You might also like
- Rapid On-site Evaluation (ROSE): A Practical GuideFrom EverandRapid On-site Evaluation (ROSE): A Practical GuideGuoping CaiNo ratings yet
- The Papanicolaou Society of Cytopathology System for Reporting Respiratory Cytology: Definitions, Criteria, Explanatory Notes, and Recommendations for Ancillary TestingFrom EverandThe Papanicolaou Society of Cytopathology System for Reporting Respiratory Cytology: Definitions, Criteria, Explanatory Notes, and Recommendations for Ancillary TestingNo ratings yet
- Breast Cancer in Young WomenFrom EverandBreast Cancer in Young WomenOreste GentiliniNo ratings yet
- Outcome Prediction in CancerFrom EverandOutcome Prediction in CancerAzzam F.G. TaktakNo ratings yet
- Imaging in Pediatric OncologyFrom EverandImaging in Pediatric OncologyStephan D. VossNo ratings yet
- Diagnosis and Management of Cholangiocarcinoma: A Multidisciplinary ApproachFrom EverandDiagnosis and Management of Cholangiocarcinoma: A Multidisciplinary ApproachJames H. TabibianNo ratings yet
- Precision Molecular Pathology of Prostate CancerFrom EverandPrecision Molecular Pathology of Prostate CancerBrian D. RobinsonNo ratings yet
- Quality and Safety in ImagingFrom EverandQuality and Safety in ImagingLluís Donoso-BachNo ratings yet
- Diagnosis and Management of Hereditary Cancer: Tabular-Based Clinical and Genetic AspectsFrom EverandDiagnosis and Management of Hereditary Cancer: Tabular-Based Clinical and Genetic AspectsNo ratings yet
- Diagnostic Problems in Tumors of Head and Neck: Selected TopicsFrom EverandDiagnostic Problems in Tumors of Head and Neck: Selected TopicsRating: 5 out of 5 stars5/5 (1)
- MDCT and MR Imaging of Acute Abdomen: New Technologies and Emerging IssuesFrom EverandMDCT and MR Imaging of Acute Abdomen: New Technologies and Emerging IssuesMichael PatlasNo ratings yet
- Histopathology Reporting: Guidelines for Surgical CancerFrom EverandHistopathology Reporting: Guidelines for Surgical CancerDavid P. BoyleNo ratings yet
- Breast Disease: Diagnosis and Pathology, Volume 1From EverandBreast Disease: Diagnosis and Pathology, Volume 1Adnan AydinerNo ratings yet
- Frozen Section Pathology: Diagnostic ChallengesFrom EverandFrozen Section Pathology: Diagnostic ChallengesAlain C. BorczukNo ratings yet
- Management of Urologic Cancer: Focal Therapy and Tissue PreservationFrom EverandManagement of Urologic Cancer: Focal Therapy and Tissue PreservationNo ratings yet
- Atypical Breast Proliferative Lesions and Benign Breast DiseaseFrom EverandAtypical Breast Proliferative Lesions and Benign Breast DiseaseFarin AmersiNo ratings yet
- Interstitial Prostate Brachytherapy: LDR-PDR-HDRFrom EverandInterstitial Prostate Brachytherapy: LDR-PDR-HDRGyörgy KovácsNo ratings yet
- The SAGES Manual of Colorectal SurgeryFrom EverandThe SAGES Manual of Colorectal SurgeryPatricia SyllaNo ratings yet
- Nasopharyngeal Carcinoma: From Etiology to Clinical PracticeFrom EverandNasopharyngeal Carcinoma: From Etiology to Clinical PracticeAnne W.M. LeeNo ratings yet
- Precision Medicine Oncology: A PrimerFrom EverandPrecision Medicine Oncology: A PrimerLorna Rodriguez-RodriguezNo ratings yet
- Atlas of Multiparametric Prostate MRI: With PI-RADS Approach and Anatomic-MRI-Pathological CorrelationFrom EverandAtlas of Multiparametric Prostate MRI: With PI-RADS Approach and Anatomic-MRI-Pathological CorrelationNo ratings yet
- Translational Research in Breast CancerFrom EverandTranslational Research in Breast CancerDong-Young NohNo ratings yet
- Pathology of Female Cancers: Precursor and Early-Stage Breast, Ovarian and Uterine CarcinomasFrom EverandPathology of Female Cancers: Precursor and Early-Stage Breast, Ovarian and Uterine CarcinomasTakuya MoriyaNo ratings yet
- Diagnostic Problems in Tumors of Central Nervous System: Selected TopicsFrom EverandDiagnostic Problems in Tumors of Central Nervous System: Selected TopicsNo ratings yet
- Lower Genital Tract Precancer: Colposcopy, Pathology and TreatmentFrom EverandLower Genital Tract Precancer: Colposcopy, Pathology and TreatmentNo ratings yet
- Genomic Medicine: A Practical GuideFrom EverandGenomic Medicine: A Practical GuideLaura J. TafeNo ratings yet
- Upper Tract Urothelial CarcinomaFrom EverandUpper Tract Urothelial CarcinomaShahrokh F. ShariatNo ratings yet
- Fast Facts: Clinical Trials in Oncology: The fundamentals of design, conduct and interpretationFrom EverandFast Facts: Clinical Trials in Oncology: The fundamentals of design, conduct and interpretationNo ratings yet
- Multiparametric Ultrasound Diagnosis of Breast DiseasesFrom EverandMultiparametric Ultrasound Diagnosis of Breast DiseasesGennady T. SukhikhNo ratings yet
- Hepatocellular Carcinoma: Translational Precision Medicine ApproachesFrom EverandHepatocellular Carcinoma: Translational Precision Medicine ApproachesYujin HoshidaNo ratings yet
- Molecular Diagnostics and Treatment of Pancreatic Cancer: Systems and Network Biology ApproachesFrom EverandMolecular Diagnostics and Treatment of Pancreatic Cancer: Systems and Network Biology ApproachesNo ratings yet
- Targeted Cancer Imaging: Design and Synthesis of Nanoplatforms based on Tumor BiologyFrom EverandTargeted Cancer Imaging: Design and Synthesis of Nanoplatforms based on Tumor BiologyNo ratings yet
- Atlas of Early Neoplasias of the Gastrointestinal Tract: Endoscopic Diagnosis and Therapeutic DecisionsFrom EverandAtlas of Early Neoplasias of the Gastrointestinal Tract: Endoscopic Diagnosis and Therapeutic DecisionsFrieder BerrNo ratings yet
- Glioma Imaging: Physiologic, Metabolic, and Molecular ApproachesFrom EverandGlioma Imaging: Physiologic, Metabolic, and Molecular ApproachesWhitney B. PopeNo ratings yet
- Diagnosis of Endometrial Biopsies and Curettings: A Practical ApproachFrom EverandDiagnosis of Endometrial Biopsies and Curettings: A Practical ApproachNo ratings yet
- The American Cancer Society's Principles of Oncology: Prevention to SurvivorshipFrom EverandThe American Cancer Society's Principles of Oncology: Prevention to SurvivorshipThe American Cancer SocietyNo ratings yet
- Human Papillomavirus: Proving and Using a Viral Cause for CancerFrom EverandHuman Papillomavirus: Proving and Using a Viral Cause for CancerNo ratings yet
- G150 Non Op Reporting Breast Cancer ScreeningDocument84 pagesG150 Non Op Reporting Breast Cancer ScreeningTania OrtegaNo ratings yet
- Pathol 2021 05 354Document6 pagesPathol 2021 05 354Tania OrtegaNo ratings yet
- TablaDescuentosGenerales 3T2022 ADocument1 pageTablaDescuentosGenerales 3T2022 ATania OrtegaNo ratings yet
- 2023 Imaging Findings in Cirrhotic LiverDocument14 pages2023 Imaging Findings in Cirrhotic LiverTania OrtegaNo ratings yet
- Rubrica de Higado 28-Iv-21Document6 pagesRubrica de Higado 28-Iv-21Tania OrtegaNo ratings yet
- DCM 194 oDocument2 pagesDCM 194 oTania OrtegaNo ratings yet
- Pediatria TrigonocefaliaDocument2 pagesPediatria TrigonocefaliaTania OrtegaNo ratings yet
- RM RodillaDocument11 pagesRM RodillaTania OrtegaNo ratings yet
- Sackett2002 en EsDocument3 pagesSackett2002 en EsTania OrtegaNo ratings yet
- COVID19 Delphi 2023Document21 pagesCOVID19 Delphi 2023Tania OrtegaNo ratings yet
- TOC Prof Chintamanis Comprehensive Book On SurgeryDocument4 pagesTOC Prof Chintamanis Comprehensive Book On SurgeryKoustav ChakrabortyNo ratings yet
- Clinical Practice Guidelines For The Diagnosis and Treatment of Patients With Soft Tissue Sarcoma by The Spanish Group For Research in Sarcomas (GEIS)Document14 pagesClinical Practice Guidelines For The Diagnosis and Treatment of Patients With Soft Tissue Sarcoma by The Spanish Group For Research in Sarcomas (GEIS)carolinapolotorresNo ratings yet
- Here Is My Project ReportDocument14 pagesHere Is My Project ReportAsha PandeyNo ratings yet
- IJHEGY-Volume 1-Issue 3 - Page 84-95Document12 pagesIJHEGY-Volume 1-Issue 3 - Page 84-95Abo-ahmed ElmasryNo ratings yet
- Hossain Tonmoy B.sc. ThesisDocument109 pagesHossain Tonmoy B.sc. ThesisAsma ChikhaouiNo ratings yet
- Thesis Topics in Pathology MDDocument6 pagesThesis Topics in Pathology MDbsdy4ahp100% (2)
- (Download pdf) Human Diseases Marianne Neighbors full chapter pdf docxDocument69 pages(Download pdf) Human Diseases Marianne Neighbors full chapter pdf docxbuggsquoffi100% (5)
- Cancer and Its Treatment: An OverviewDocument7 pagesCancer and Its Treatment: An OverviewIJAR JOURNALNo ratings yet
- Test Bank For Exploring Medical Language 11th Edition by Myrna Lafleur BrooksDocument57 pagesTest Bank For Exploring Medical Language 11th Edition by Myrna Lafleur Brooksmarcuskenyatta275No ratings yet
- Irfan's Shukar BookDocument56 pagesIrfan's Shukar BookHina MalikNo ratings yet
- Chapter: Evolution and Human Health and Disease: BIOLOGY - AssignmentDocument10 pagesChapter: Evolution and Human Health and Disease: BIOLOGY - Assignmentyogesh ahireNo ratings yet
- Clinical Manifestations, Differential Diagnosis, and Clinical Evaluation of A Palpable Breast Mass - UpToDateDocument17 pagesClinical Manifestations, Differential Diagnosis, and Clinical Evaluation of A Palpable Breast Mass - UpToDateariel cobosNo ratings yet
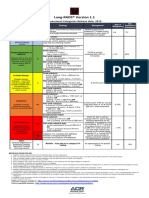
- Lung RADS® Version 1.1: Assessment Categories Release Date: 2019Document1 pageLung RADS® Version 1.1: Assessment Categories Release Date: 2019S Francisco MotNo ratings yet
- Part 1 Student NCM 112 Oncology NotesDocument12 pagesPart 1 Student NCM 112 Oncology NotesJohn Kenley FerryNo ratings yet
- International 3Document3 pagesInternational 3daffunkmadansyahNo ratings yet
- Pathology Chapterwise Year Questions. 2nd Yr BdsDocument10 pagesPathology Chapterwise Year Questions. 2nd Yr Bds76 S.SHRAVAN KUMARNo ratings yet
- Big Data Analytics To Predict Breast CancerDocument8 pagesBig Data Analytics To Predict Breast CancerIJRASETPublicationsNo ratings yet
- Final Draft Study Material Ranchi Region-1Document89 pagesFinal Draft Study Material Ranchi Region-1Chitransh AwasthiNo ratings yet
- Table of Surgical)Document98 pagesTable of Surgical)Bilal AhmadNo ratings yet
- Application of Knowledge QuestionsDocument16 pagesApplication of Knowledge QuestionsElllie TattersNo ratings yet
- Oncology McqsDocument115 pagesOncology McqsSyed NoorNo ratings yet
- Health 7 4th Quarter LasDocument17 pagesHealth 7 4th Quarter Lassarah jane ocenar100% (2)
- Pathology Course Audit-3Document26 pagesPathology Course Audit-3Joana Marie PalatanNo ratings yet
- M5 BIO111 Assignment1Document7 pagesM5 BIO111 Assignment1Kyle DunnNo ratings yet
- Medical Examination ReportDocument23 pagesMedical Examination Report李文No ratings yet
- Lytic Bone Lesions - StatPearls - NCBI BookshelfDocument9 pagesLytic Bone Lesions - StatPearls - NCBI Bookshelfjuan ricardo carvajal alvaradoNo ratings yet
- Cancer FungusDocument7 pagesCancer FungusAllison HobbsNo ratings yet
- Spirituality, Hope and Wisdom in Cancer PatientsDocument5 pagesSpirituality, Hope and Wisdom in Cancer PatientsIJAR JOURNALNo ratings yet
- Prefixes Suffixes RootsDocument4 pagesPrefixes Suffixes RootsZahoor Ul HaqNo ratings yet
- 57-2-3 BiologyDocument19 pages57-2-3 BiologyRavneet KaurNo ratings yet