You might also like
- Aki 4Document11 pagesAki 4WindaNo ratings yet
- Aki To CKDDocument22 pagesAki To CKDSrinivas PingaliNo ratings yet
- The Japanese Clinical Practice Guideline For Acute Kidney Injury 2016Document55 pagesThe Japanese Clinical Practice Guideline For Acute Kidney Injury 2016RobertNo ratings yet
- Nihms 300455Document22 pagesNihms 300455Maria Eduarda CardosoNo ratings yet
- Personalized Acute Kidney Injury TreatmentDocument8 pagesPersonalized Acute Kidney Injury TreatmentGabriela PachecoNo ratings yet
- AKI PathogenesisDocument11 pagesAKI PathogenesisKaren RamNo ratings yet
- Acute Kidney Injury Narrative 2021Document16 pagesAcute Kidney Injury Narrative 2021Sanjith SaseedharanNo ratings yet
- Article AcuteKidneyInjuryInTheCriticalDocument16 pagesArticle AcuteKidneyInjuryInTheCriticalJoão João MendesNo ratings yet
- Diagnosis and Treatment of Acute Kidney Injury in PediatricsDocument13 pagesDiagnosis and Treatment of Acute Kidney Injury in PediatricsagungNo ratings yet
- News & Views: Acute Kidney Injury: Still Misunderstood and MisdiagnosedDocument3 pagesNews & Views: Acute Kidney Injury: Still Misunderstood and MisdiagnosedRobertNo ratings yet
- Ostermann 2020 Cs 200002 1604501146.08266Document17 pagesOstermann 2020 Cs 200002 1604501146.08266Marco RahardjaNo ratings yet
- Sepsis-Associated Acute Kidney Injury: Consensus Report of The 28th Acute Disease Quality Initiative WorkgroupDocument17 pagesSepsis-Associated Acute Kidney Injury: Consensus Report of The 28th Acute Disease Quality Initiative WorkgroupDaniel AmezcuaNo ratings yet
- AKI Perioperatif 2Document12 pagesAKI Perioperatif 2Kevin JohanesNo ratings yet
- Periop AKIDocument12 pagesPeriop AKINavjot KaurNo ratings yet
- Acute Kidney Injury 2019Document16 pagesAcute Kidney Injury 2019ShadowK 99No ratings yet
- Markers of Acute Kidney InjuryDocument7 pagesMarkers of Acute Kidney InjuryPrasanna KhuntiNo ratings yet
- Acute Kidney Injury Lancet RoncoDocument16 pagesAcute Kidney Injury Lancet RoncoRogelio MarchanNo ratings yet
- Anemia and AkiDocument10 pagesAnemia and AkiIkaDian PuspitanzaNo ratings yet
- 1 s2.0 S0085253821006621 MainDocument11 pages1 s2.0 S0085253821006621 MainAllison Eunice ServandoNo ratings yet
- The KDIGO AKI Guidelines: From 2011-2019Document38 pagesThe KDIGO AKI Guidelines: From 2011-2019Andreas Agung KurniawanNo ratings yet
- Low-Flow Acute Kidney InjuryDocument11 pagesLow-Flow Acute Kidney InjuryJuan Manuel Lopez VargasNo ratings yet
- Intensive Care Unit-Acquired Weakness in Patients With Acute Kidney Injury A Contemporary ReviewDocument16 pagesIntensive Care Unit-Acquired Weakness in Patients With Acute Kidney Injury A Contemporary ReviewMajooCalderonNo ratings yet
- Management of Acute Kidney Injury - Core Curriculum 2018Document13 pagesManagement of Acute Kidney Injury - Core Curriculum 2018Enrique Aguilar MNo ratings yet
- AkiDocument20 pagesAkiEnvhy AmaliaNo ratings yet
- Acute Kidney InjuryDocument16 pagesAcute Kidney InjuryAdo QuirozNo ratings yet
- Acute Kidney Injury: Current Concepts and New Insights: Key WordsDocument5 pagesAcute Kidney Injury: Current Concepts and New Insights: Key WordsIHNo ratings yet
- Management of Acute Kidney Injury: Core Curriculum 2018Document13 pagesManagement of Acute Kidney Injury: Core Curriculum 2018Kholida NabilaNo ratings yet
- Biomarcadores Post Aki A ErcDocument12 pagesBiomarcadores Post Aki A ErcGiss UrizarNo ratings yet
- Subphenotypes of Acute Kidney Injury 2022Document6 pagesSubphenotypes of Acute Kidney Injury 2022Juan Diego JImenez AlvizoNo ratings yet
- Paper 2Document15 pagesPaper 2constanzanazarethNo ratings yet
- Section 1. Definition and Classification of Acute Kidney InjuryDocument18 pagesSection 1. Definition and Classification of Acute Kidney InjuryPremaKurniaNo ratings yet
- Acute Kidney Injury - Seminar Lancet 2019Document16 pagesAcute Kidney Injury - Seminar Lancet 2019Giliana P. García AcevedoNo ratings yet
- AKI - Acute Kidney Injury Classification RIFLE and AKIN CriteriaDocument6 pagesAKI - Acute Kidney Injury Classification RIFLE and AKIN CriteriaIntan Siti HulaimaNo ratings yet
- Acute Kidney Injury - Diagnosis and Management 2019Document8 pagesAcute Kidney Injury - Diagnosis and Management 2019srikandiNo ratings yet
- Sfaa 142Document11 pagesSfaa 142Eduardo AdameNo ratings yet
- Definiendio Enfermedad Renal Aguda 2021 NephronDocument4 pagesDefiniendio Enfermedad Renal Aguda 2021 NephronGabino Alexander Liviac CrisostomoNo ratings yet
- Molen2018 Article Post-contrastAcuteKidneyInjury PDFDocument11 pagesMolen2018 Article Post-contrastAcuteKidneyInjury PDFEliza CrăciunNo ratings yet
- Study of Etiology, Clinical Profile and Outcome of Acute Kidney (AKI) in Medical Intensive Care UnitDocument4 pagesStudy of Etiology, Clinical Profile and Outcome of Acute Kidney (AKI) in Medical Intensive Care UnitDavid Al HavizNo ratings yet
- Overview of Diagnostic Criteria and Epidemiology of Acute Kidney Injury and Acute Kidney Disease in The Critically Ill PatientDocument19 pagesOverview of Diagnostic Criteria and Epidemiology of Acute Kidney Injury and Acute Kidney Disease in The Critically Ill PatientPaulo PimentelNo ratings yet
- Epidemio AkiDocument10 pagesEpidemio AkiSoniamartilovaNo ratings yet
- Jurnal Aki 2018Document13 pagesJurnal Aki 2018Arief TricahyonoNo ratings yet
- The RIFLE and AKIN Classifications For Acute Kidney Injury: A Critical and Comprehensive ReviewDocument7 pagesThe RIFLE and AKIN Classifications For Acute Kidney Injury: A Critical and Comprehensive ReviewLivia Meidy UbayidNo ratings yet
- In-Depth Review: Joseph L. Alge and John M. ArthurDocument9 pagesIn-Depth Review: Joseph L. Alge and John M. ArthurKiran AsrannaNo ratings yet
- An Update of Long-Noncoding Rnas in Acute Kidney Injury: Lina Yang, Bo Wang, Liang Ma and Ping FuDocument12 pagesAn Update of Long-Noncoding Rnas in Acute Kidney Injury: Lina Yang, Bo Wang, Liang Ma and Ping FuFrank Antony Arizabal GaldosNo ratings yet
- WWW - Uwonephrology.ca Pdfs Academichalfday 20110308 AKIPart12011Document8 pagesWWW - Uwonephrology.ca Pdfs Academichalfday 20110308 AKIPart12011Ale Marques - TarólogoNo ratings yet
- 2020 Article 390Document2 pages2020 Article 390Riswanto RuslanNo ratings yet
- Evidence-Based Nephrology: Rakesh Malhotra and Edward D. SiewDocument25 pagesEvidence-Based Nephrology: Rakesh Malhotra and Edward D. SiewnudhakoNo ratings yet
- 2021 - Outcome of Acute Kidney Injury - How To Make A DiferenceDocument11 pages2021 - Outcome of Acute Kidney Injury - How To Make A Diference5rjpyc2mgfNo ratings yet
- Somekerki 2024Document10 pagesSomekerki 2024Emiliano GarcilazoNo ratings yet
- Kdoki y KdigoDocument24 pagesKdoki y KdigoIsrael Armida SodanargNo ratings yet
- The Potential Use of Biomarkers in Predicting Contrast-Induced Acute Kidney InjuryDocument17 pagesThe Potential Use of Biomarkers in Predicting Contrast-Induced Acute Kidney Injuryumie khoirunNo ratings yet
- Global Epidemiology and Outcomes of Acute Kidney InjuryDocument19 pagesGlobal Epidemiology and Outcomes of Acute Kidney Injuryredouane bennaiNo ratings yet
- Indicaciones AkiDocument8 pagesIndicaciones Akijair giancarlo villanueva arteagaNo ratings yet
- Urine NGAL Predicts Severity of Acute Kidney Injury After Cardiac Surgery: A Prospective StudyDocument9 pagesUrine NGAL Predicts Severity of Acute Kidney Injury After Cardiac Surgery: A Prospective StudyCa Nd RaNo ratings yet
- 154-The Frequency and Aetiology of Repeated Kidney Injury Episodes Determine The Degree of Renal DamageDocument2 pages154-The Frequency and Aetiology of Repeated Kidney Injury Episodes Determine The Degree of Renal DamageCarlos Martinez SalgadoNo ratings yet
- Potential Interventions in Sepsis-Related Acute Kidney InjuryDocument14 pagesPotential Interventions in Sepsis-Related Acute Kidney InjurynudhakoNo ratings yet
- The Definition of Acute Kidney Injury and Its Use in PracticeDocument12 pagesThe Definition of Acute Kidney Injury and Its Use in PracticeErwin SiahaanNo ratings yet
- Recent Advances of Sarcopenia and Frailty in CKDFrom EverandRecent Advances of Sarcopenia and Frailty in CKDAkihiko KatoNo ratings yet
- Anschutz: City of HealthDocument42 pagesAnschutz: City of HealthMark HardenNo ratings yet
- PKC AryanDocument62 pagesPKC AryanAryan PurohitNo ratings yet
- NCM 112 - Renal DisordersDocument4 pagesNCM 112 - Renal DisordersCailah Sofia SelausoNo ratings yet
- Hurst 11 - RenalDocument6 pagesHurst 11 - RenalPascal St Peter NwaorguNo ratings yet
- Monitoring Hipertensi Andi NasirDocument6 pagesMonitoring Hipertensi Andi NasirBabay JamNo ratings yet
- 713 FullfDocument11 pages713 FullfMario HBNo ratings yet
- Glomerulopathy: Acute Nephritic SyndromeDocument109 pagesGlomerulopathy: Acute Nephritic SyndromekamalNo ratings yet
- KHC Education Session English PowerpointDocument65 pagesKHC Education Session English PowerpointkugernnesNo ratings yet
- Nbns2203 Renal and Endocrine NursingDocument10 pagesNbns2203 Renal and Endocrine Nursingdicky chongNo ratings yet
- Acute Glomerulonephritis (AGN)Document5 pagesAcute Glomerulonephritis (AGN)smashayielNo ratings yet
- 1 Childhood Nephrotic Syndrome - Diagnosis and ManagementDocument52 pages1 Childhood Nephrotic Syndrome - Diagnosis and ManagementThana Balan100% (1)
- Google XRay LinkedIn 2020 748893069Document12 pagesGoogle XRay LinkedIn 2020 748893069vinaykaambleNo ratings yet
- Chronic Kidney Disease in Adults - Assessment and ManagementDocument5 pagesChronic Kidney Disease in Adults - Assessment and ManagementAnahí Cortés HerreraNo ratings yet
- Sindrome Nefrotico - Etiology, Clinical Manifestations, and Diagnosis of Nephrotic Syndrome in ChildrenDocument13 pagesSindrome Nefrotico - Etiology, Clinical Manifestations, and Diagnosis of Nephrotic Syndrome in ChildrenAiled HerediaNo ratings yet
- Pediatric Iga Nephropathy in Europe: Review ArticleDocument7 pagesPediatric Iga Nephropathy in Europe: Review ArticleAmabelle PanganibanNo ratings yet
- Full Download Ebook Ebook PDF Nelson Essentials of Pediatrics 8th Edition PDFDocument41 pagesFull Download Ebook Ebook PDF Nelson Essentials of Pediatrics 8th Edition PDFdavid.anderson198100% (42)
- Hubungan Antara NLR Dan Aki Pada Pasien SepsisDocument4 pagesHubungan Antara NLR Dan Aki Pada Pasien Sepsisdwi widyaNo ratings yet
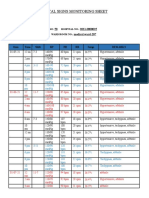
- Vital Signs Monitoring SheetDocument2 pagesVital Signs Monitoring SheetRenea Joy ArruejoNo ratings yet
- Case Report模板Document18 pagesCase Report模板ChenNo ratings yet
- Nurses Chart SampleDocument18 pagesNurses Chart SampleJake Marcelo Tabua100% (4)
- NephSAP HTNDocument88 pagesNephSAP HTNAditya JayaramanNo ratings yet
- Dr. Shekhawat (Assignment)Document18 pagesDr. Shekhawat (Assignment)Myrna ChristyNo ratings yet
- Clinico-Microbiological Spectrum of Hemodialysis Catheter-Related Blood Stream Infections: A Concise ReviewDocument7 pagesClinico-Microbiological Spectrum of Hemodialysis Catheter-Related Blood Stream Infections: A Concise ReviewIJAR JOURNALNo ratings yet
- Hospital List District Wise-FinalDocument13 pagesHospital List District Wise-FinalArkiNo ratings yet
- Congenital Anomalies of KidneDocument7 pagesCongenital Anomalies of KidneSanthosh.S.U100% (2)
- Thiazide and Thiazide-Like DiureticsDocument3 pagesThiazide and Thiazide-Like DiureticsYohanes SutrisnoNo ratings yet
- Chapter 48Document15 pagesChapter 482071317No ratings yet
- Chronic Renal Failure: Lecture Speaker Dr. V. Lakshmi Prasanna MariseDocument23 pagesChronic Renal Failure: Lecture Speaker Dr. V. Lakshmi Prasanna MariseManjunath ArunachalamNo ratings yet
- GlomerulonephritisDocument1 pageGlomerulonephritismaleskunNo ratings yet
- New Latest List of Delhi Updated June 2020Document88 pagesNew Latest List of Delhi Updated June 2020Ashish Singh NegiNo ratings yet