You might also like
- (备份)皇冠GRE新新高高频填空篇(2022版) pdf 20231025201907593Document167 pages(备份)皇冠GRE新新高高频填空篇(2022版) pdf 20231025201907593florexxi19No ratings yet
- Physical Therapy AssessmentDocument38 pagesPhysical Therapy Assessmentnikki98% (56)
- Strasinger, Susan King, Di Lorenzo, Marjorie Schaub - Urinalysis and Body Fluids 7th EdDocument426 pagesStrasinger, Susan King, Di Lorenzo, Marjorie Schaub - Urinalysis and Body Fluids 7th EdJocelle89% (9)
- Dr. Asif Mian Ansari DNB Resident Dept. of General Surgery Max Hospital, MohaliDocument25 pagesDr. Asif Mian Ansari DNB Resident Dept. of General Surgery Max Hospital, MohaliKarem Maali100% (1)
- Complete Mind FullDocument1,079 pagesComplete Mind FullhayasakaNo ratings yet
- 2022 Non-Cardiac SurgeryDocument105 pages2022 Non-Cardiac Surgeryhosameldin ahmedNo ratings yet
- Nail StructureDocument48 pagesNail StructureZyraMarie MartinNo ratings yet
- Treatment of Acute Ischemic StrokeDocument22 pagesTreatment of Acute Ischemic StrokeByron Coello ViñánNo ratings yet
- (19330693 - Journal of Neurosurgery) Decompressive Hemicraniectomy - Predictors of Functional Outcome in Patients With Ischemic StrokeDocument7 pages(19330693 - Journal of Neurosurgery) Decompressive Hemicraniectomy - Predictors of Functional Outcome in Patients With Ischemic StrokeRandy Reina RiveroNo ratings yet
- Can Transient BP High Risk Cerebral InfarctsDocument9 pagesCan Transient BP High Risk Cerebral InfarctsshofidhiaaaNo ratings yet
- Intensive Care Management of Subarachnoid HaemorrhDocument9 pagesIntensive Care Management of Subarachnoid HaemorrhTariku GelesheNo ratings yet
- Bismilah PPT Jurnal SAH MandaDocument26 pagesBismilah PPT Jurnal SAH MandaaristaNo ratings yet
- Summary 2014 Esc GuidelinesDocument13 pagesSummary 2014 Esc GuidelinesNick StamatiadisNo ratings yet
- Ultra-Early Tranexamic Acid After Subarachnoid Hemorrhage (ULTRA) : Study Protocol For A Randomized Controlled TrialDocument7 pagesUltra-Early Tranexamic Acid After Subarachnoid Hemorrhage (ULTRA) : Study Protocol For A Randomized Controlled Trialrikadwi20No ratings yet
- Olavarria2016 PDFDocument5 pagesOlavarria2016 PDFNurul AzmiyahNo ratings yet
- Acute MX of StrokeDocument23 pagesAcute MX of StrokeAshish GuragainNo ratings yet
- ESO Guideline TIADocument24 pagesESO Guideline TIASiti ZulaikhahNo ratings yet
- Prehospital Stroke Care: New Prospects For Treatment and Clinical ResearchDocument8 pagesPrehospital Stroke Care: New Prospects For Treatment and Clinical ResearchmiriamneuroNo ratings yet
- POINT TrialDocument27 pagesPOINT TrialRutaNo ratings yet
- Thirty-Day Readmission Is Higher in Patients With Brainstem vs. Non-Brainstem Lacunar StrokeDocument5 pagesThirty-Day Readmission Is Higher in Patients With Brainstem vs. Non-Brainstem Lacunar StrokeijasrjournalNo ratings yet
- Missed Ischemic Stroke Diagnosis in The Emergency Department by Emergency Medicine and Neurology ServicesDocument7 pagesMissed Ischemic Stroke Diagnosis in The Emergency Department by Emergency Medicine and Neurology ServicesReyhansyah RachmadhyanNo ratings yet
- Goyal Et Al-2015-Annals of NeurologyDocument7 pagesGoyal Et Al-2015-Annals of NeurologyWinda Wahyu IkaputriNo ratings yet
- Module 1 - Acute Ischemic StrokeDocument51 pagesModule 1 - Acute Ischemic StrokeRick RanitNo ratings yet
- TX Iskemik StrokeDocument17 pagesTX Iskemik StrokeNailis Sa'adahNo ratings yet
- GFHFGHFGHDocument3 pagesGFHFGHFGHAndrés JimaNo ratings yet
- Admission Inferior Vena Cava Measurements Are Associated With Mortality After Hospitalization For Acute Decompensated Heart FailureDocument18 pagesAdmission Inferior Vena Cava Measurements Are Associated With Mortality After Hospitalization For Acute Decompensated Heart FailurePuja Nastia LubisNo ratings yet
- Acute Ischemic Stroke Thrombolysis With Tenecteplase - An Institutional Experience From South India - PMCDocument8 pagesAcute Ischemic Stroke Thrombolysis With Tenecteplase - An Institutional Experience From South India - PMCviva dialysisNo ratings yet
- Ischemicstroke: Advances in Diagnosis and ManagementDocument20 pagesIschemicstroke: Advances in Diagnosis and ManagementPatty MArivel ReinosoNo ratings yet
- JHLT Abstract 2020-1Document1 pageJHLT Abstract 2020-1G WNo ratings yet
- Association Between Stress Hyperglycemia and OutcomesDocument9 pagesAssociation Between Stress Hyperglycemia and OutcomesResiden Neuro FK UNPAD - RSHSNo ratings yet
- Early Stroke Risk After Transient Ischemic Attack Among Individuals With Symptomatic Intracranial Artery StenosisDocument5 pagesEarly Stroke Risk After Transient Ischemic Attack Among Individuals With Symptomatic Intracranial Artery StenosisYunifianti ViviNo ratings yet
- Features of Branch Occlusive Disease-Type Intracranial Atherosclerotic Stroke in Young PatientsDocument7 pagesFeatures of Branch Occlusive Disease-Type Intracranial Atherosclerotic Stroke in Young PatientsrajaririnNo ratings yet
- Cambios en El EKG Predictores de Edema Pulmonar Neurogénico en Hemorragia SubaracnoideaDocument4 pagesCambios en El EKG Predictores de Edema Pulmonar Neurogénico en Hemorragia SubaracnoideaCristina Duran GarcíaNo ratings yet
- Tiempo e Intervalo de Reduccion HSADocument7 pagesTiempo e Intervalo de Reduccion HSAjosue leonardo RuizNo ratings yet
- DCV PDFDocument25 pagesDCV PDFLeyDi CamposanoNo ratings yet
- Acute Stroke Intervention: The Heart of The Matter: SciencedirectDocument2 pagesAcute Stroke Intervention: The Heart of The Matter: SciencedirectMarianaPlataNo ratings yet
- Los 10 Mandamientos Del Síndrome Coronario Agudo SEC 2023Document3 pagesLos 10 Mandamientos Del Síndrome Coronario Agudo SEC 2023Yaneth FernandezNo ratings yet
- Higher Prevalence of Diabetes in Pontine Infarction Than inDocument8 pagesHigher Prevalence of Diabetes in Pontine Infarction Than inMarshall ThompsonNo ratings yet
- 2023 Guideline Aneurysmal Subarachnoid HemorrhageDocument165 pages2023 Guideline Aneurysmal Subarachnoid Hemorrhagewmy6rf7nypNo ratings yet
- Anticoagulation Resumption After Intracerebral HemorrhageDocument10 pagesAnticoagulation Resumption After Intracerebral HemorrhagesenkonenNo ratings yet
- En Do Vascular Stenting or Carotid My For Treatment of Carotid Stenosis A Meta AnalysisDocument6 pagesEn Do Vascular Stenting or Carotid My For Treatment of Carotid Stenosis A Meta Analysisjohn_smith_532No ratings yet
- JCM 11 06258Document13 pagesJCM 11 06258deja234No ratings yet
- HSCRP (High-Sensitivity C - Reactive Protein) and Its Association With Short Term Prognosis Following Ischaemic StrokeDocument5 pagesHSCRP (High-Sensitivity C - Reactive Protein) and Its Association With Short Term Prognosis Following Ischaemic Strokeahc4allNo ratings yet
- QR Management of Ischaemic Stroke 3rd Edition 2020 v20210228Document25 pagesQR Management of Ischaemic Stroke 3rd Edition 2020 v20210228Jye yiNo ratings yet
- Antiandri, 5358-1 PDFDocument4 pagesAntiandri, 5358-1 PDFrifki irsyadNo ratings yet
- Echocardiography in Hemodynamic MonitoringDocument5 pagesEchocardiography in Hemodynamic MonitoringDr.Biswajit jenaNo ratings yet
- Annals of Neurology - 2021 - Polymeris - Oral Anticoagulants in The Oldest Old With Recent Stroke and Atrial FibrillationDocument11 pagesAnnals of Neurology - 2021 - Polymeris - Oral Anticoagulants in The Oldest Old With Recent Stroke and Atrial FibrillationJavier RamirezNo ratings yet
- Predictors and Outcomes of Shunt-Dependent Hydrocephalus in Patients With Aneurysmal Sub-Arachnoid HemorrhageDocument8 pagesPredictors and Outcomes of Shunt-Dependent Hydrocephalus in Patients With Aneurysmal Sub-Arachnoid HemorrhageNovia AyuNo ratings yet
- Sinkovi 2018Document8 pagesSinkovi 2018EviNo ratings yet
- Nurses Application FormDocument7 pagesNurses Application FormVillanueva Ameera MaeNo ratings yet
- Case Meta AnalysisDocument10 pagesCase Meta AnalysisTutik RahayuNo ratings yet
- Endovascular Therapy Neuro Intervention (MT) in AIS DR GaneshDocument34 pagesEndovascular Therapy Neuro Intervention (MT) in AIS DR GaneshDr Ganeshgouda MajigoudraNo ratings yet
- Massive Hemorrhage ProtocolDocument19 pagesMassive Hemorrhage ProtocolJefferson Duque MartinezNo ratings yet
- Guidelines & Protocols: Stroke and Transient Ischemic Attack - Management and Prevention Advisory CommitteeDocument13 pagesGuidelines & Protocols: Stroke and Transient Ischemic Attack - Management and Prevention Advisory CommitteeAndi SaputraNo ratings yet
- Timing of Aneurysm Treatment After Subarachnoid HemorrhageDocument5 pagesTiming of Aneurysm Treatment After Subarachnoid HemorrhageJulieta PereyraNo ratings yet
- Prognosis ExampleDocument13 pagesPrognosis ExamplenathanielNo ratings yet
- Ijmsv 14 P 1241Document10 pagesIjmsv 14 P 1241Milan PetrikNo ratings yet
- Clinical Characteristics of Fast and Slow Progressors of Infarct Growth in Anterior Circulation Large Vessel Occlusion StrokeDocument6 pagesClinical Characteristics of Fast and Slow Progressors of Infarct Growth in Anterior Circulation Large Vessel Occlusion StrokeItamar MeirelesNo ratings yet
- Flat-Head Positioning Increases Cerebral Blood Flow in Anterior Circulation Acute Ischemic Stroke. A Cluster Randomized Phase Iib TrialDocument12 pagesFlat-Head Positioning Increases Cerebral Blood Flow in Anterior Circulation Acute Ischemic Stroke. A Cluster Randomized Phase Iib TrialSelvi PurnamasariNo ratings yet
- Stroke PreventionDocument8 pagesStroke PreventionjaanhoneyNo ratings yet
- The Role of Imaging in Acute Ischemic Stroke: E T, M.D., Q H, M.D., P .D., J B. F, M.D., M W, M.D., M.a.SDocument17 pagesThe Role of Imaging in Acute Ischemic Stroke: E T, M.D., Q H, M.D., P .D., J B. F, M.D., M W, M.D., M.a.Schrist_cruzerNo ratings yet
- Komplikasi Stroke PDFDocument7 pagesKomplikasi Stroke PDFJose Hady PuteraNo ratings yet
- Clinical Risk Factors of Asymptomatic Deep VenousDocument7 pagesClinical Risk Factors of Asymptomatic Deep VenoussenkonenNo ratings yet
- Flat-Head Positioning Increases Cerebral Blood Flow in Anterior Circulation Acute Ischemic Stroke. A Cluster Randomized Phase Iib TrialDocument12 pagesFlat-Head Positioning Increases Cerebral Blood Flow in Anterior Circulation Acute Ischemic Stroke. A Cluster Randomized Phase Iib TrialNaufal HilmiNo ratings yet
- CHANCE Trial: Early Short-Term Dual Antiplatelet Treatment For Stroke PreventionDocument3 pagesCHANCE Trial: Early Short-Term Dual Antiplatelet Treatment For Stroke PreventionNada AhmedNo ratings yet
- Cardiac Sarcoidosis: Key Concepts in Pathogenesis, Disease Management, and Interesting CasesFrom EverandCardiac Sarcoidosis: Key Concepts in Pathogenesis, Disease Management, and Interesting CasesNo ratings yet
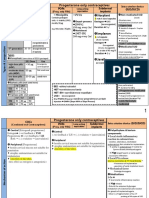
- Norplant: Progesterone Only ContraceptivesDocument9 pagesNorplant: Progesterone Only ContraceptivesFathy ElsheshtawyNo ratings yet
- CCCXXDGBN Lab Result 2022 07 22 11 - 41 - 26Document1 pageCCCXXDGBN Lab Result 2022 07 22 11 - 41 - 26bkimberlymarNo ratings yet
- OET Test 1 PA by DrNesma RabieDocument5 pagesOET Test 1 PA by DrNesma RabieRancesh FamoNo ratings yet
- Effectively Planning For and Managing Major Disasters: John C. CavanaughDocument21 pagesEffectively Planning For and Managing Major Disasters: John C. CavanaughMichael AquinoNo ratings yet
- Advances and Challenges in Stroke RehabilitationDocument13 pagesAdvances and Challenges in Stroke Rehabilitationarif 2006No ratings yet
- English For Presentation CDocument11 pagesEnglish For Presentation CeviNo ratings yet
- Safety Data Sheet: Texclad 2Document7 pagesSafety Data Sheet: Texclad 2Om Prakash RajNo ratings yet
- ENG 111 - RHETORICAL ANALYSIS - OvercomerDocument7 pagesENG 111 - RHETORICAL ANALYSIS - OvercomerZareen SubahNo ratings yet
- 1548 6066 1 PBDocument10 pages1548 6066 1 PBOun VikrethNo ratings yet
- Emirates Aluminium Smelter Complex QA PlanDocument32 pagesEmirates Aluminium Smelter Complex QA PlanSagar AliasjackeyNo ratings yet
- San Carlos College: Detailed Lesson Plan in Physical Education IvDocument9 pagesSan Carlos College: Detailed Lesson Plan in Physical Education IvJolina MatabangNo ratings yet
- Health Declaration Form A1 Whole PageDocument1 pageHealth Declaration Form A1 Whole PageFedelyn SemenianoNo ratings yet
- IARCDocument868 pagesIARCmarcosiqNo ratings yet
- Prep 4 Post LabDocument2 pagesPrep 4 Post LabKate MendozaNo ratings yet
- New Principles in Pilon Fractres ManagementDocument17 pagesNew Principles in Pilon Fractres ManagementCamila FontechaNo ratings yet
- Traditional BSN Degree Plan 2022 2023 202220Document1 pageTraditional BSN Degree Plan 2022 2023 202220Edgar MartínezNo ratings yet
- Palm Beach County Student Academic Support PlanDocument29 pagesPalm Beach County Student Academic Support PlanMatt PapaycikNo ratings yet
- Practical Research 2Document7 pagesPractical Research 2Jesa mae TorinoNo ratings yet
- Overview of The Automated Coagulation AnalyzerDocument10 pagesOverview of The Automated Coagulation AnalyzerNoah ZlinNo ratings yet
- PHYSICIANS Room Assignment 03-2021Document13 pagesPHYSICIANS Room Assignment 03-2021PRC BaguioNo ratings yet
- Bioethics and ResearchDocument4 pagesBioethics and ResearchHan CallejaNo ratings yet
- Push Jerk - CrossFit Training GuideDocument6 pagesPush Jerk - CrossFit Training GuideDominik KadlecNo ratings yet
- Holistic Approach To Mental HealthDocument38 pagesHolistic Approach To Mental HealthabhishekNo ratings yet
- ICD 10 Codes For Dental Practice: L PracticesDocument9 pagesICD 10 Codes For Dental Practice: L PracticesAji HerlambangNo ratings yet