You might also like
- Mind Power SecretsDocument38 pagesMind Power SecretsIan Faian92% (52)
- Aircraft Instruments and Avionics PDFDocument211 pagesAircraft Instruments and Avionics PDFairbuk doeing88% (8)
- Detox 101Document31 pagesDetox 101Botoşanu Diana-LarisaNo ratings yet
- Minutes of The MeetingDocument2 pagesMinutes of The MeetingJeremy Gaddi100% (1)
- Cochlear ImplantsDocument53 pagesCochlear ImplantsSovitJungBaralNo ratings yet
- Regenerative Endodontics Study GuideDocument21 pagesRegenerative Endodontics Study GuideKristineNo ratings yet
- Ibsen in PracticeDocument17 pagesIbsen in PracticevictorkalkaNo ratings yet
- Maximize muscle gains with reverse pyramid trainingDocument8 pagesMaximize muscle gains with reverse pyramid trainingMusadiq Ahmed100% (1)
- How Yeast Growth is AffectedDocument9 pagesHow Yeast Growth is AffectedMisika AlamNo ratings yet
- SC upholds reclusion perpetua for statutory rape within the familyDocument9 pagesSC upholds reclusion perpetua for statutory rape within the familymrvirginesNo ratings yet
- Schwarz Et Al (2018) - Peri Implantitis - 1Document23 pagesSchwarz Et Al (2018) - Peri Implantitis - 1FelipeOyarceSalazarNo ratings yet
- 4Y7zAw Ccrs23149Document12 pages4Y7zAw Ccrs23149Jefry JapNo ratings yet
- A Long-Term Study of 370 Autotransplanted Premolars.Document11 pagesA Long-Term Study of 370 Autotransplanted Premolars.jing.zhao222No ratings yet
- Management of Complex Anal FistulasDocument7 pagesManagement of Complex Anal Fistulasraka wibawa PutraNo ratings yet
- Abdalla 2017Document3 pagesAbdalla 2017dewaprasatyaNo ratings yet
- Cannulation Attempts and The Development of Post EDocument2 pagesCannulation Attempts and The Development of Post EMarcio MullerNo ratings yet
- Proforma For Registration of Subject For DissertationDocument12 pagesProforma For Registration of Subject For DissertationLijoeliyasNo ratings yet
- Closed Double-Lumen Suction Irrigation in The Management of Chronic Diaphyseal OsteomyelitisDocument6 pagesClosed Double-Lumen Suction Irrigation in The Management of Chronic Diaphyseal OsteomyelitisSonny WijanarkoNo ratings yet
- Role of Swallowing Function of Tracheotomised Patients in Major Head and Neck Cancer SurgeryDocument3 pagesRole of Swallowing Function of Tracheotomised Patients in Major Head and Neck Cancer SurgeryAnonymous xvlg4m5xLXNo ratings yet
- Advanced Platelet-Rich Fibrin A New Concept For Cell-Based Tissue Engineering by Means of Inflammatory CellsDocument11 pagesAdvanced Platelet-Rich Fibrin A New Concept For Cell-Based Tissue Engineering by Means of Inflammatory CellsmaxNo ratings yet
- Comparative Anatomical Analysis of The Transcallosal-Transchoroidal and Transcallosal-Transforniceal-Transchoroidal Approaches To The Third VentricleDocument10 pagesComparative Anatomical Analysis of The Transcallosal-Transchoroidal and Transcallosal-Transforniceal-Transchoroidal Approaches To The Third VentricleZeptalanNo ratings yet
- 1 - Prevalence of Maxillary Sinus SeptaDocument9 pages1 - Prevalence of Maxillary Sinus SeptaLamis MagdyNo ratings yet
- KumarasingheDocument4 pagesKumarasingheVitta Kusma WijayaNo ratings yet
- 1 s2.0 S174391911100553X MainDocument6 pages1 s2.0 S174391911100553X MainAndrea RodríguezNo ratings yet
- Sauer Bier 2010Document10 pagesSauer Bier 2010abdelrahman s.hassopaNo ratings yet
- RETRACTED The First Tissue Engineered Airway TranDocument7 pagesRETRACTED The First Tissue Engineered Airway TranJoni SiahaanNo ratings yet
- Fistulectomy With Primary Sphincter Reconstruction: What Does This Paper Add To The Literature?Document9 pagesFistulectomy With Primary Sphincter Reconstruction: What Does This Paper Add To The Literature?miguelNo ratings yet
- Fistula Ani Japanese GuidelineDocument7 pagesFistula Ani Japanese GuidelinevivianmtNo ratings yet
- Poh 2011Document8 pagesPoh 2011DH SiriruiNo ratings yet
- A Long-Term Study of 370 Autotransplanted Premolars. Part II. Tooth Survival and Pulp Healing Subsequent To TransplantationDocument11 pagesA Long-Term Study of 370 Autotransplanted Premolars. Part II. Tooth Survival and Pulp Healing Subsequent To TransplantationRudnapon AmornlaksananonNo ratings yet
- Autologus Fibroblast InjectionsDocument14 pagesAutologus Fibroblast InjectionsDr. DeeptiNo ratings yet
- Free Flap Thrombosis in Patients With Hypercoagulability: A Systematic ReviewDocument8 pagesFree Flap Thrombosis in Patients With Hypercoagulability: A Systematic ReviewDiego PerezNo ratings yet
- Lungs Regeneration Tao 2018Document27 pagesLungs Regeneration Tao 2018José Antonio Silva NetoNo ratings yet
- 10.1055@s 0039 1693992Document8 pages10.1055@s 0039 1693992Claudia Sughey Herrera PalominoNo ratings yet
- Prevalence of Maxillary Sinus Septa: Systematic Review and Meta-AnalysisDocument9 pagesPrevalence of Maxillary Sinus Septa: Systematic Review and Meta-AnalysisDennis DinellyNo ratings yet
- Hyareetal 2010Document9 pagesHyareetal 2010DanielMahendraNo ratings yet
- Oronasal Fistula Formation Post Cleft RepairDocument7 pagesOronasal Fistula Formation Post Cleft RepairMiguelito JohnsonNo ratings yet
- Meta-Analysis of Closure of The Fascial Defect During Laparoscopic Incisional and Ventral Hernia RepairDocument10 pagesMeta-Analysis of Closure of The Fascial Defect During Laparoscopic Incisional and Ventral Hernia RepairUday PrabhuNo ratings yet
- Recurrent Groin HerniaDocument6 pagesRecurrent Groin HerniaJohn-adewaleSmithNo ratings yet
- Comparative Study Between Open Fistulectomy and Ligation of Intersphincteric Fistulas Tract (LIFT) Procedure For Uncomplicated Perianal FistulaDocument7 pagesComparative Study Between Open Fistulectomy and Ligation of Intersphincteric Fistulas Tract (LIFT) Procedure For Uncomplicated Perianal FistulaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- fissure dilationDocument5 pagesfissure dilationIbrahim AlmoosaNo ratings yet
- Flap Surgical Techniques For Incisional Hernia Recurrences. A Swine Experimental ModelDocument9 pagesFlap Surgical Techniques For Incisional Hernia Recurrences. A Swine Experimental ModelFlorina PopaNo ratings yet
- Tensimektoki Terhadap Imun SistemDocument7 pagesTensimektoki Terhadap Imun SistemIndri yaniNo ratings yet
- Infundibulo-Tuberal or Not Strictly Intraventricular Craniopharyngioma: Evidence For A Major Topographical CategoryDocument24 pagesInfundibulo-Tuberal or Not Strictly Intraventricular Craniopharyngioma: Evidence For A Major Topographical CategoryAmina GoharyNo ratings yet
- Epidermoid Cysts TNEDocument10 pagesEpidermoid Cysts TNEbello_england_209552No ratings yet
- Etiology of Late Free Flap Failures Occurring After Hospital Discharge 2007Document3 pagesEtiology of Late Free Flap Failures Occurring After Hospital Discharge 2007Nanna de VengerbergNo ratings yet
- Yun DKK - 2010 - Regional Distribution ICC in GasterDocument8 pagesYun DKK - 2010 - Regional Distribution ICC in Gasterida aprianiNo ratings yet
- 2011 Coronectomy of The Lower Third Molar Is Safe Within The First 3 YearsDocument8 pages2011 Coronectomy of The Lower Third Molar Is Safe Within The First 3 YearskaarlaamendezNo ratings yet
- Daigle-Boerema Gastropexy PEHDocument7 pagesDaigle-Boerema Gastropexy PEHGunduz AgaNo ratings yet
- Clin Physio Funct Imaging - 2013 - Munkholm - Mucociliary Clearance Pathophysiological AspectsDocument7 pagesClin Physio Funct Imaging - 2013 - Munkholm - Mucociliary Clearance Pathophysiological AspectsIkon ikonicNo ratings yet
- Thirty Years of Submental Intubation: A Review: Review Paper Oral SurgeryDocument5 pagesThirty Years of Submental Intubation: A Review: Review Paper Oral SurgeryUmer HussainNo ratings yet
- Investigation of Free-Flap Transfer Reconstruction in Elderly Patients and Oral Intake FunctionDocument3 pagesInvestigation of Free-Flap Transfer Reconstruction in Elderly Patients and Oral Intake Functioncusom34No ratings yet
- Novaes 1969Document13 pagesNovaes 1969Ana OrtizNo ratings yet
- Oral Field CancerizationDocument7 pagesOral Field CancerizationFarah UlyaNo ratings yet
- J Tripleo 2009 05 043Document8 pagesJ Tripleo 2009 05 043Sudheer KondakaNo ratings yet
- Primary Versus Secondary Tracheoesophageal Puncture: Systematic Review and Meta-AnalysisDocument8 pagesPrimary Versus Secondary Tracheoesophageal Puncture: Systematic Review and Meta-AnalysisIsrael BlancoNo ratings yet
- Modified Rives StoppaDocument8 pagesModified Rives StoppaAndrei SinNo ratings yet
- jcmm0017 1525Document12 pagesjcmm0017 1525Aya AlkaffNo ratings yet
- Pre Peritoneal LaparoscópicaDocument16 pagesPre Peritoneal Laparoscópicamarquete72100% (1)
- Detection of Apoptosis During Orthodontic Tooth Movement in RatsDocument6 pagesDetection of Apoptosis During Orthodontic Tooth Movement in RatsHusni mubarakNo ratings yet
- Benefits of Primary Thoracoscopic Treatment for Pediatric Pleural EmpyemaDocument9 pagesBenefits of Primary Thoracoscopic Treatment for Pediatric Pleural EmpyemaJHONATAN MATA ARANDANo ratings yet
- Decision Algỏithm and Surgical Strategies For Managing Trachecutaneous FistulaDocument9 pagesDecision Algỏithm and Surgical Strategies For Managing Trachecutaneous Fistulahai1No ratings yet
- Nihms 1796721Document17 pagesNihms 1796721CLINIC SURGERY 17THNo ratings yet
- Lymphedema Rates in Pedicled ALTP For Coverage in Irradiated Groin Defects 2019Document4 pagesLymphedema Rates in Pedicled ALTP For Coverage in Irradiated Groin Defects 2019yeapdshengNo ratings yet
- Surgical Treatment of Popliteal Cyst A SystematicDocument9 pagesSurgical Treatment of Popliteal Cyst A SystematicSri KarunNo ratings yet
- JIAP October 2011 - The Influence of Restorations and Prosthetic Crowns Finishing Lines On Inflammatory Levels After Non-Surgical Periodontal TherapyDocument8 pagesJIAP October 2011 - The Influence of Restorations and Prosthetic Crowns Finishing Lines On Inflammatory Levels After Non-Surgical Periodontal TherapyMedstudNo ratings yet
- Early Recurrence of Mandibular Torus Following SurDocument4 pagesEarly Recurrence of Mandibular Torus Following SurPaola GillNo ratings yet
- Robotic Hernia Surgery: A Comprehensive Illustrated GuideFrom EverandRobotic Hernia Surgery: A Comprehensive Illustrated GuideOmar Yusef KudsiNo ratings yet
- Cell Movement and Neoplasia: Proceedings of the Annual Meeting of the Cell Tissue and Organ Culture Study Group, Held at the Janssen Research Foundation, Beerse, Belgium, May 1979From EverandCell Movement and Neoplasia: Proceedings of the Annual Meeting of the Cell Tissue and Organ Culture Study Group, Held at the Janssen Research Foundation, Beerse, Belgium, May 1979M. De BrabanderRating: 5 out of 5 stars5/5 (1)
- Hiatal HerniaDocument63 pagesHiatal HerniaCandace LongNo ratings yet
- Surgical Management of Diabetic Foot Ulcers: September 2012Document16 pagesSurgical Management of Diabetic Foot Ulcers: September 2012polin timiselaNo ratings yet
- HerniaDocument47 pagesHerniaCandace LongNo ratings yet
- Because of UDocument1 pageBecause of UCandace LongNo ratings yet
- Surat Layak TerbangDocument1 pageSurat Layak TerbangCandace LongNo ratings yet
- Emergency Package Medical Supplies Adults ChildrenDocument1 pageEmergency Package Medical Supplies Adults ChildrenCandace LongNo ratings yet
- Estimasi Paket Sunat Massal SistemDocument2 pagesEstimasi Paket Sunat Massal SistemCandace LongNo ratings yet
- Clinical Pathway ObgynDocument1 pageClinical Pathway ObgynCandace LongNo ratings yet
- K01.0 K03.2 K03.0 K08.0 K06.2 K06.1 K06.0 K06.9 K03.0 K03.9 K03.4 K07.0 K.09 K04.8 C03 K00.3 K03.3 Z01.2 K04.6 K04.4 K04.5 K03.7 K04.2 K08.3 K08.9 K08 K00 K00.8Document1 pageK01.0 K03.2 K03.0 K08.0 K06.2 K06.1 K06.0 K06.9 K03.0 K03.9 K03.4 K07.0 K.09 K04.8 C03 K00.3 K03.3 Z01.2 K04.6 K04.4 K04.5 K03.7 K04.2 K08.3 K08.9 K08 K00 K00.8Candace LongNo ratings yet
- He Modi AlisaDocument1 pageHe Modi AlisaCandace LongNo ratings yet
- Alat Inventaris Maternity WardDocument4 pagesAlat Inventaris Maternity WardCandace LongNo ratings yet
- Budget ESWL Dan CATH LABDocument4 pagesBudget ESWL Dan CATH LABCandace LongNo ratings yet
- Budget WARDDocument4 pagesBudget WARDCandace LongNo ratings yet
- Paket Inhealth IGDDocument1 pagePaket Inhealth IGDCandace LongNo ratings yet
- Budget ESWL Dan CATH LABDocument4 pagesBudget ESWL Dan CATH LABCandace LongNo ratings yet
- AHA Guidelines For CPR and ECC Comparison Chart of Key Changes (2010)Document8 pagesAHA Guidelines For CPR and ECC Comparison Chart of Key Changes (2010)PhilippineNursingDirectory.comNo ratings yet
- Sedation DoseDocument3 pagesSedation DoseCandace LongNo ratings yet
- Aftercooler - Test: Shutdown SIS Previous ScreenDocument7 pagesAftercooler - Test: Shutdown SIS Previous ScreenKeron Trotz100% (1)
- Nikon Nivo C Series Instruction ManualDocument65 pagesNikon Nivo C Series Instruction ManualBambang Deriyanto100% (1)
- 0972 June 2021 QP 41 Cie Igcse Physics - Pdfquestion7Document2 pages0972 June 2021 QP 41 Cie Igcse Physics - Pdfquestion7Kareem YouakimNo ratings yet
- Supplying Ready Mix in Southeast Asia - Adapting Concrete Mix Design for Hot, Tropical WeatherDocument2 pagesSupplying Ready Mix in Southeast Asia - Adapting Concrete Mix Design for Hot, Tropical Weathermixtoes7647No ratings yet
- Cambridge O Level: English Language 1123/22Document4 pagesCambridge O Level: English Language 1123/22Shania SeneviratneNo ratings yet
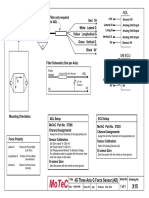
- Filter and wiring schematic for 3-axis ADL G-force sensorDocument1 pageFilter and wiring schematic for 3-axis ADL G-force sensorJuan Ramón Pérez LorenzoNo ratings yet
- Section - A: Holiday Homework For Grade XiDocument7 pagesSection - A: Holiday Homework For Grade XiGM Ali KawsarNo ratings yet
- Boiler Feedwater ControlDocument14 pagesBoiler Feedwater ControlJonas PeraterNo ratings yet
- Formula 1480 Rub Off Mask PDFDocument1 pageFormula 1480 Rub Off Mask PDFAbdul WasayNo ratings yet
- Report On PantaloonsDocument63 pagesReport On PantaloonsKashish AroraNo ratings yet
- Jear C PB 2018 PDFDocument174 pagesJear C PB 2018 PDFArasu RajendranNo ratings yet
- Midterm Exam Reviewer: Surgical Handwashing QuizDocument9 pagesMidterm Exam Reviewer: Surgical Handwashing QuizOfficially RandomNo ratings yet
- FBSUPRAPAKENDocument6 pagesFBSUPRAPAKENKontczey DavidNo ratings yet
- Diseases That Cause HypoproteinemiaDocument12 pagesDiseases That Cause HypoproteinemiaRachel Marie M. GaniaNo ratings yet
- Caffeine Natural Coffee BeanDocument1 pageCaffeine Natural Coffee BeanMayang TariNo ratings yet
- STD Comparison ChartDocument4 pagesSTD Comparison Chartabu ubaidahNo ratings yet
- Jadwal Oral Presentation Peserta FIT-VIIIDocument26 pagesJadwal Oral Presentation Peserta FIT-VIIIKlinik FellitaNo ratings yet
- Complementary Therapies in Clinical Practice: Effect of Aromatherapy On Post-Partum Complications: A Systematic ReviewDocument7 pagesComplementary Therapies in Clinical Practice: Effect of Aromatherapy On Post-Partum Complications: A Systematic ReviewAras PinantiNo ratings yet
- 4140DE Data SheetDocument1 page4140DE Data SheetNabeel AmeerNo ratings yet
- What Is A PronounDocument9 pagesWhat Is A PronounFanera JefferyNo ratings yet
- Group 3Document11 pagesGroup 3Sharp MIER TVNo ratings yet