You might also like
- Kidney Diet Secrets BookDocument175 pagesKidney Diet Secrets BookNikKiCasiño100% (1)
- Autism Spectrum DisorderDocument60 pagesAutism Spectrum DisorderPriyash JainNo ratings yet
- SOAP Notes Format in EMR: SOAP Stands For Subjective, Objective, Assessment, and PlanDocument2 pagesSOAP Notes Format in EMR: SOAP Stands For Subjective, Objective, Assessment, and PlanNick Jacob100% (7)
- Surgical Treatment of Hip Arthritis PDFDocument523 pagesSurgical Treatment of Hip Arthritis PDFMaria RamonaNo ratings yet
- Axa PhilDocument13 pagesAxa PhilKat EspanoNo ratings yet
- MCQ OphthalmologyDocument206 pagesMCQ OphthalmologyMohammed Mousa Imran100% (4)
- GRE Words List TestDocument38 pagesGRE Words List TestAsif Iqbal100% (1)
- NCPDocument3 pagesNCPranee diane0% (1)
- Oral Medicine and Radiology MCQDocument7 pagesOral Medicine and Radiology MCQsamhita100% (1)
- Fasting, Nature"s Best Remedy, Albert MosseriDocument76 pagesFasting, Nature"s Best Remedy, Albert MosseriAnonymous fO8xe7rMyA100% (2)
- The Casket of MedicineDocument104 pagesThe Casket of Medicinejivasumana100% (4)
- Eye Docs RetinaDocument279 pagesEye Docs RetinaRahul LokhandeNo ratings yet
- Oral Hygiene in VentilatorDocument136 pagesOral Hygiene in VentilatorFelicia Risca RyandiniNo ratings yet
- Coats Disease: Classification and Treatment: by Rishav Kansal, Bs Kiran Turaka, MD and Carol L. Shields, MDDocument3 pagesCoats Disease: Classification and Treatment: by Rishav Kansal, Bs Kiran Turaka, MD and Carol L. Shields, MDAnggie Imaniah SitompulNo ratings yet
- Ocular Ischemic Syndrome Survey OphthalmologyDocument33 pagesOcular Ischemic Syndrome Survey OphthalmologyamaiacNo ratings yet
- DHF Central Artery OclusionDocument2 pagesDHF Central Artery OclusionRia Septi HarmiaNo ratings yet
- Keratoconus in Cogan ReeseDocument3 pagesKeratoconus in Cogan ReeseDr. Abhishek OnkarNo ratings yet
- Iridocorneal Endothelial Syndrome in A 16-Year-OldDocument4 pagesIridocorneal Endothelial Syndrome in A 16-Year-OldCamiCasasNo ratings yet
- Clinicopathologic Reports, Case Reports, and Small Case SeriesDocument3 pagesClinicopathologic Reports, Case Reports, and Small Case SeriesDiaz RandanilNo ratings yet
- Is Episcleritis Associated To Glaucoma?Document3 pagesIs Episcleritis Associated To Glaucoma?Alvin JulianNo ratings yet
- Optic Neuritis in Leprosy - 231215 - 030338Document2 pagesOptic Neuritis in Leprosy - 231215 - 030338dr samyNo ratings yet
- 100255-Article Text-1482-2-10-20220311Document6 pages100255-Article Text-1482-2-10-20220311Fachry RahmanNo ratings yet
- Spontaneous Association of Macular Hole and Choroidal Neovascularization: A Case ReportDocument4 pagesSpontaneous Association of Macular Hole and Choroidal Neovascularization: A Case ReportIJAR JOURNALNo ratings yet
- Smital Poster New-1-1Document11 pagesSmital Poster New-1-1Smital JaiswalNo ratings yet
- A Case of Angle-Closure Glaucoma, Cataract, Nanophthalmos and Spherophakia in Oculo-Dento-Digital SyndromeDocument3 pagesA Case of Angle-Closure Glaucoma, Cataract, Nanophthalmos and Spherophakia in Oculo-Dento-Digital SyndromeSriana K. LaliyoNo ratings yet
- Iridocorneal Endothelial Syndrome in A 14-Year-Old MaleDocument2 pagesIridocorneal Endothelial Syndrome in A 14-Year-Old MaleCamiCasasNo ratings yet
- Retninal Vein OcclusionDocument10 pagesRetninal Vein OcclusionuhibNo ratings yet
- Journal Casereport 1Document5 pagesJournal Casereport 1Arif MohammadNo ratings yet
- Retina Pearls: Recognizing and Managing Coats DiseaseDocument2 pagesRetina Pearls: Recognizing and Managing Coats DiseaseNur Asri AinunNo ratings yet
- Cogan With MEDocument4 pagesCogan With MEDr. Abhishek OnkarNo ratings yet
- Probable Vogt-Koyanagi-Harada Disease: A Case ReportDocument5 pagesProbable Vogt-Koyanagi-Harada Disease: A Case ReportIJAR JOURNALNo ratings yet
- Macular Edema As Unusual Presentation of Non-Arteritic Ischemic Optic Neuropathy (Naion)Document9 pagesMacular Edema As Unusual Presentation of Non-Arteritic Ischemic Optic Neuropathy (Naion)IJAR JOURNALNo ratings yet
- Indirect Carotid-Cavernous Fistula Mimicking Scleritis: MagesDocument1 pageIndirect Carotid-Cavernous Fistula Mimicking Scleritis: MagesClarithq LengguNo ratings yet
- Retina AnswersDocument5 pagesRetina AnswersKhushal Khan KakarNo ratings yet
- Cornea 2014 p1109Document4 pagesCornea 2014 p1109beny sidabutarNo ratings yet
- Diagnosis and Management of AniridiaDocument3 pagesDiagnosis and Management of AniridiaCretu Mihail SebastianNo ratings yet
- MyopiaDocument11 pagesMyopiablueiceNo ratings yet
- Acute Retinal Necrosis Following Contralateral Herpes Zoster OphthalmicusDocument4 pagesAcute Retinal Necrosis Following Contralateral Herpes Zoster Ophthalmicusnurul_sharaswatiNo ratings yet
- Orbital Apex Syndrome from Herpes Zoster OphthalmicusDocument4 pagesOrbital Apex Syndrome from Herpes Zoster OphthalmicusYosiita KartinaaNo ratings yet
- Central Serous Retinopathy: Michael Colucciello, MDDocument9 pagesCentral Serous Retinopathy: Michael Colucciello, MDRani Henty NovitaNo ratings yet
- Secondary Acute Angle Closure Attack As An Initial Presentation of A Novel Type of Systemic Lupus ErythematosusDocument4 pagesSecondary Acute Angle Closure Attack As An Initial Presentation of A Novel Type of Systemic Lupus ErythematosusPutri kartiniNo ratings yet
- Granuloma PiogenikDocument2 pagesGranuloma PiogenikVindhiya Lissa VioletthaNo ratings yet
- Hypertensive Retinopathy Presenting as Angle Closure Glaucoma CaseDocument5 pagesHypertensive Retinopathy Presenting as Angle Closure Glaucoma CaseyunjaealwaysNo ratings yet
- Revisi 3 Case ReportDocument8 pagesRevisi 3 Case Reportzazaza94No ratings yet
- Meta-analysis of genetic links to PACGDocument1 pageMeta-analysis of genetic links to PACGjuan jose mansillaNo ratings yet
- Sawyer 1976Document8 pagesSawyer 1976FrancescFranquesaNo ratings yet
- Articulo FistulaDocument6 pagesArticulo FistulaOpti MonturasNo ratings yet
- chiều sâu theo nhiều látDocument6 pageschiều sâu theo nhiều látkim bíchNo ratings yet
- Casereport Neuristic OptDocument3 pagesCasereport Neuristic OptItsirch AydinNo ratings yet
- Pupil Capture of Intraocular Lens in Vitrectomized Eye With Primary Pigment Dispersion SyndromeDocument2 pagesPupil Capture of Intraocular Lens in Vitrectomized Eye With Primary Pigment Dispersion SyndromeHuang WanjingNo ratings yet
- Cambridge Ophthalmological SymposiumDocument22 pagesCambridge Ophthalmological SymposiumvericaNo ratings yet
- Solitary Retinal Capillary Hemangioma in A Patient With Bilateral Chorioretinal ColobomaDocument4 pagesSolitary Retinal Capillary Hemangioma in A Patient With Bilateral Chorioretinal ColobomaViolin NurkhaNo ratings yet
- Multiple Sclerosis With Ophthalmologic Onset - Case ReportDocument5 pagesMultiple Sclerosis With Ophthalmologic Onset - Case ReportVannyNo ratings yet
- Case Report: A Case of Type II Bilateral Sturge - Weber SyndromeDocument3 pagesCase Report: A Case of Type II Bilateral Sturge - Weber SyndromeIOSRjournalNo ratings yet
- Diagnostic and Therapeutic Challenges: Edited by H. Richard McdonaldDocument4 pagesDiagnostic and Therapeutic Challenges: Edited by H. Richard McdonaldAndhi Riawan Eko WiikramatunggadewaNo ratings yet
- 01 e 503 AsnrDocument2 pages01 e 503 AsnrLiyanti RinceNo ratings yet
- Chronic Conjunctivitis From A Retained Contact LensDocument4 pagesChronic Conjunctivitis From A Retained Contact Lensnana nurdahliaNo ratings yet
- Recurrent Optic Neuritis As A Clinical Manifestation in Multiple Sclerosis A Case Report - Anisa Feby ArifaniDocument11 pagesRecurrent Optic Neuritis As A Clinical Manifestation in Multiple Sclerosis A Case Report - Anisa Feby Arifanidenny070111209No ratings yet
- The Association of Carotid Cavernous Fistula With Graves' Ophthalmopathy Brief CommunicationsDocument3 pagesThe Association of Carotid Cavernous Fistula With Graves' Ophthalmopathy Brief CommunicationsRiris SihotangNo ratings yet
- Cystoid Macular EdemaDocument5 pagesCystoid Macular EdemaAgnes Triana BasjaNo ratings yet
- Ophthal Notes PGDocument6 pagesOphthal Notes PGSwati TyagiNo ratings yet
- Retinal LaserDocument7 pagesRetinal LaserSandra BabuNo ratings yet
- Treatment options for angle-closure glaucoma based on stagingDocument13 pagesTreatment options for angle-closure glaucoma based on stagingcindy sweeteniaNo ratings yet
- Glaucoma, Pseudoexfoliation: Emedicine Specialtiesophthalmologyintraocular PressureDocument9 pagesGlaucoma, Pseudoexfoliation: Emedicine Specialtiesophthalmologyintraocular PressureChintya Dwi PutriNo ratings yet
- Keratoconus: Picture 1Document6 pagesKeratoconus: Picture 1BuiyiWongNo ratings yet
- Keratoconus: Picture 1Document6 pagesKeratoconus: Picture 1BuiyiWongNo ratings yet
- Jurnal BlefaritisDocument5 pagesJurnal BlefaritisAkhdan AufaNo ratings yet
- Acta Ophthalmologica Scandinavica - 2003 - ZdemirDocument4 pagesActa Ophthalmologica Scandinavica - 2003 - ZdemirDr. Abhishek OnkarNo ratings yet
- Complications in UveitisFrom EverandComplications in UveitisFrancesco PichiNo ratings yet
- Biology 9th Solving A Biological ProblemDocument5 pagesBiology 9th Solving A Biological Problemmhussainshigri786No ratings yet
- Gaint Cell Lesions UPLOADDocument176 pagesGaint Cell Lesions UPLOADAkshayNo ratings yet
- Guideline, Management of HypoglycemiaDocument5 pagesGuideline, Management of HypoglycemianellieauthorNo ratings yet
- World Breastfeeding Week 2011Document20 pagesWorld Breastfeeding Week 2011Annapurna DangetiNo ratings yet
- EBOOK Infection Control and Management of Hazardous Materials For The Dental Team Download Full Chapter PDF KindleDocument62 pagesEBOOK Infection Control and Management of Hazardous Materials For The Dental Team Download Full Chapter PDF Kindlemichael.carathers448100% (36)
- ImmunizationDocument16 pagesImmunizationShafie ElmiNo ratings yet
- Early Childhood CariesDocument3 pagesEarly Childhood CariessreshtamukhiNo ratings yet
- Remedy Options: Anxiety (Homeopathy)Document1 pageRemedy Options: Anxiety (Homeopathy)Amanda CamposNo ratings yet
- Peel 1996 - Cardiopulmonary System and Movement DysfunctionDocument8 pagesPeel 1996 - Cardiopulmonary System and Movement DysfunctionBeto ZamunérNo ratings yet
- NCP: Nursing Care Plan For Bone FracturesDocument8 pagesNCP: Nursing Care Plan For Bone FracturesElham TabaoNo ratings yet
- M.03 THE STRONGYLIDA - Hookworms - Dr. AyochokDocument7 pagesM.03 THE STRONGYLIDA - Hookworms - Dr. AyochokJohn Louis AguilaNo ratings yet
- Crs Peripheral Artery Disease - Billi Brian GeniroDocument21 pagesCrs Peripheral Artery Disease - Billi Brian Genirofathiya nurkhalisaNo ratings yet
- OctreotideDocument12 pagesOctreotiderpadmakrishnanNo ratings yet
- 6th Science Source of Food Notes PDFDocument2 pages6th Science Source of Food Notes PDFPankaj ARORANo ratings yet
- Paediatric NeuroanaesthesiaDocument28 pagesPaediatric Neuroanaesthesiakoolstarone100% (1)
- Lesson 2-Introduction To The ICD-10-CM ClassificationDocument10 pagesLesson 2-Introduction To The ICD-10-CM ClassificationSwamyNo ratings yet
- 99names PDFDocument6 pages99names PDFYush GhNo ratings yet
- Chapter 6 NeoplasiaDocument24 pagesChapter 6 Neoplasiahenna patelNo ratings yet
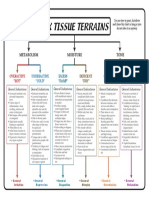
- 6 Tissue Terrains ColorDocument1 page6 Tissue Terrains Colorஆ.க.கோ. இராஜேஷ்வரக் கோன்No ratings yet