You might also like
- The Esthetic Biological Contour Concept (Blatz) (2021)Document12 pagesThe Esthetic Biological Contour Concept (Blatz) (2021)Sofia Avila86% (7)
- 2021 The Esthetic Biological Contour Concept For Implant RestorationDocument12 pages2021 The Esthetic Biological Contour Concept For Implant RestorationOd. Valeria Gutierrez G100% (3)
- Testing and Commissioning For Cooling TowerDocument6 pagesTesting and Commissioning For Cooling TowerDong VanraNo ratings yet
- Geometric Considerations in AnteriorDocument11 pagesGeometric Considerations in AnteriorSebastián BernalNo ratings yet
- Biologic Esthetics by Gingival Framework Desing Part 2 Gingival EstheticsDocument13 pagesBiologic Esthetics by Gingival Framework Desing Part 2 Gingival EstheticsAna Veronica100% (2)
- 004 Articulo Estetica NishimuraDocument29 pages004 Articulo Estetica NishimuraJesusCordoba100% (1)
- A Didactic Concept Of: Dental MorphologyDocument9 pagesA Didactic Concept Of: Dental MorphologyErick Brañes Espinoza100% (1)
- Carranza 12e - Furcation Involvement and TreatmentDocument14 pagesCarranza 12e - Furcation Involvement and TreatmentK KNo ratings yet
- The Neutral Zone in Complete DenturesDocument8 pagesThe Neutral Zone in Complete DenturesToDownload81No ratings yet
- Topcon SL-D7 Slitlamp - Service ManualDocument40 pagesTopcon SL-D7 Slitlamp - Service ManualPablo MartínezNo ratings yet
- Experiment 1 - G13 PDFDocument20 pagesExperiment 1 - G13 PDFAllan ChongNo ratings yet
- Factores Macroesteticos en El Diseño de SonrisaDocument7 pagesFactores Macroesteticos en El Diseño de SonrisaJassel DurdenNo ratings yet
- Haptics - The Science of Touch in Dental TrainingDocument4 pagesHaptics - The Science of Touch in Dental TrainingInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- L'influence Des Incisives CentralesDocument6 pagesL'influence Des Incisives CentralesMajdou LineNo ratings yet
- Articulo Estetica Nishimura PDFDocument29 pagesArticulo Estetica Nishimura PDFDiana Lorena Moreno Vega100% (1)
- Aesthetics in Complete Denture - A REVIEWDocument2 pagesAesthetics in Complete Denture - A REVIEWInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Physiology of Tooth Form: FunctionDocument1 pagePhysiology of Tooth Form: FunctionTayyuba AslamNo ratings yet
- Esthetic Rehabilitation Evaluating Full Conservative Treatment.Document5 pagesEsthetic Rehabilitation Evaluating Full Conservative Treatment.floressam2000No ratings yet
- Waxing Techniques To Develop Proper Occlusal Morphology in Different Occlusal SchemesDocument6 pagesWaxing Techniques To Develop Proper Occlusal Morphology in Different Occlusal SchemesMihaela VasiliuNo ratings yet
- Emergence Angles of The Cej in Natural Max Ant TeethDocument8 pagesEmergence Angles of The Cej in Natural Max Ant TeethN&M CHANNELNo ratings yet
- Principles For Establishment of Esthetics in Fixed Prosthodontics A ReviewDocument12 pagesPrinciples For Establishment of Esthetics in Fixed Prosthodontics A ReviewDjoumana BentoumiNo ratings yet
- Aesthetics in Orthodontics: Six Horizontal Smile LinesDocument14 pagesAesthetics in Orthodontics: Six Horizontal Smile LinesPaulinaNo ratings yet
- Esthetic - Considerations - in - Orthodontics - An - Overview SECOND YEAR JC (FIRST)Document6 pagesEsthetic - Considerations - in - Orthodontics - An - Overview SECOND YEAR JC (FIRST)VEENA k.aNo ratings yet
- Esthetic and Phonetics in Complete Dentures: December 2011Document5 pagesEsthetic and Phonetics in Complete Dentures: December 2011AndreeaNo ratings yet
- Pietrokovski 2007Document7 pagesPietrokovski 2007vickydivi09No ratings yet
- 12-Aesthetics in Removable Prosthodontics - MahmoudDocument39 pages12-Aesthetics in Removable Prosthodontics - Mahmoudhassan.h.h.elhusseinyNo ratings yet
- Pneumocephalus As A Fatal But Very RareDocument27 pagesPneumocephalus As A Fatal But Very RareHossam ThabetNo ratings yet
- JCDP 19 624Document4 pagesJCDP 19 624Priyanka GandhiNo ratings yet
- Prosthodontics May 2015Document39 pagesProsthodontics May 2015samikshaNo ratings yet
- 03 CanineDocument12 pages03 Canine蕭亦No ratings yet
- Jco 1998 07 432Document14 pagesJco 1998 07 432Pulkit BimalNo ratings yet
- Smile DesignDocument64 pagesSmile Designbaskarend67% (6)
- Removable Prosthodontics: The Neutral Zone in Complete DenturesDocument12 pagesRemovable Prosthodontics: The Neutral Zone in Complete DenturesAsma Akram - ProsthodonticsNo ratings yet
- Biologic Width and Its Relation To PeriodontalDocument7 pagesBiologic Width and Its Relation To PeriodontalBethania CarolinaNo ratings yet
- Principles of Smile Design: Invited ReviewDocument8 pagesPrinciples of Smile Design: Invited ReviewamitNo ratings yet
- Abutment Evaluation in FPD 2Document5 pagesAbutment Evaluation in FPD 2ahmad955mlsNo ratings yet
- Cracked Tooth Syndrome: A Review of The LiteratureDocument8 pagesCracked Tooth Syndrome: A Review of The Literaturetexew44804No ratings yet
- Introduction To Dental Anatomy: Learning Objec TivesDocument12 pagesIntroduction To Dental Anatomy: Learning Objec Tivesbalkiz mahamedNo ratings yet
- A Review of Root Fractures Diagnosis Treatment and PDFDocument10 pagesA Review of Root Fractures Diagnosis Treatment and PDFaadil thimwalaNo ratings yet
- MicroestheticsDocument7 pagesMicroestheticsVasanthavalli DevanathanNo ratings yet
- The Aesthetic Smile: Diagnosis Treatment: Garber SalamaDocument11 pagesThe Aesthetic Smile: Diagnosis Treatment: Garber SalamaAdriana RibeiroNo ratings yet
- A Review of Root Fractures Diagnosis Treatment and PDFDocument10 pagesA Review of Root Fractures Diagnosis Treatment and PDFMinh Nhat Le ThanhNo ratings yet
- Selection of Teeth & Arrangement of Teeth: Praveen V BadwaikDocument46 pagesSelection of Teeth & Arrangement of Teeth: Praveen V BadwaikPraveen BadwaikNo ratings yet
- Garib (2010) - Alveolar Bone Morphology Under The Perspective of The Computed Tomography. Defining The Biological Limits of Tooth Movement PDFDocument15 pagesGarib (2010) - Alveolar Bone Morphology Under The Perspective of The Computed Tomography. Defining The Biological Limits of Tooth Movement PDFIsmaelLouGomezNo ratings yet
- Micro and Macro Dental Esthetics: The Key To Smile IndividualizationDocument14 pagesMicro and Macro Dental Esthetics: The Key To Smile IndividualizationRoo GaunaNo ratings yet
- AbcDocument4 pagesAbcAquinnaNo ratings yet
- Significance of Facebow For Dental RestorationsDocument5 pagesSignificance of Facebow For Dental RestorationsMahmoud Ibrahem maanNo ratings yet
- Guia Anterior - Gonzalez Hernandez-61-2Document12 pagesGuia Anterior - Gonzalez Hernandez-61-2Fred TorresNo ratings yet
- Significance of Facebow For Dental RestorationsDocument5 pagesSignificance of Facebow For Dental RestorationsSahana RangarajanNo ratings yet
- Chang2004 2Document8 pagesChang2004 2AlfonsoNo ratings yet
- Nine Steps To Occlusal Harmony FamdentDocument5 pagesNine Steps To Occlusal Harmony FamdentGhenciu Violeta100% (1)
- The Importance of Treating Functional Cross Bite A Clinical ViewpointDocument7 pagesThe Importance of Treating Functional Cross Bite A Clinical ViewpointAna María ReyesNo ratings yet
- Neutral Zone FinalDocument37 pagesNeutral Zone FinalJyoti Tripathi100% (1)
- Symmetry 13 01741Document19 pagesSymmetry 13 01741Carina NicoleNo ratings yet
- The Fate of The Distal Papilla Around Tooth-Bound Implant-Supported Restorations in Maxillary Central Incisor SitesDocument7 pagesThe Fate of The Distal Papilla Around Tooth-Bound Implant-Supported Restorations in Maxillary Central Incisor SitesValentinaNo ratings yet
- The Orthodontic/Restorative Interface. Restorative Procedures To Aid Orthodontic TreatmentDocument11 pagesThe Orthodontic/Restorative Interface. Restorative Procedures To Aid Orthodontic TreatmentNeelash KrishnaNo ratings yet
- Significance of Facebow For Dental Restorations: September 2014Document5 pagesSignificance of Facebow For Dental Restorations: September 2014AnuRaveendranNo ratings yet
- Principles of Smile DesignDocument2 pagesPrinciples of Smile DesignChristopher PriceNo ratings yet
- Implant Esthetics: Review ArticleDocument6 pagesImplant Esthetics: Review ArticleSahana RangarajanNo ratings yet
- Orthodontically Driven Corticotomy: Tissue Engineering to Enhance Orthodontic and Multidisciplinary TreatmentFrom EverandOrthodontically Driven Corticotomy: Tissue Engineering to Enhance Orthodontic and Multidisciplinary TreatmentFederico BrugnamiNo ratings yet
- Design of 360 Degree Steering System: Saransh Tiwari Dr. Rajeev AryaDocument6 pagesDesign of 360 Degree Steering System: Saransh Tiwari Dr. Rajeev AryaAkarsh AdiNo ratings yet
- People - Information Processing and Transmission LabDocument1 pagePeople - Information Processing and Transmission Labmahmood sky13571No ratings yet
- Experiment 3: Fatty Acid Determination Using Gas Chromatography (GC)Document12 pagesExperiment 3: Fatty Acid Determination Using Gas Chromatography (GC)nur hafikah mustaphaNo ratings yet
- Equipment Data Sheet Lift N LockDocument4 pagesEquipment Data Sheet Lift N LockJesus LopezNo ratings yet
- CE 370 Tutorial Note 4Document5 pagesCE 370 Tutorial Note 4Ibrahim AlmohannaNo ratings yet
- 3G4 Distillation CalculationsDocument22 pages3G4 Distillation Calculationsrkm_rkmNo ratings yet
- Vine RobotsDocument20 pagesVine Robotsdivya AshishNo ratings yet
- FREE Photoshop CC 2018 (32 & 64 Bit) Full Crack + Portable + Paid Plugins - Mac Win DownloadDocument7 pagesFREE Photoshop CC 2018 (32 & 64 Bit) Full Crack + Portable + Paid Plugins - Mac Win DownloadADDECC INFO INDIANo ratings yet
- Microjet Recorder E: Instruction ManualDocument99 pagesMicrojet Recorder E: Instruction ManualkmpoulosNo ratings yet
- Arcelor - Catalog Cu Palplanse Metalice - 2Document16 pagesArcelor - Catalog Cu Palplanse Metalice - 2S. Marius100% (1)
- Unit - 1 - Bricks PDFDocument105 pagesUnit - 1 - Bricks PDFChandana Chandran100% (1)
- Digital JewelleryDocument15 pagesDigital JewelleryRicha Mungali100% (1)
- 04 - Modul Simulasi Impetus Physics 2021Document162 pages04 - Modul Simulasi Impetus Physics 2021Doraemon Music100% (2)
- bkc19 PDFDocument25 pagesbkc19 PDFrohitrgt4uNo ratings yet
- Floor PlansDocument11 pagesFloor PlansDaniel KoloNo ratings yet
- 3-Lesson Notes Lecture 1Document11 pages3-Lesson Notes Lecture 1José Diogo ForteNo ratings yet
- Part3 Q A Marine EngineerDocument10 pagesPart3 Q A Marine Engineer12345No ratings yet
- MT87Document2 pagesMT87Jenalyn Orbasido EvangelistaNo ratings yet
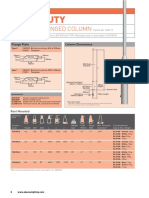
- Light Duty: 4-8M Base Hinged ColumnDocument3 pagesLight Duty: 4-8M Base Hinged ColumnAbrar AhmadNo ratings yet
- Manual Evo DSP Plus TT 10-20-30!40!60 Ita EngDocument100 pagesManual Evo DSP Plus TT 10-20-30!40!60 Ita Enghytham.midani.63No ratings yet
- Carlin GarwinDocument16 pagesCarlin GarwinGalih 'djawa' Parikesit100% (1)
- Drager Flame 1300 Instrument SpecificationDocument1 pageDrager Flame 1300 Instrument SpecificationjulioNo ratings yet
- MBA-BS-Recap Session Model Questions-13-07-2023-SV1Document74 pagesMBA-BS-Recap Session Model Questions-13-07-2023-SV1seyon sithamparanathanNo ratings yet
- 9709 Mathematics Paper4 Example Candidate ResponsesDocument38 pages9709 Mathematics Paper4 Example Candidate ResponsesWalid AamirNo ratings yet
- Performance Tuning - Expert PanelDocument135 pagesPerformance Tuning - Expert Panelagathian0% (1)
- Physical Examination and Health Assessment Canadian 2Nd Edition Jarvis Solutions Manual Full Chapter PDFDocument25 pagesPhysical Examination and Health Assessment Canadian 2Nd Edition Jarvis Solutions Manual Full Chapter PDFlegacycuttinglkhd100% (9)
- Modelling and Control of A Spray Drying ProcessDocument225 pagesModelling and Control of A Spray Drying ProcessAdrian García MoyanoNo ratings yet