Examination. Lecture N1Noor AliNo ratings yet
- Well Woman Physical: ObjectivesDocument50 pagesWell Woman Physical: ObjectivesbiffdoggieNo ratings yet
- Health AssessmentDocument18 pagesHealth AssessmentSavita Hanamsagar100% (1)
- (PEDIA) Clerks Revalida Review 2022Document130 pages(PEDIA) Clerks Revalida Review 2022Sheila SantosNo ratings yet
- 1 - Internal Medicine UKIDocument128 pages1 - Internal Medicine UKILewishoppusNo ratings yet
- Assignment in PathoDocument8 pagesAssignment in PathoLyka Milo AvilaNo ratings yet
- 2023 Introduction To Physical DiagnosisDocument37 pages2023 Introduction To Physical DiagnosisNejibMohe Abagisa100% (1)
- Week 7 - Lecture NotesDocument76 pagesWeek 7 - Lecture NotesAbdul Rahim RattaniNo ratings yet
- Case of ENDocument73 pagesCase of ENHarold Nathan TanNo ratings yet
- HistoryDocument27 pagesHistoryabuhajerah15No ratings yet
- Orthopedic History and Physical ExamDocument28 pagesOrthopedic History and Physical ExamAgriya Shresth100% (1)
- History Taking Physical ExamininationDocument41 pagesHistory Taking Physical ExamininationAya AmerNo ratings yet
- Physical AssessmentDocument8 pagesPhysical AssessmentGlaiza LiamMaddieNo ratings yet
- A 5 - Initial Assesment Untl 2017Document45 pagesA 5 - Initial Assesment Untl 2017Tíťhús D'Cårvålhõ100% (1)
- A Guide To Physical ExaminationDocument73 pagesA Guide To Physical ExaminationDessy AmaranthaNo ratings yet
- HISTORYDocument28 pagesHISTORYrxmskdkd33No ratings yet
- Seminar - History Taking & Physical ExaminationDocument13 pagesSeminar - History Taking & Physical ExaminationsarxxxxNo ratings yet
- Initial Assesment Untl 2017Document45 pagesInitial Assesment Untl 2017Maqatu P'xiguNo ratings yet
- Clinical Examination: Plan of Conduction & Scheme of RecordingDocument112 pagesClinical Examination: Plan of Conduction & Scheme of RecordingNilakshi Barik MandalNo ratings yet
- History TakingDocument28 pagesHistory TakingMutegeki AdolfNo ratings yet
- History Taking & ExaminationDocument14 pagesHistory Taking & ExaminationMark AdrianNo ratings yet
- 02 C F Components of HistoryDocument34 pages02 C F Components of HistoryYared TJNo ratings yet
- 6-Head and Neck ExaminationDocument34 pages6-Head and Neck Examinationaxmedfare36No ratings yet
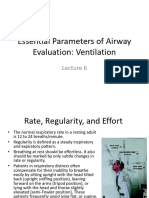
- Essential Parameters of Airway Evaluation Lecture 6Document27 pagesEssential Parameters of Airway Evaluation Lecture 69yqgmkvyzdNo ratings yet
- 02 1-Principles of History Taking and Physical ExaminationDocument56 pages02 1-Principles of History Taking and Physical ExaminationMorani WijegunawardanaNo ratings yet
- 15.1. History Taking + ECG 1-肖培林Document125 pages15.1. History Taking + ECG 1-肖培林mirabel IvanaliNo ratings yet
- Patient Examination: History: by Professor of Internal MedicineDocument47 pagesPatient Examination: History: by Professor of Internal MedicineMonqith YousifNo ratings yet
- Case History: U, Stor, SDocument41 pagesCase History: U, Stor, SmohanNo ratings yet
- Slide 1 - The History and Physical ExamDocument38 pagesSlide 1 - The History and Physical ExamCWT2010No ratings yet
- Head To Toe Assessment - InserviceDocument10 pagesHead To Toe Assessment - InservicelovelivetaylorNo ratings yet
- A Review of A Case of A Patient Presenting With Low Back Pain Leading To A Low Back Emergency Managed in The Intensive Care Unit.Document57 pagesA Review of A Case of A Patient Presenting With Low Back Pain Leading To A Low Back Emergency Managed in The Intensive Care Unit.chadchimaNo ratings yet
- Physical ExaminationDocument39 pagesPhysical ExaminationMutegeki AdolfNo ratings yet
- Pediatric CVS Exam: 2015/2016 Mohamad-Hani Temsah, M.DDocument24 pagesPediatric CVS Exam: 2015/2016 Mohamad-Hani Temsah, M.Dعلي. احمدNo ratings yet
- Clinical Examination: Plan of Conduction & Scheme of RecordingDocument112 pagesClinical Examination: Plan of Conduction & Scheme of RecordingNilakshi Barik MandalNo ratings yet
- Physical DiagnosisDocument63 pagesPhysical Diagnosishailemariamgebrehiwot02No ratings yet
- Clinical Examination - Eric Sarpong-NtiamoahDocument52 pagesClinical Examination - Eric Sarpong-NtiamoahFathimathNo ratings yet
- Physical Assessment ComprehensiveDocument118 pagesPhysical Assessment ComprehensiverootieNo ratings yet
- History Taking and ExaminationDocument48 pagesHistory Taking and ExaminationNaomi Tolulope OlasehindeNo ratings yet
- Sheet AnamnesisDocument4 pagesSheet Anamnesis4gen_7No ratings yet
- HX TakingDocument37 pagesHX TakingAya SalahNo ratings yet
- ADCON April 12 406Document23 pagesADCON April 12 406Andrassy Twinkle AlineaNo ratings yet
- Lecture 11 History TakingDocument6 pagesLecture 11 History Takingpxb8dhqgs9No ratings yet
- 'Span BibleDocument96 pages'Span BiblePatrice BlakeNo ratings yet
- Physical Examination 2011Document171 pagesPhysical Examination 2011Norakmal Andika YusriNo ratings yet
- 1a-History Taking in SurgeryDocument19 pages1a-History Taking in SurgeryMohammad Farouq Omar100% (1)
- Outline For Pediatric HistoryDocument15 pagesOutline For Pediatric HistoryZīshān Fārūq100% (2)
- Medical HistoryDocument13 pagesMedical HistoryChiranjeevi Kumar EndukuruNo ratings yet
- History Taking: DR Anwar H. SiddiquiDocument26 pagesHistory Taking: DR Anwar H. SiddiquiAssad mustafNo ratings yet
- Physical Exam For DiagnosisDocument61 pagesPhysical Exam For DiagnosisSurat Tanprawate100% (2)
- Case Presentation On Urinary Tract InfectionDocument86 pagesCase Presentation On Urinary Tract InfectionPraty SawadenNo ratings yet
- Introduction To Internal Medicine - PPTMDocument30 pagesIntroduction To Internal Medicine - PPTMAddyNo ratings yet
- The Ultimate Guide to Physician Associate OSCEs: Written by a Physician Associate for Physician AssociatesFrom EverandThe Ultimate Guide to Physician Associate OSCEs: Written by a Physician Associate for Physician AssociatesNo ratings yet
- Shenimt e Mia Personale Per DDXDocument281 pagesShenimt e Mia Personale Per DDXJeronim H'gharNo ratings yet
- Internal Medicine IDocument3 pagesInternal Medicine Iaxmedfare138No ratings yet
- Case Study On Congestive Heart FailureDocument5 pagesCase Study On Congestive Heart Failureaxmedfare138No ratings yet
- Case Study On Congestive Heart FailureDocument5 pagesCase Study On Congestive Heart Failureaxmedfare138No ratings yet
- Case Presentation: Hypertension: Anish Dhakal (Aryan)Document18 pagesCase Presentation: Hypertension: Anish Dhakal (Aryan)axmedfare138No ratings yet
- 4.iJGP - Case ReportDocument4 pages4.iJGP - Case Reportpalak GandhiNo ratings yet
- Emotional Body Pain Chart: How It WorksDocument3 pagesEmotional Body Pain Chart: How It Worksdaniel50% (2)
- Final Draft Research EssayDocument4 pagesFinal Draft Research EssayizellahnavarroNo ratings yet
- (Template) BEED CHAPTER 3 MODULE 3 - Sci 1Document6 pages(Template) BEED CHAPTER 3 MODULE 3 - Sci 1Regilyn GalasNo ratings yet
- Nebosh: Management of Health and Safety Unit Ig1Document5 pagesNebosh: Management of Health and Safety Unit Ig1TFIBER PROGRESSNo ratings yet
- Arrangement of Artificial Teeth: Dr. Enas Abdul-SattarDocument50 pagesArrangement of Artificial Teeth: Dr. Enas Abdul-SattarShashank AadarshNo ratings yet
- Skil Lab EBMDocument6 pagesSkil Lab EBMYahya Darmais FaridNo ratings yet
- Week Four AssignmentDocument4 pagesWeek Four AssignmentRachel Elaine WilliamsNo ratings yet
- HIV Related Policies and Guidelines Issuances: Training On HIV Counseling and Testing and Facility-Based HIV ScreeningDocument77 pagesHIV Related Policies and Guidelines Issuances: Training On HIV Counseling and Testing and Facility-Based HIV ScreeningJovania B.No ratings yet
- Acute Kidney InjuryDocument4 pagesAcute Kidney Injuryjumi jumdailNo ratings yet
- KI Health 75th FinalDocument127 pagesKI Health 75th FinalChandrimaChatterjeeNo ratings yet
- Sop of Disinfection, CoatingDocument27 pagesSop of Disinfection, CoatingAhmed Quadri0% (1)
- PrelimDocument3 pagesPrelimJM RebancosNo ratings yet
- Diagnostic Test Battery For Different Age GroupsDocument14 pagesDiagnostic Test Battery For Different Age GroupsDhana KrishnaNo ratings yet
- CS Form No - 6, Revised 2020 (Application For Leave) (Fillable) - 1Document3 pagesCS Form No - 6, Revised 2020 (Application For Leave) (Fillable) - 1ben carlo ramos srNo ratings yet
- Neonatal and Pediatric Mechanical Ventilation - 2020Document88 pagesNeonatal and Pediatric Mechanical Ventilation - 2020Ahmed YasserNo ratings yet
- Articles of PartnershipDocument3 pagesArticles of Partnershipjonel sembranaNo ratings yet
- Chapter1 To 3Document26 pagesChapter1 To 3Gerard Adrian Bautista AnonuevoNo ratings yet
- Parent Child RelationshipDocument8 pagesParent Child RelationshipHUSSAINA BANONo ratings yet
- Method of Statement For GroutingDocument7 pagesMethod of Statement For GroutingCezar DasiNo ratings yet
- Minimal Invasive Dentistry-A Comprehensive ReviewDocument9 pagesMinimal Invasive Dentistry-A Comprehensive ReviewKarissa NavitaNo ratings yet
- Chinese Contractor Wins Kuwait Remediation WorkDocument4 pagesChinese Contractor Wins Kuwait Remediation WorkSanabel EliasNo ratings yet
- Staff Nurses, Lab-Technicians& Pharmacists: WWW - Vizianagaram.nic - inDocument6 pagesStaff Nurses, Lab-Technicians& Pharmacists: WWW - Vizianagaram.nic - inSATYAM NAIDUNo ratings yet
- Ulkus DiabetikumDocument8 pagesUlkus DiabetikumDwi Feri HariyantoNo ratings yet
- Name: Date: - Year/Section:: Task 1: PAR-Q and YOU Questionnaire (Prior To The Activity Test)Document3 pagesName: Date: - Year/Section:: Task 1: PAR-Q and YOU Questionnaire (Prior To The Activity Test)Angela Louise Smiths0% (1)
- Sweet Dreams KitDocument1 pageSweet Dreams KitPoplacenel Serban DanNo ratings yet
- Free Consent - UNDUE INFLUENCEDocument3 pagesFree Consent - UNDUE INFLUENCESEKANISH KALPANA ANo ratings yet
- Community Health Situtional AnalysisDocument79 pagesCommunity Health Situtional AnalysisYongNo ratings yet
- Informative Speech TextDocument2 pagesInformative Speech TextadzwinjNo ratings yet
- Drako Fluid SF 10 enDocument11 pagesDrako Fluid SF 10 enthanggimme.phanNo ratings yet