MANAGEMENT OF ACUTE KIDNEY INJURY
PREVENTION OF AKI
Identify those at risk
• Many patients are already developing AKI on admission and many others during admission.
• To prevent AKI and recognize AKI early, consider these risk factors on admission and on every review:
• General: age >65, known CKD, previous AKI
• Acute events: sepsis, falls with long lie, dehydration (vomiting, diarrhoea, high fever, ileostomy),
haemorrhage, shock, major surgery, overnight or repeated fasting
• Comorbidities: diabetes, vascular disease, heart disease, liver disease, malignancy
• Drugs/toxins: ACEI/ARBs, NSAIDs, diuretics, aminoglucosides, contrast
Monitor those at risk
• Assess volume status daily with clinical monitoring
• Fluid balance chart and weight daily
• U+Es every 1-2 days
Protect those at risk
• Individualize volume status targets. Avoid dehydration/hypovolaemia by NG and/or IV fluid supplementation.
• 500ml 0.9% saline over 6-8 hrs before and after contrast exposure
• Review drugs: adjust doses, stop nephrotoxins, once daily renal dose aminoglycosides if unavoidable •
Early treatment for sepsis
MOHW August 2020
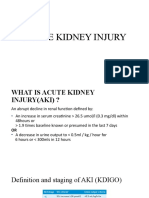
What is AKI ?
• AKI is a sudden decline in kidney function over hours or days
• Most often seen during episodes of acute illness
• Can occur on top of chronic kidney disease
• It is diagnosed by either a rise in serum creatinine or a fall in urine output (see table below)
KDIGO AKI Staging
Stage Serum creatinine Urine Output
1 1.5 to 1.9 x baseline OR increase by ≥ 26 μmol/L within 48hrs <0.5 mL/kg/hr for > 6 consecutive
hrs
2 2 to 2.9 x baseline <0.5 mL/kg/ hr for > 12 hrs
3 ≥3 X baseline OR increase to ≥ 354 μmol/L <0.3 mL/kg/ hr for > 24 hrs
OR initiation on renal replacement therapy OR anuria for 12 hrs
WHY IS AKI IMPORTANT?
AKI occurs in 10-20% of emergency hospital admissions
Increased length of hospital stay and morbidity
>20% of these will die during hospital admission, usually due to cardiovascular events,sepsis or upper GI bleed
AKI can progress to CKD later in life (may lead to needing long term dialysis)
AKI can accelerate progression of pre-existing CKD (may lead to needing long term dialysis)
Pre-renal AKI is rapidly reversible if treated early. If not, it l0eads to a more serious acute tubular injury
SEEK EXPERT HELP
Refer to nephrology team if:
●
There is no clear cause of AKI
●
New finding of blood and/or protein on urine dipstick (in absence of UTI, regardless of stage) ●
Systemic symptoms e.g. vasculitic rash, epistaxis, haemoptysis, polyarthralgia
●
Patient has a kidney transplant
●
Inadequate response to initial treatment
●
AKI Stage 3 or serum creatinine >300umol/l
●
Dialysis is indicated: Life-threatening or intractable pulmonary oedema
Uncontrollably rising K+
Severe (pH < 7.2) or worsening acidosis
Refer to urology if obstruction suspected. Refer to ICU if patient critically ill .
MANAGEMENT OF AKI
Fluid management. Assess fluid status. Correct hypovolaemia using 0.9% saline with continuous monitoring of
pulse, BP, JVP, chest auscultation and urine output. If urine output remains low after 2 litres of fluid seek Sp
advice. Once patient is adequately volume resuscitated maintain fluid intake at a rate of urine output + 30 ml/hr.
Use diuretics ONLY if volume overload is present.
Optimise blood pressure. If patient remains hypotensive (SBP<100 mm Hg) after fluid therapy consider
inotropic agent (not renal dose dopamine) and ICU advice. CVP monitoring is useful only in ICU.
Check for palpable bladder. Urethral catheterisation NOT mandatory. Only indicated if patient immobile,
obstructed, uncooperative or critically ill.
Treat sepsis with appropriate antibiotics. Put on PPI as stress ulcers likely.
Treat hyperglycaemia with sliding scale insulin but stop metformin, sulphonylureas, SGLT2I
Stop all nephrotoxins: ACEI, ARB, NSAIDs, aminoglycosides
Adjust drug doses to allow for reduced renal clearance (eg opiates, vancomycin)
Watch out for complications: fluid overload (see protocol), hyperkalaemia ( see protocol), metabolic acidosis,
hypoglycaemia not rare in AKI patients (IV dextrose infusion)
Baseline Investigations
Urine: dipstick, microscopy, ACR, culture and sensitivity
Blood: U+Es, LFTs, calcium, uric acid, Fbc with differential. ABG if clinically indicated
Imaging: USS of kidneys and urinary tract
FIND THE CAUSE oF AKI
Most causes will be obvious from history, examination and the above investigations. If not consider the following:
PRE-RENAL INTRINSIC
Decreased effective Acute tubular injury
Circulating volume Ischaemic (from prolonged or severe pre-renal AKI)
Haemorrhage Toxins
Volume depletion - Nephrotoxic drugs
Sepsis Full culture screen, CRP - Radiocontrasts
Cardio-renal syndromes
Troponin, cardiac imaging - Haemoglobinuria Full haemolysis screen
Liver failure - Myoglobinuria CK, urinary myoglobin
- Intratubular crystal
Arterial narrowing - Myeloma casts BJP, serum protein electrophoresis,
free light chains, kidney biopsy
Vasomotor
NSAIDs
Glomerulonephritis/ANCA, ANA, Anti-GBM, Anti dsDNA,
ACEI/ARBs
Vasculitis C3/C4, ENA
, Immunoglobulins, cryoglobulins,
hep B,C HIV serology, kidney biopsy
Interstitial nephritiseosinophilia,eosinophiluria, kidney biopsy
POST-RENAL CT imaging, cystoscopy
Bladder Outlet obstruction Vascular
Bilateral ureteric obstruction HUS/TTP Full haemolysis screen
Ureteric obstruction of single kidney Accelerated hypertension
You might also like
- Noel A. Villanueva, MD, FPCP, FPSNDocument62 pagesNoel A. Villanueva, MD, FPCP, FPSNagilNo ratings yet
- Acute Kidney InjuryDocument40 pagesAcute Kidney InjuryNabin SimkhadaNo ratings yet
- L11 Renal Failure General Approach 230213 002819Document16 pagesL11 Renal Failure General Approach 230213 002819S sNo ratings yet
- 1tatalaksana Mal-berat-KalbarDocument29 pages1tatalaksana Mal-berat-Kalbarcindy christiantiNo ratings yet
- Renal Faliure 1Document50 pagesRenal Faliure 1180045No ratings yet
- Pedoman Tatalaksana Sindrom Koroner Akut 2015Document29 pagesPedoman Tatalaksana Sindrom Koroner Akut 2015Vittorio bagscenterNo ratings yet
- Acute Kidney Injury: Dana BabaDocument31 pagesAcute Kidney Injury: Dana Babanaheel98shNo ratings yet
- Acute Kidney Injury:: A Brief OutlineDocument48 pagesAcute Kidney Injury:: A Brief OutlinehanaNo ratings yet
- Aki NotesDocument10 pagesAki NotesGennel Mae GarovilloNo ratings yet
- 12a. Kuliah Aki 2017Document36 pages12a. Kuliah Aki 2017yussikafernandaNo ratings yet
- Acute Kidney Injury Diagnosis and Management ApproachDocument45 pagesAcute Kidney Injury Diagnosis and Management ApproachAndika Yusuf RamadhanNo ratings yet
- Lecture 2. Acute Renal FailureDocument85 pagesLecture 2. Acute Renal FailurePharmswipe KenyaNo ratings yet
- Acute Kidney Injury: Syakib BakriDocument46 pagesAcute Kidney Injury: Syakib BakriBhisma D. SyaputraNo ratings yet
- MRCP 2 Nephrology NOTESDocument74 pagesMRCP 2 Nephrology NOTESMuhammad HaneefNo ratings yet
- Integrated Therapeutics IiDocument165 pagesIntegrated Therapeutics IiSalahadinNo ratings yet
- Acute Kidney Injury OsamaDocument23 pagesAcute Kidney Injury Osamaosamafoud7710No ratings yet
- Aki - CKDDocument51 pagesAki - CKDAyu Luh Ratri WeningNo ratings yet
- Modul 7 Kegawatan Ginjal AnakDocument24 pagesModul 7 Kegawatan Ginjal AnakSanti IskandarNo ratings yet
- Acute Kidney Injury - Chronic Kidney DeseaseDocument71 pagesAcute Kidney Injury - Chronic Kidney DeseaseFina Ahmad Fitriana100% (1)
- Renal EmergenciesDocument93 pagesRenal EmergenciesShubham gaurNo ratings yet
- Acute Kidney Injury and Chronic Kidney DiseaseDocument44 pagesAcute Kidney Injury and Chronic Kidney DiseaseIda Bagus Putu Swabawa100% (1)
- Gagal GinjalDocument75 pagesGagal GinjalAndi HeriantoNo ratings yet
- Acute Kidney InjuryDocument3 pagesAcute Kidney InjuryHarkirat AtwalNo ratings yet
- Acute Kidney Injury: in The ClinicDocument29 pagesAcute Kidney Injury: in The ClinicAnitha SNo ratings yet
- Renal DisordersDocument164 pagesRenal Disorderspblinder1319No ratings yet
- Nephrology & Urology: Archer Online USMLE ReviewsDocument107 pagesNephrology & Urology: Archer Online USMLE ReviewsBeerappaJanpetNo ratings yet
- Acute Kidney Injury (AKI) : by Prof Grace Irimu Consultant Pediatrician and NephrologistDocument43 pagesAcute Kidney Injury (AKI) : by Prof Grace Irimu Consultant Pediatrician and Nephrologistokwadha simionNo ratings yet
- Acute Kidney Injury AKIDocument6 pagesAcute Kidney Injury AKIfazeel shah vlogsNo ratings yet
- Acute Renal FailureDocument33 pagesAcute Renal FailureAqsa Akbar AliNo ratings yet
- Acute Kidney Injury and Chronic Kidney DiseaseDocument44 pagesAcute Kidney Injury and Chronic Kidney DiseaseshihochanNo ratings yet
- Acute Renal FailureDocument5 pagesAcute Renal FailureSalman KhanNo ratings yet
- Acute Kidney Injury: Causes and DiagnosisDocument37 pagesAcute Kidney Injury: Causes and DiagnosisEndah Risky GustiyantiNo ratings yet
- Akd & CKDDocument44 pagesAkd & CKDﻣﻠﻚ عيسىNo ratings yet
- Tutorial Liver FailureDocument59 pagesTutorial Liver FailureNadhrah zulkifliNo ratings yet
- 1 Acute Renal FailureDocument65 pages1 Acute Renal FailureDammaqsaa W BiyyanaaNo ratings yet
- Kidney Emergency: M. Syamsul BakhriDocument30 pagesKidney Emergency: M. Syamsul BakhrierahadeNo ratings yet
- AKI and CKDDocument73 pagesAKI and CKDzaw wai aungNo ratings yet
- Acute Renal Failure in The ICU PulmCritDocument27 pagesAcute Renal Failure in The ICU PulmCritchadchimaNo ratings yet
- Acute Kidney Injury: Causes, Stages, and ManagementDocument62 pagesAcute Kidney Injury: Causes, Stages, and ManagementApidha KartinasariNo ratings yet
- Lecture - Acute Renal FailureDocument57 pagesLecture - Acute Renal FailureJames StiltonNo ratings yet
- Approach To Acute Kidney InjuryDocument44 pagesApproach To Acute Kidney InjuryKue GosongNo ratings yet
- AkiDocument42 pagesAkimarauder_popNo ratings yet
- Aki Miu BCPS 2015Document52 pagesAki Miu BCPS 2015SaraHussienNo ratings yet
- Management of Acute Kidney InjuryDocument31 pagesManagement of Acute Kidney InjurysumitNo ratings yet
- Dr.P.Sankaranarayanan MD: Emeritus Professor of Medicine Acs Medical College & HospitalDocument81 pagesDr.P.Sankaranarayanan MD: Emeritus Professor of Medicine Acs Medical College & HospitalvaishnaviNo ratings yet
- Acrf CDocument70 pagesAcrf CHussain AzharNo ratings yet
- AkiDocument38 pagesAkiPhillip MartinezNo ratings yet
- Baldwin Tub Ulo InterstitialDocument36 pagesBaldwin Tub Ulo InterstitialdrryanalwynNo ratings yet
- 6 To 12 Hours. For 12 Hours For 24 HoursDocument3 pages6 To 12 Hours. For 12 Hours For 24 HoursMohamad AbdelkhalikNo ratings yet
- Acute Kidney InjuryDocument21 pagesAcute Kidney InjuryyinyangdongNo ratings yet
- Acute Kidney Injury: DR B Parag Department of NephrologyDocument34 pagesAcute Kidney Injury: DR B Parag Department of NephrologybgfhnfgNo ratings yet
- Acute Renal FailureDocument50 pagesAcute Renal FailureEster Libunao DollagaNo ratings yet
- Material For Cme - AKIDocument20 pagesMaterial For Cme - AKIHzm AzizulNo ratings yet
- 00 NephrologyDocument98 pages00 Nephrologyeryxsp0% (1)
- Renal Emergency RevisiDocument103 pagesRenal Emergency Revisidesy f sarahNo ratings yet
- Materi 7 - Gagal Ginjal AkutDocument30 pagesMateri 7 - Gagal Ginjal AkutTegar Muhamad RifkiNo ratings yet
- Liver Cirrhosis: Etiology Pathogenesis Clinical Features Management PrognosisDocument35 pagesLiver Cirrhosis: Etiology Pathogenesis Clinical Features Management PrognosisMohd Johari Mohd ShafuwanNo ratings yet
- Acute Renal Failure Lecture 1 Critical Care NursingDocument52 pagesAcute Renal Failure Lecture 1 Critical Care NursingDina Rasmita100% (2)
- Pediatrics history taking PDF 2Document2 pagesPediatrics history taking PDF 2Red DevilNo ratings yet
- Pediatrics History Taking PDF 4Document2 pagesPediatrics History Taking PDF 4Red DevilNo ratings yet
- Pediatrics History Taking PDF 4Document2 pagesPediatrics History Taking PDF 4Red DevilNo ratings yet
- Hypertensive emergenciesDocument28 pagesHypertensive emergenciesRed DevilNo ratings yet
- Pediatrics history taking PDF 2Document2 pagesPediatrics history taking PDF 2Red DevilNo ratings yet
- 15.guidelines COPDDocument5 pages15.guidelines COPDRed DevilNo ratings yet
- Assessment and Management of The Unconscious PatientDocument6 pagesAssessment and Management of The Unconscious PatientRed DevilNo ratings yet
- Approach To Patient With Diarrhea and VomitingDocument4 pagesApproach To Patient With Diarrhea and VomitingRed DevilNo ratings yet
- 21 UtiDocument2 pages21 UtiRed DevilNo ratings yet
- Swingler (2013)Document4 pagesSwingler (2013)KayleighNo ratings yet
- Upper GIT BleedDocument4 pagesUpper GIT BleedRed DevilNo ratings yet
- 12.alcohol Withdrawal EffectsDocument2 pages12.alcohol Withdrawal EffectsRed DevilNo ratings yet
- Short Version of Draft Guideline 3Document14 pagesShort Version of Draft Guideline 3Red DevilNo ratings yet
- HEAD INJURY Presentation HDDocument29 pagesHEAD INJURY Presentation HDRed DevilNo ratings yet
- Traumatic Brain InjuryDocument40 pagesTraumatic Brain InjuryRed DevilNo ratings yet
- 01 VaccinationDocument1 page01 VaccinationRed DevilNo ratings yet
- Neuro SepsisDocument18 pagesNeuro SepsisRed DevilNo ratings yet
- Asthma Treatment MART Regime Guidance HMMC 102018Document1 pageAsthma Treatment MART Regime Guidance HMMC 102018Red DevilNo ratings yet
- Pi Is 0012369216412146Document3 pagesPi Is 0012369216412146Red DevilNo ratings yet
- Practice Exam: Https://learnuw - Wisc.edu/ (Requires Log In) 2. Practice OSCE Scenarios (Below)Document20 pagesPractice Exam: Https://learnuw - Wisc.edu/ (Requires Log In) 2. Practice OSCE Scenarios (Below)Red Devil100% (1)
- Premedicantdrugs1 170216071329Document49 pagesPremedicantdrugs1 170216071329Sagar BhardwajNo ratings yet
- Practice Exam: Https://learnuw - Wisc.edu/ (Requires Log In) 2. Practice OSCE Scenarios (Below)Document20 pagesPractice Exam: Https://learnuw - Wisc.edu/ (Requires Log In) 2. Practice OSCE Scenarios (Below)Red DevilNo ratings yet
- Health Statistics Report 2019Document147 pagesHealth Statistics Report 20197063673nasNo ratings yet
- Asthma Treatment MART Regime Guidance HMMC 102018Document1 pageAsthma Treatment MART Regime Guidance HMMC 102018Red DevilNo ratings yet
- Pi Is 0012369216412146Document3 pagesPi Is 0012369216412146Red DevilNo ratings yet
- Short Version of Draft Guideline 3Document14 pagesShort Version of Draft Guideline 3Red DevilNo ratings yet
- CKD Stages, Causes, Symptoms and TreatmentDocument40 pagesCKD Stages, Causes, Symptoms and Treatmentandi hikmasharyNo ratings yet
- Daftar Pustaka Penyakit Ginjal KronikDocument3 pagesDaftar Pustaka Penyakit Ginjal KronikArifaAlkafNo ratings yet
- Facebook Faqs Website Faqs (Included) : Laboratory / Radiology InquiriesDocument13 pagesFacebook Faqs Website Faqs (Included) : Laboratory / Radiology InquiriesChristian SanchezNo ratings yet
- Empanelled HospitalsDocument14 pagesEmpanelled HospitalsSwaroopVishnuNo ratings yet
- Guidelines NephrologyDocument1 pageGuidelines NephrologyVicky HadiNo ratings yet
- MSU11011Document8 pagesMSU11011Michael TarverNo ratings yet
- Robbins Ch. 20 The Kidney Review QuestionsDocument10 pagesRobbins Ch. 20 The Kidney Review QuestionsPA2014100% (4)
- Wiley Journal APCs Open AccessDocument216 pagesWiley Journal APCs Open AccessLupi YudhaningrumNo ratings yet
- Nephrotic Vs Nephritic SyndromeDocument80 pagesNephrotic Vs Nephritic Syndromevan016_bunnyNo ratings yet
- Pathophysio Chronic GlomerulonephritisDocument1 pagePathophysio Chronic GlomerulonephritisRan Ma100% (1)
- Definition and Criteria For CKDDocument2 pagesDefinition and Criteria For CKDalejandraNo ratings yet
- Renal Diseases - BSMLS OLFUDocument15 pagesRenal Diseases - BSMLS OLFUMitch IbayNo ratings yet
- What Is Glomerulonephritis?Document7 pagesWhat Is Glomerulonephritis?SSNo ratings yet
- The PRISMAFLEX System: Making Possible PersonalDocument12 pagesThe PRISMAFLEX System: Making Possible PersonalluisfulaNo ratings yet
- CNEMU-VI: Celebes Nephro-Endo Metabolic UpdateDocument1 pageCNEMU-VI: Celebes Nephro-Endo Metabolic UpdateMagfira Al HabsyiNo ratings yet
- Pregnancy CKDDocument6 pagesPregnancy CKDRajiv MedankiNo ratings yet
- The Kidney Disease Solution PDF Free Download The Kidney Disease Solution PDF Free Download PDFDocument9 pagesThe Kidney Disease Solution PDF Free Download The Kidney Disease Solution PDF Free Download PDFRadoth Reagen SihombingNo ratings yet
- Daftar PustakaDocument3 pagesDaftar Pustakasari murnaniNo ratings yet
- Bootcamp's Step 1 Study ScheduleDocument8 pagesBootcamp's Step 1 Study ScheduleGlorivy E. Mora GonzalezNo ratings yet
- Hospital Paneld 18 November 20191 PDFDocument88 pagesHospital Paneld 18 November 20191 PDFHarish prajapatNo ratings yet
- Nephrotic Syndrome: Diagnosis and ManagementDocument5 pagesNephrotic Syndrome: Diagnosis and Managementchloe1411No ratings yet
- CCHT Prep GuideDocument18 pagesCCHT Prep GuideAmmar YasserNo ratings yet
- Design and construction of dialysis unitsDocument4 pagesDesign and construction of dialysis unitsRidho Wahyutomo100% (1)
- Nephrology Module: 2007/8 Curriculum: Year 4 & 5 Undergraduate MedicineDocument7 pagesNephrology Module: 2007/8 Curriculum: Year 4 & 5 Undergraduate MedicineemmaNo ratings yet
- Administration of Intravenous Iron SucroseDocument7 pagesAdministration of Intravenous Iron SucroseCristian MuñozNo ratings yet
- Introduction To Medical Terminology: Dr. Jill Villarreal Harris-Stowe State University Spring 2019Document44 pagesIntroduction To Medical Terminology: Dr. Jill Villarreal Harris-Stowe State University Spring 2019Lia LNo ratings yet
- FCM3-3.03 Renal Disease Control ProgramDocument10 pagesFCM3-3.03 Renal Disease Control ProgramJoher MendezNo ratings yet
- Hubungan Lama Menjalani Hemodialisa Dengan Tingkat Stres Pada Pasien Gagal Ginjal Kronik Di Rsud Bendan Kota PekalonganDocument6 pagesHubungan Lama Menjalani Hemodialisa Dengan Tingkat Stres Pada Pasien Gagal Ginjal Kronik Di Rsud Bendan Kota PekalonganYuni SumarianiNo ratings yet
- MKSAP 19 (Medical Knowledge Self-Assessment Program) Nephrology (American College of Physicians) (American College of Physicians)Document195 pagesMKSAP 19 (Medical Knowledge Self-Assessment Program) Nephrology (American College of Physicians) (American College of Physicians)Emin bojecNo ratings yet
- Hubungan Management Cairan Dengan Tipe Sindrom Nefrotik Pada AnakDocument6 pagesHubungan Management Cairan Dengan Tipe Sindrom Nefrotik Pada AnakTitis HandayaniNo ratings yet