You might also like
- Research Article: Prone Position After Liberation From Prolonged Mechanical Ventilation in COVID-19 Respiratory FailureDocument7 pagesResearch Article: Prone Position After Liberation From Prolonged Mechanical Ventilation in COVID-19 Respiratory FailurewiwiNo ratings yet
- 1807 5932 Clin 75 E2021Document2 pages1807 5932 Clin 75 E2021Claudia Lorena MedinaNo ratings yet
- Guidance On RehabilitationDocument67 pagesGuidance On RehabilitationJimmyNo ratings yet
- Gaudry2017 Article PronePositioningInAcuteRespiraDocument8 pagesGaudry2017 Article PronePositioningInAcuteRespiraEmmanuel Guar HuaNo ratings yet
- Journal Appraisal 2Document14 pagesJournal Appraisal 2Norjetalexis Maningo CabreraNo ratings yet
- Article in Press: Nasal High - Ow Oxygen Therapy in Icu: A Before-And-After StudyDocument6 pagesArticle in Press: Nasal High - Ow Oxygen Therapy in Icu: A Before-And-After StudyCharah IC NuRseNo ratings yet
- Papers Intervencion CovidDocument6 pagesPapers Intervencion Coviddayllyn iglesiasNo ratings yet
- 2015 Article 159Document8 pages2015 Article 159andri anaNo ratings yet
- Covid Critical Ill NutritionDocument9 pagesCovid Critical Ill NutritionRizqaFebrilianyNo ratings yet
- Original ArticleDocument8 pagesOriginal ArticleRania T.No ratings yet
- Effects of Oral Intake of WateDocument11 pagesEffects of Oral Intake of WateChenNo ratings yet
- 1705128278galley Proof-Knowledge, Attitude and Practice and Associated Factors On Oxygen Therapy Among Nurses and Midwives in Y12 HMC-2022 GCDocument11 pages1705128278galley Proof-Knowledge, Attitude and Practice and Associated Factors On Oxygen Therapy Among Nurses and Midwives in Y12 HMC-2022 GCKirubel TesfayeNo ratings yet
- COVID-19 Disease Invasive VentilationDocument8 pagesCOVID-19 Disease Invasive VentilationfikriafisNo ratings yet
- Jurnal Anestesi 3Document8 pagesJurnal Anestesi 3Rizky Frida Monica TomasilaNo ratings yet
- High Flow Oxygen Therapy V Standard Care in InfantsDocument5 pagesHigh Flow Oxygen Therapy V Standard Care in InfantsJaque ArandaNo ratings yet
- Clinical Profile and Outcome of Covid-19 Patients With Requirement of Oxygen Therapy For Greater Than One WeekDocument3 pagesClinical Profile and Outcome of Covid-19 Patients With Requirement of Oxygen Therapy For Greater Than One WeekIJAR JOURNALNo ratings yet
- Application of High-Fow Nasal CannulaDocument7 pagesApplication of High-Fow Nasal CannulaCLAUDIANo ratings yet
- Telerehab InterventionDocument12 pagesTelerehab InterventionNelson LoboNo ratings yet
- Nutrition Therapy COVID 19 SCCM ASPENDocument8 pagesNutrition Therapy COVID 19 SCCM ASPENtomtranNo ratings yet
- Journal of Critical Care: ArticleinfoDocument7 pagesJournal of Critical Care: ArticleinfoNindy CantikNo ratings yet
- Manual Proning and COVID-19 OutcomesDocument9 pagesManual Proning and COVID-19 Outcomesapi-587935422No ratings yet
- Daily Interruption of Sedation in Patients Treated With Mechanical VentilationDocument4 pagesDaily Interruption of Sedation in Patients Treated With Mechanical VentilationMark_LiGx_8269No ratings yet
- 2020 06 22 20137273v1 Full PDFDocument24 pages2020 06 22 20137273v1 Full PDFeswarNo ratings yet
- Physiotherapy and Weaning From Prolonged Mechanical VentilationDocument9 pagesPhysiotherapy and Weaning From Prolonged Mechanical VentilationdanielNo ratings yet
- Biblio Ms Abcrisis NCM 107 1Document3 pagesBiblio Ms Abcrisis NCM 107 1Nica SalazarNo ratings yet
- JPEN 9999 NaDocument28 pagesJPEN 9999 NaedithNo ratings yet
- Non InvasiveventilationDocument10 pagesNon InvasiveventilationpiusputraNo ratings yet
- A Proposal For Multidisciplinary Tele-Rehabilitation in The Assessment and Rehabilitation of COVID-19 SurvivorsDocument11 pagesA Proposal For Multidisciplinary Tele-Rehabilitation in The Assessment and Rehabilitation of COVID-19 Survivorsnidya yunazNo ratings yet
- 5794 22276 2 PBDocument4 pages5794 22276 2 PBalifa ishmahdinaNo ratings yet
- Prone For COVID: Are You Awake?: EditorialDocument2 pagesProne For COVID: Are You Awake?: EditorialMahtosurup GodavarthyNo ratings yet
- 2444 054X Cicr 91 04 479Document7 pages2444 054X Cicr 91 04 479Marìa GuevaraNo ratings yet
- Early Versus Late Awake Prone Positioning in Non-Intubated Patients With COVID-19Document9 pagesEarly Versus Late Awake Prone Positioning in Non-Intubated Patients With COVID-19Fadil AhmadNo ratings yet
- Early View: A Randomised Trial of High-Flow Nasal Cannula in Infants With Moderate BronchiolitisDocument28 pagesEarly View: A Randomised Trial of High-Flow Nasal Cannula in Infants With Moderate BronchiolitisutamiprakosoNo ratings yet
- !an Integrated Multidisciplinary Model of COVID-19 Recovery CareDocument8 pages!an Integrated Multidisciplinary Model of COVID-19 Recovery CareCARLA CRISTINA DE ARAUJONo ratings yet
- Vap Care Bundle FinalDocument4 pagesVap Care Bundle FinalMother of Mercy Hospital -Tacloban Inc.No ratings yet
- Nutrition CoviddDocument3 pagesNutrition CoviddYuly Asih WidiyaningrumNo ratings yet
- Airway Management in Pre-Hospital Critical Care: A Review of The Evidence For A Top Five ' Research PriorityDocument6 pagesAirway Management in Pre-Hospital Critical Care: A Review of The Evidence For A Top Five ' Research PriorityMeska AmeliaNo ratings yet
- Helmet CPAP Vs HFNC Clinical TrialDocument19 pagesHelmet CPAP Vs HFNC Clinical TrialTaufik RiansyahNo ratings yet
- Use of High-Flow Nasal Cannula Oxygen Therapy To Prevent Desaturation During Tracheal Intubation of Intensive Care Patients With Mild-to-Moderate HypoxemiaDocument10 pagesUse of High-Flow Nasal Cannula Oxygen Therapy To Prevent Desaturation During Tracheal Intubation of Intensive Care Patients With Mild-to-Moderate HypoxemiaLingga AniNo ratings yet
- Ventilatorweaningand Extubation: Karen E.A. Burns,, Bram Rochwerg, Andrew J.E. SeelyDocument18 pagesVentilatorweaningand Extubation: Karen E.A. Burns,, Bram Rochwerg, Andrew J.E. Seelyأركان هيلث Arkan healthNo ratings yet
- Awake Proning or Repositioning in Covid-19 PatientDocument4 pagesAwake Proning or Repositioning in Covid-19 PatientIJAR JOURNALNo ratings yet
- A Comprehensive Protocol For Ventilator Weaning and ExtubationDocument9 pagesA Comprehensive Protocol For Ventilator Weaning and ExtubationPaulaNo ratings yet
- Original: Intensive Care Med (2021) 47:1295-1302Document8 pagesOriginal: Intensive Care Med (2021) 47:1295-1302Andrea Ruiz LópezNo ratings yet
- Geriatric Nursing: Canan Karadas, MSC, Leyla Ozdemir, RN, PHDDocument6 pagesGeriatric Nursing: Canan Karadas, MSC, Leyla Ozdemir, RN, PHDCharah IC NuRseNo ratings yet
- Acute Life-Threatening Hypoxemia During Mechanical VentilationDocument8 pagesAcute Life-Threatening Hypoxemia During Mechanical VentilationCesar Rivas CamposNo ratings yet
- Journal Reading Marsya Y. Loppies (201283003)Document9 pagesJournal Reading Marsya Y. Loppies (201283003)joions gilberth oppiesNo ratings yet
- Pediatric Anesthesia - 2022 - Weatherall - Developing An Extubation Strategy For The Difficult Pediatric Airway Who WhenDocument8 pagesPediatric Anesthesia - 2022 - Weatherall - Developing An Extubation Strategy For The Difficult Pediatric Airway Who WhenPamela Mamani FloresNo ratings yet
- 1 BernardesDocument14 pages1 Bernardescesia llancaoNo ratings yet
- Title: Effect of Balloon-Blowing On Dyspnea and Oxygenation in Noncritical Adult Covid19 Patients: A Pilot StudyDocument17 pagesTitle: Effect of Balloon-Blowing On Dyspnea and Oxygenation in Noncritical Adult Covid19 Patients: A Pilot Studyelieser toding mendilaNo ratings yet
- AULA 06 Intravenous To OralDocument9 pagesAULA 06 Intravenous To OralRenataFonsecaNo ratings yet
- Impact Vap Bundle 2017Document6 pagesImpact Vap Bundle 2017Elisya KharuniawatiNo ratings yet
- C 8 F 0 CF 2 F 9 C 13052842 DDocument11 pagesC 8 F 0 CF 2 F 9 C 13052842 DDewi Ji YongNo ratings yet
- Innovative Physiotherapy Clinical Education in Response To The COVID-19 Pandemic With A Clinical Research Placement ModelDocument3 pagesInnovative Physiotherapy Clinical Education in Response To The COVID-19 Pandemic With A Clinical Research Placement ModelGeysel SuarezNo ratings yet
- Use of A Shared Canister Protocol For The Delivery of Metered-Dose Inhalers in Mechanically Ventilated SubjectsDocument8 pagesUse of A Shared Canister Protocol For The Delivery of Metered-Dose Inhalers in Mechanically Ventilated SubjectsevyNo ratings yet
- Farach 2014Document5 pagesFarach 2014mia widiastutiNo ratings yet
- Research PaperDocument11 pagesResearch Paperapi-625175559No ratings yet
- Could Physical Therapy Interventions Be Adopted in The Management of Critically Ill Patients With COVID-19? A Scoping ReviewDocument18 pagesCould Physical Therapy Interventions Be Adopted in The Management of Critically Ill Patients With COVID-19? A Scoping ReviewFernando JarixNo ratings yet
- Acute Respiratory Distress Syndrome (ARDS) Developed Clinical Pathway: Suggested ProtocolDocument6 pagesAcute Respiratory Distress Syndrome (ARDS) Developed Clinical Pathway: Suggested ProtocolRia sasmitaNo ratings yet
- Essentials in Lung TransplantationFrom EverandEssentials in Lung TransplantationAllan R. GlanvilleNo ratings yet
- ENHANZE® Drug Delivery Technology: Advancing Subcutaneous Drug Delivery using Recombinant Human Hyaluronidase PH20From EverandENHANZE® Drug Delivery Technology: Advancing Subcutaneous Drug Delivery using Recombinant Human Hyaluronidase PH20No ratings yet
- HIV ManagmentDocument44 pagesHIV ManagmentSarvesh PatilNo ratings yet
- Admission HospitalDocument7 pagesAdmission HospitalYuhuuNo ratings yet
- NCP GiDocument6 pagesNCP GiTroy MagcalasNo ratings yet
- nsg-320cc Careplan 4Document12 pagesnsg-320cc Careplan 4api-509452165No ratings yet
- 11 Lumbar LaminectomyDocument3 pages11 Lumbar LaminectomyIndah ChristyNo ratings yet
- What Is Medical Technology?Document5 pagesWhat Is Medical Technology?Bernadine Salado100% (1)
- Care Planning ToolkitDocument47 pagesCare Planning ToolkitAjeet YadavNo ratings yet
- A Postpartum Vaccination PromotionDocument8 pagesA Postpartum Vaccination Promotionanon_327352238No ratings yet
- Ghid Resuscitare Europ 2021Document25 pagesGhid Resuscitare Europ 2021Crisan Elena-simonaNo ratings yet
- The Appreciative InquiryDocument4 pagesThe Appreciative InquiryGilbert IskandarNo ratings yet
- Physiotherapy Advice After Abdominal SurgeryDocument8 pagesPhysiotherapy Advice After Abdominal SurgeryNewbieNo ratings yet
- Medical AnthropologyDocument5 pagesMedical Anthropologyankulin duwarahNo ratings yet
- Intercostal Nerve BlockDocument1 pageIntercostal Nerve BlockThunderboltA.LexaNo ratings yet
- Prenatal Development 1Document10 pagesPrenatal Development 1nate1425No ratings yet
- Burnout Research (Final)Document49 pagesBurnout Research (Final)rumman tariqNo ratings yet
- 10 Squamouspapilloma-ReportoftwocasesDocument7 pages10 Squamouspapilloma-ReportoftwocasesAyik DarkerThan BlackNo ratings yet
- DR Amr HassanDocument9 pagesDR Amr Hassanmohamed lotfyNo ratings yet
- 1 s2.0 S240589632201374X MainDocument6 pages1 s2.0 S240589632201374X MainApollonia VitelliNo ratings yet
- Legal-Med-Module For The BettermentDocument79 pagesLegal-Med-Module For The BettermentMjay MedinaNo ratings yet
- Cutaneous Manifestations of TuberculosisDocument35 pagesCutaneous Manifestations of TuberculosisSaid Plazola MercadoNo ratings yet
- Are Exercise Prescriptions For Patients WithDocument11 pagesAre Exercise Prescriptions For Patients Withnele657No ratings yet
- Caitlyn 211 CetDocument7 pagesCaitlyn 211 Cetapi-534410130No ratings yet
- Wma Medical Ethics ManualDocument71 pagesWma Medical Ethics ManualMatin Ahmad KhanNo ratings yet
- The Skeletal SystemDocument26 pagesThe Skeletal Systemapi-312562123No ratings yet
- PPP Listening Practice Test 7 Question PaperDocument12 pagesPPP Listening Practice Test 7 Question PaperhaffizmoradNo ratings yet
- Cone Beam CT Guided Radiotherapy: Jan-Jakob SonkeDocument64 pagesCone Beam CT Guided Radiotherapy: Jan-Jakob Sonkebabba241276No ratings yet
- Management of Hypoxia During AnaesthesiaDocument5 pagesManagement of Hypoxia During AnaesthesiaNurhafizahImfista100% (1)
- Colon and Rectum Colorectal CancerDocument20 pagesColon and Rectum Colorectal CancerJemima Nove JapitanaNo ratings yet
- The Original MayCo Zapper Is HereDocument15 pagesThe Original MayCo Zapper Is HereMariel Angela Bueno100% (1)
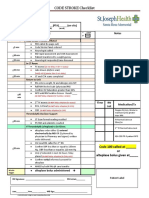
- CODE STROKE Checklist:: NotesDocument1 pageCODE STROKE Checklist:: NotesAdam MochtarNo ratings yet